

Volume 8, Issue 1 (Continuously Updated 2025)
Func Disabil J 2025, 8(1): 0-0 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Emmanuel G, Nadasan T, Olagbegi O. Work-related Musculoskeletal Disorder Among Physiotherapists in Sub–Saharan Africa: A Scoping Review. Func Disabil J 2025; 8 (1)
URL: http://fdj.iums.ac.ir/article-1-343-en.html
URL: http://fdj.iums.ac.ir/article-1-343-en.html
Work-related Musculoskeletal Disorder Among Physiotherapists in Sub–Saharan Africa: A Scoping Review



1- Department of Physiotherapy, Olabisi Onabanjo University Teaching Hospital, Sagamu, Nigeria. , emmanuelgrace345@yahoo.com
2- Discipline of Physiotherapy, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
2- Discipline of Physiotherapy, Faculty of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
Full-Text [PDF 917 kb]
(63 Downloads)
| Abstract (HTML) (166 Views)
Full-Text: (37 Views)
Introduction
Work-related musculoskeletal disorders (WRMSDs) are injuries or pain in the musculoskeletal system, resulting from repetitive tasks, awkward postures, or excessive physical exertion during work [1]. These disorders constitute a significant occupational health hazard globally, especially among healthcare professionals, such as physiotherapists. The physical demands of manual therapy, prolonged static postures, and repetitive movements put physiotherapists at higher risk of WRMSDs than other healthcare professionals [1–3].
Global studies on WRMSDs show that up to 90% of physiotherapists develop WRMSDs at various points in their careers, with the lower back, neck, and shoulders being the most commonly affected body areas [4–6].
There is limited evidence from sub-Saharan Africa (SSA) regarding the prevalence and risk factors associated with WRMSDs among physiotherapists, which have been extensively studied in high-income countries [5, 7–9].
The challenges faced by physiotherapists in this region include limited resources, high workloads, and diverse work environments, which may aggravate the burden of WRMSDs in this population, underscoring the need to consider the prevalence, associated risk factors, and prevention strategies in the sub-Saharan context [2, 3, 10]
The health of physiotherapists is critical to ensure quality patient care and maintaining a sustainable workforce because they play a crucial role in providing rehabilitation care, particularly in low- and middle-income countries where access to specialist care is limited [11]. Understanding the burden of WRMSDs among physiotherapists in SSA is essential to develop targeted interventions and inform occupational health policies [12].
This scoping review aimed to map and synthesize the existing evidence on WRMSDs among physiotherapists in SSA, focusing on prevalence, pattern, effects and methods of mitigating WRMSDs among physiotherapists in the region. In addition, this review aimed to reduce the burden of WRMSDs in this region by identifying research gaps and providing a basis for future research.
Materials and Methods
A scoping review was conducted following the methodological framework of the Joana Briggs Institute guidelines. In accordance with this framework, the five steps used were: Identifying the research question; identifying relevant studies; study selection; charting the data; and collating, summarizing, and reporting the results.
Identification of the research question
The overall aim of the study underpinning the scoping review was to determine the efficacy of an educational program for mitigating WRMSDs among physiotherapists in southwest Nigeria
They were specifically identified as follows:
1) What is the framework of prevalence of WRMSDs among physiotherapists in SSA? 2) What are the patterns of WRMSDs among this population? 3) What are the effects of WRMSDs among SSA physiotherapists? 4) What are the methods used to mitigate WRMSDs among physiotherapists in SSA.
The population, concept, and context framework was used to define the eligibility criteria for the studies for the primary research question. The population included physiotherapists. The concept is on WRMSDs, while the context is within SSA.
Identifying relevant studies
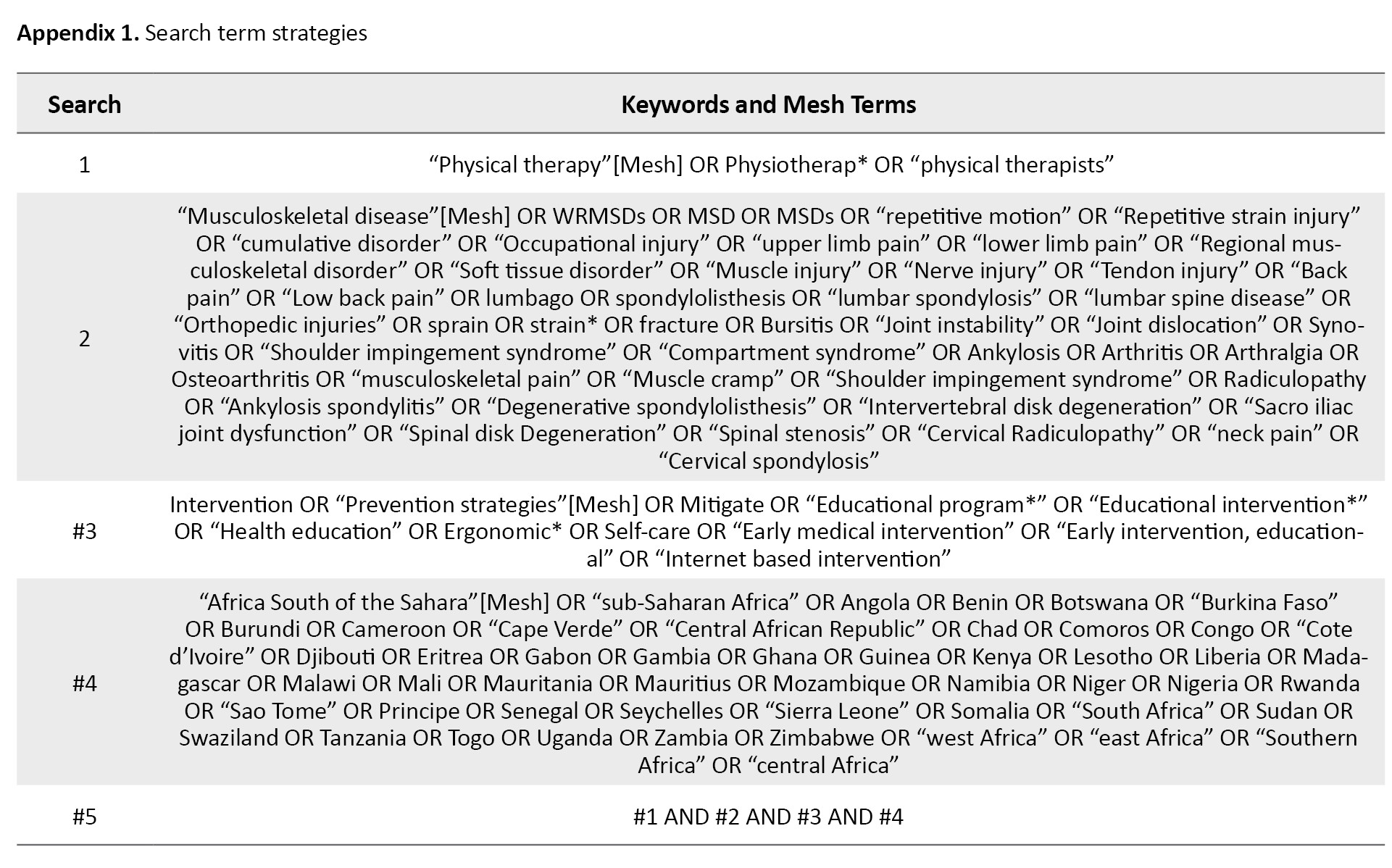
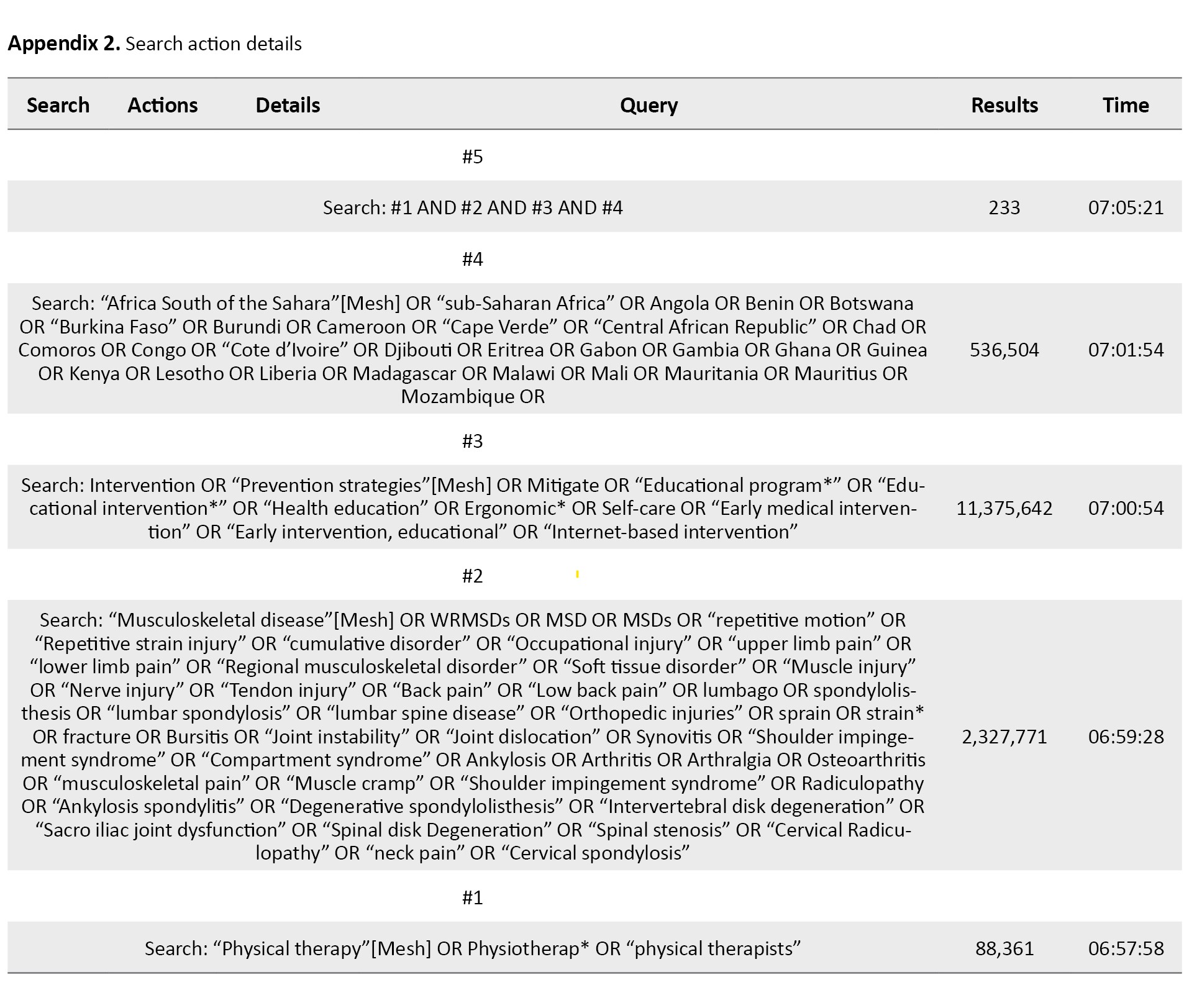
The following electronic databases were used to conduct a search for literature: PubMed, Cochrane Library, Web of Science, and Scopus; the search was from 2005 to November 2024. A search strategy was conducted using the following keywords: ‘physiotherapy’, ‘physical therapy’, ‘physiotherapist’, ‘musculoskeletal disorder,’ ‘Intervention’, ‘SSA’. The Boolean terms ‘AND’, ‘OR,’ and ‘NOT’ were used to separate keywords. An expert librarian at the University of KwaZulu-Natal was consulted during the literature search (Appendices 1 and 2).
Rayyan reference manager was used to manage all the citations.
Eligibility criteria
Inclusion and exclusion criteria were developed to identify key areas of interest.
The inclusion criteria included studies published in peer-reviewed journals, written in English, from 2005 to November 2024, both qualitative and quantitative studies assessing the effectiveness, outcomes, challenges, and best practices of these programs. Also, grey literature, conference abstracts, editorials, letters, and reference lists. The exclusion criteria included studies not directly related to physiotherapists, studies focusing solely on treatment rather than prevention, articles not in the English language, and articles published before 2005.
Study selection
Eligible articles were identified and uploaded to Rayyan, and all duplicate articles were removed. Two independent reviewers screened the titles and abstracts, and the full texts of retrieved articles relevant to the research objectives. A third reviewer screened any excluded citations and resolved any differences between the two reviewers to make a final decision. The library service at the University of KwaZulu-Natal was used to access full-text articles from non-open-access publications.
Charting the data
Relevant data from the included articles were extracted using a piloted Google Form to corroborate the study characteristics and their relevance. The data charting form was regularly updated to include new information that addressed the research question. The following variables were extracted from included studies: Author name(s), publication date, study title, study design, study setting, population, number of males and females, patterns/anatomical distributions, effects, and coping strategies.
Collating, summarizing, and reporting the results
Thematic content analysis was used to analyze the narrative accounts derived from the included studies. Data were extracted on the prevalence, patterns, effects, and methods of WRMSDS mitigation among physiotherapists. The results of this proposed study are presented according to the preferred reporting items for systematic reviews and meta-analysis: Extension for scoping review (PRISMA-ScR) [13].
Results
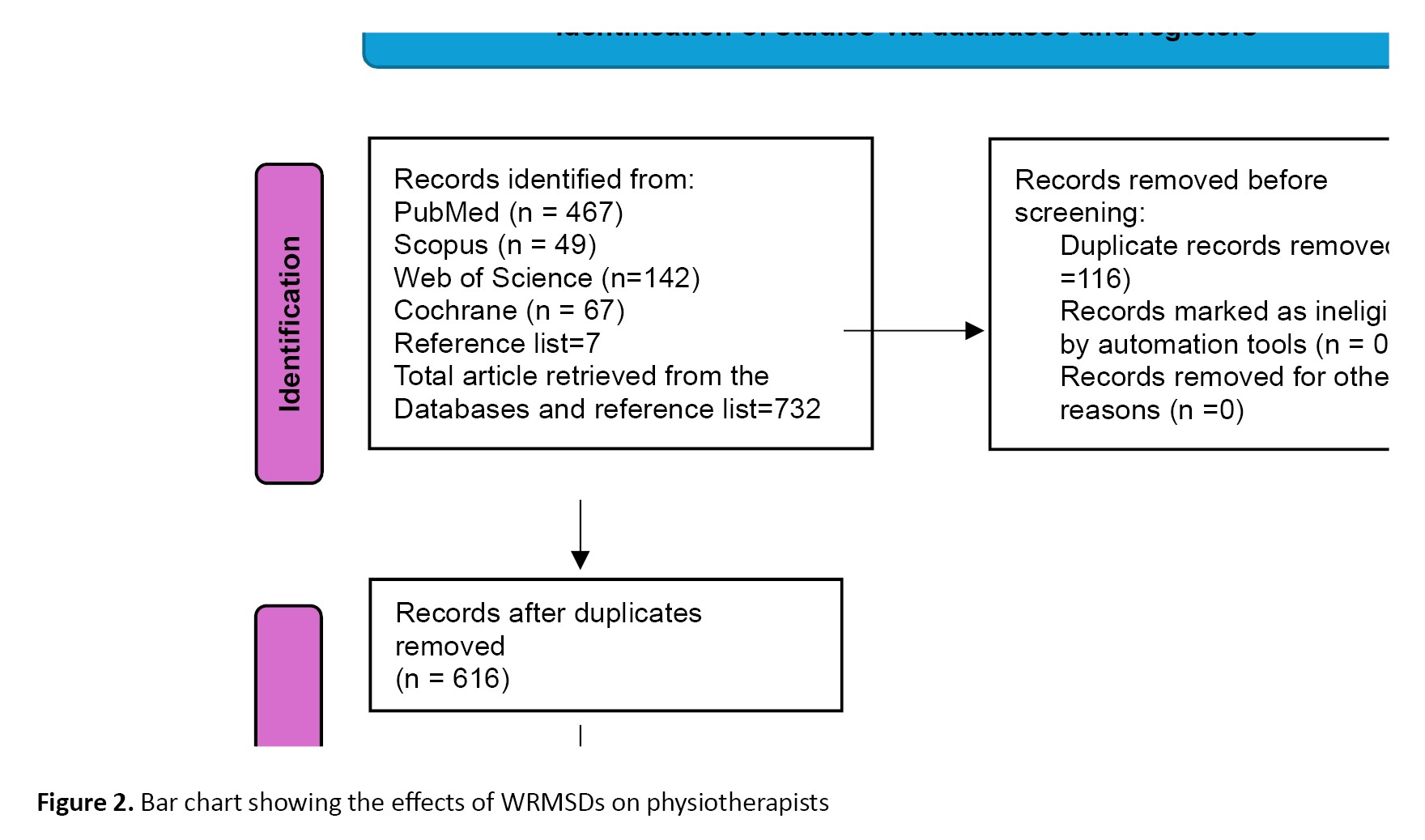
A total of 732 eligible studies (Cochrane-57, Scopus-49, Web of Science-142, PubMed-467, reference list-7) were identified from the databases and reference lists (Figure 1).
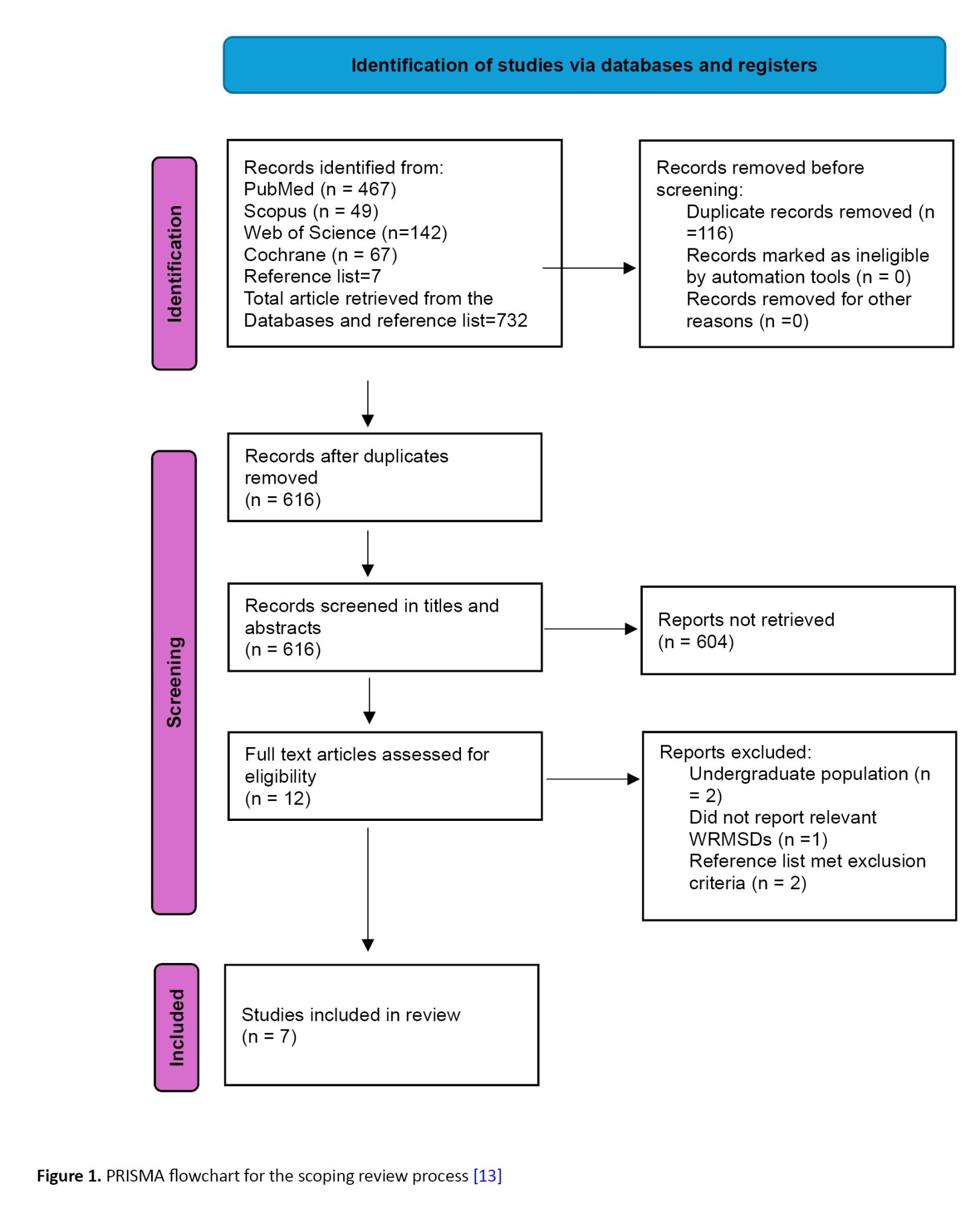 After duplicate removal and title screening of articles from the databases, 609 studies were selected for the review. Thereafter, abstract screening was conducted, of which 604 studies were excluded for not meeting the inclusion criteria, thus reducing the eligible articles for screening to 5 articles. After the full-article screening, three studies were excluded for the following reasons: Two of those three studies made a report on undergraduate students [14, 15], and one study did not report on the prevalence, pattern effect, and method of mitigation of WRMSDs [16] leaving only two [10, 12] eligibly for data extraction. Also, two references [17, 18] out of the seven studies obtained from the reference lists were excluded for not meeting the inclusion criteria, leaving five studies [2, 3, 19–21] that met the inclusion criteria and were included from the reference lists. Ultimately, seven articles were included in the review for data extraction, as they met our inclusion criteria (Table 1).
After duplicate removal and title screening of articles from the databases, 609 studies were selected for the review. Thereafter, abstract screening was conducted, of which 604 studies were excluded for not meeting the inclusion criteria, thus reducing the eligible articles for screening to 5 articles. After the full-article screening, three studies were excluded for the following reasons: Two of those three studies made a report on undergraduate students [14, 15], and one study did not report on the prevalence, pattern effect, and method of mitigation of WRMSDs [16] leaving only two [10, 12] eligibly for data extraction. Also, two references [17, 18] out of the seven studies obtained from the reference lists were excluded for not meeting the inclusion criteria, leaving five studies [2, 3, 19–21] that met the inclusion criteria and were included from the reference lists. Ultimately, seven articles were included in the review for data extraction, as they met our inclusion criteria (Table 1).
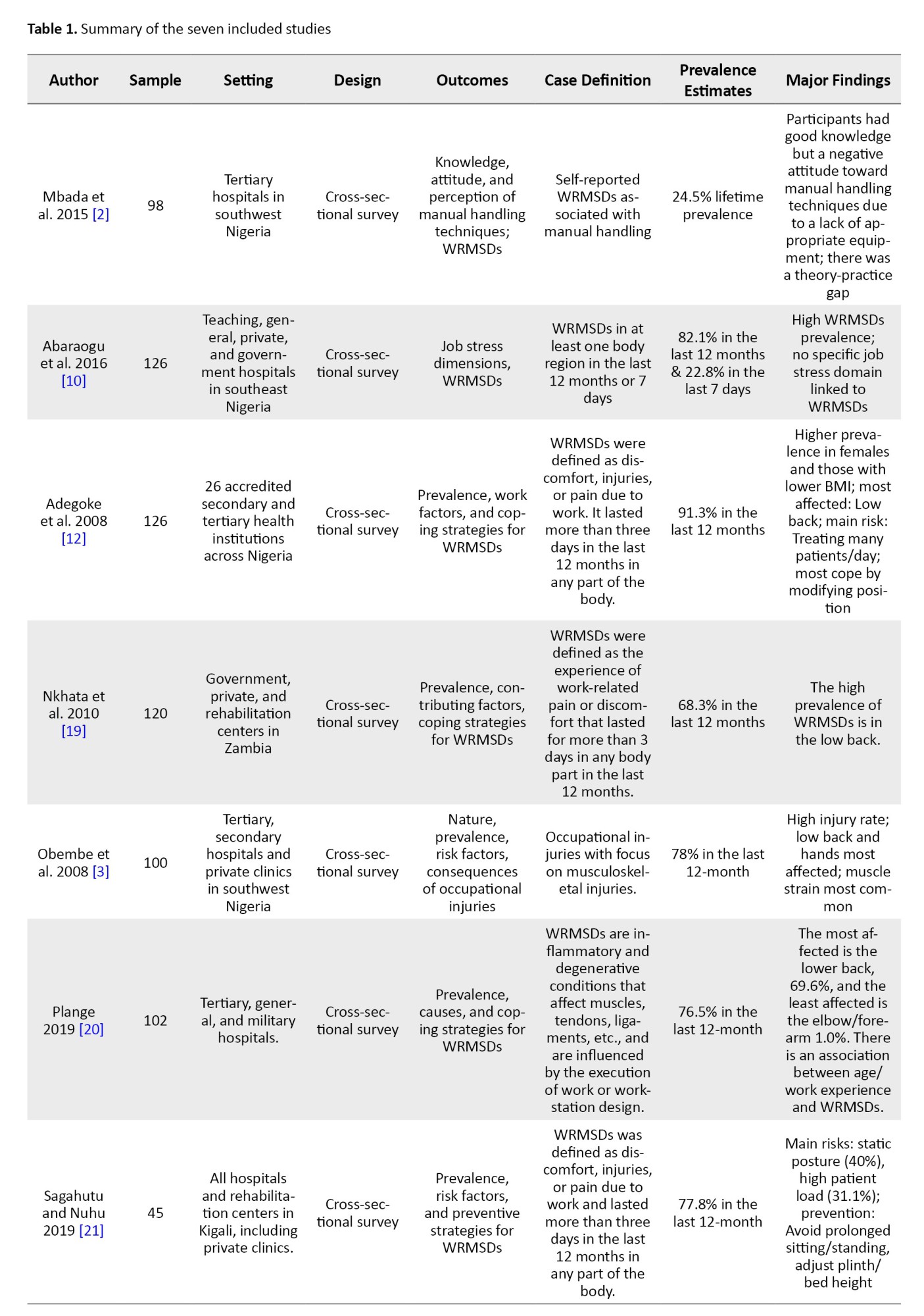
Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart for the screening and selection of studies in this review (Table 1 and Figure 1).
Characteristics of the included studies
A total of 7 published articles between 2005 and 2024 were found eligible for inclusion in our scoping review. The included studies were conducted in different hospital settings, and the population was drawn from male and female physiotherapists.
In this study, 57.1% (4/7) of the included studies were conducted in Nigeria [2, 3, 10, 12] while other studies were from Gambia [19], Ghana [20], and Rwanda [21]. A total of 717 participants included in the included studies.
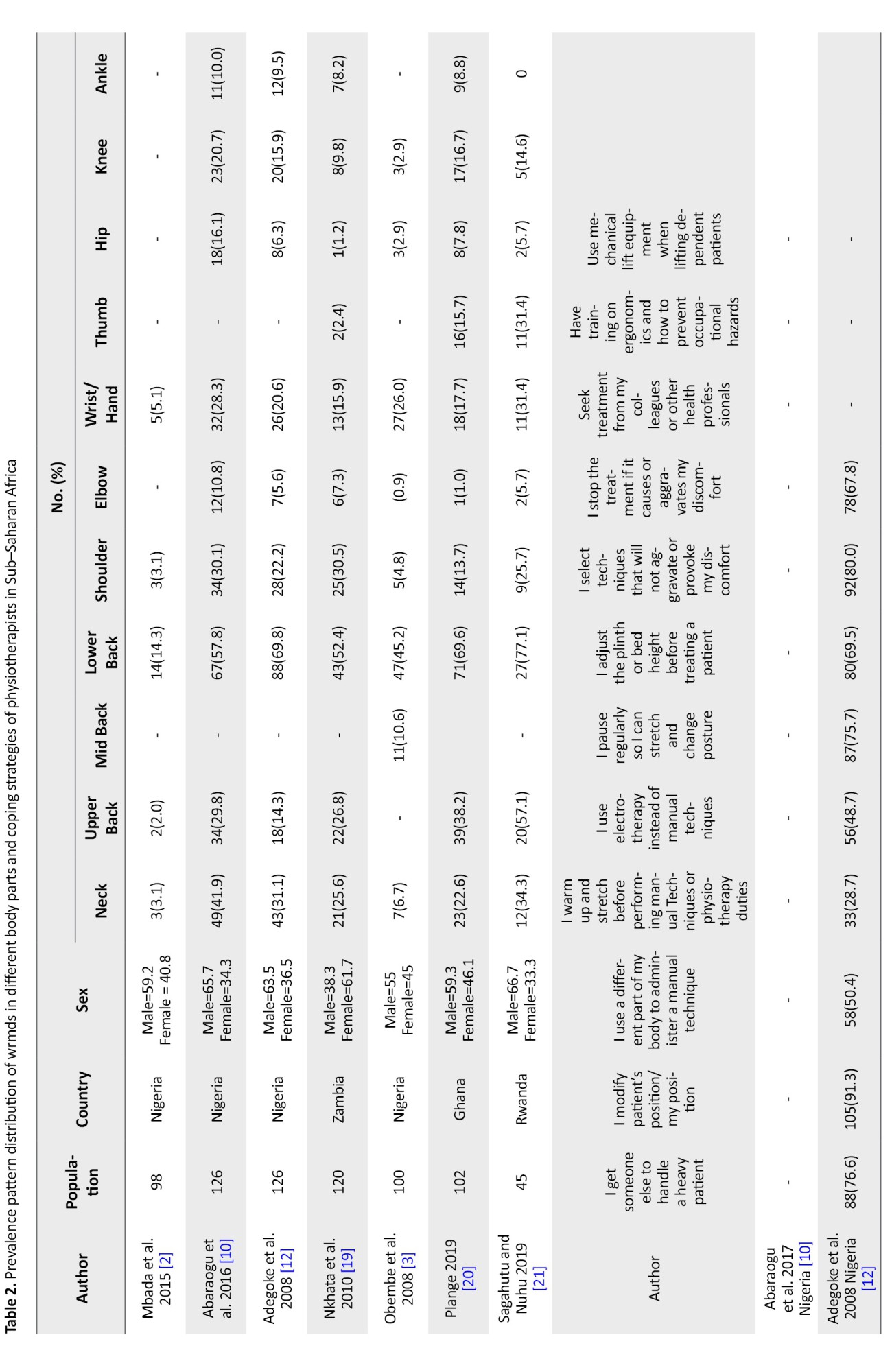
All 7 included studies were cross-sectional surveys. Of the seven included studies, all of them, as presented in Table 1, showed evidence on the prevalence and pattern of WRMSDs among physiotherapists [2, 3, 10, 12, 19–21]. Only one of the studies provided evidence on effect of WRMSDs [12], and four described coping strategies or methods to mitigate WRMSDs [12, 19–21] (Figure 2 and Table 2).
Gender distribution
Gender distribution varied across studies, though in most samples, male physiotherapists constituted the majority, such as in Adegoke et al. (63.5% male) [12] and Abaraogu et al. (65.7% male) [10], while some, such as Nkhata et al. [19], reported a predominantly female workforce (61.7%).
Prevalence/pattern and anatomical distribution of WRMSDs
There was a high prevalence of WRMSDs among physiotherapists across the SSA studies included in this scoping review. Although this prevalence was not consistently reported as single percentage values across studies, anatomical site-specific prevalence figures provide a reliable estimate of the widespread nature of these disorders among physiotherapists in the region.
Based on the anatomical distribution of WRMSDs, our findings revealed that the lower back is the most affected region among physiotherapists in SSA. The reported prevalence rates were 69.6% [18], 77.1% [19], and 69.8% [12]. Similarly, Nkhata et al. [19] found that 52.4% of physiotherapists in Zambia reported lower back symptoms.
Neck and upper back pain were the next most commonly reported symptoms. In Abaraogu et al. [10] study, neck pain was reported to be 41.9% while in Sagahutu and Nuhu's study, there was a prevalence rate of 34.3% [21]. Meanwhile, a higher prevalence rate of upper back pain was reported in Sagahutu and Nuhu (57.1%) [21] and Plange (38.2%) [20]. These results underscore a recurrent theme across studies: concentrated musculoskeletal strain in regions heavily involved in manual therapy and patient handling.
Upper back symptoms were also common, with a higher percentage of samples observed in Sagahutu and Nuhu (57.1%) [21], followed by plange at 38.2% [20]. A moderate prevalence rate of musculoskeletal complaints was reported for the shoulder, wrist/hand, and thumb. For instance, wrist/hand symptoms were reported to be 28.3% in Abaraogu et al. [10] and 31.4% in Sagahutu and Nuhu [21]. In comparison, shoulder discomfort was reported to be 30.5% of respondents in Nkhata et al. [19] and 30.1% in Abaraogu et al. [10].
Distal upper limb symptoms were extensively reported in the wrist/hand and thumb. For example, wrist/hand disorders were reported to be 31.4% [21] in Sagahutu and Nuhu's sample and 28.3% [10] in Abaraogu's et al. A less commonly reported symptom site is thumb strain. However, there was a high prevalent rate of this in Sagahutu and Nuhu at 31.4% [21]. In Plange at 15.7% [20], this could probably be due to repetitive manual therapy practices, such as joint mobilizations and manipulations when handling patients.
Symptoms in the lower limbs (hip, knee, and ankle) were rarely reported, yet significant. Abaraogu et al. [10] indicated that 16.1% of participants experienced hip pain and 20.7% had knee pain. Plange similarly noted a 16.7% [20] prevalence of knee pain, while the Sagahutu and Nuhu [21] study documented no cases of lower ankle involvement (0%) but observed a higher incidence of knee involvement (14.6%) [21]. Overall, these prevalence patterns underscore the physically demanding nature of physiotherapy in these contexts and the strain placed on various anatomical regions during clinical practice.
Effects of WRMSDs
Despite the high prevalent rate and widespread distribution of WRMSDs among physiotherapists, most remained in the profession or changed their area of practice. According to a study by Adegoke et al. a greater percentage (62.6%) of physiotherapists modifies or changes their treatment techniques due to the effect of WRMSDs. However, despite these health challenges, 88.4% did not change their area of specialization, and 87.0% remained in the profession (Figure 2). This may be because each physiotherapist loves the area of practice in which they specialize. Furthermore, these results highlight the professional resilience of physiotherapists in SSA. However, they also pinpoint the potential risk of ongoing physical strain if adequate interventions and institutional support are deficient [12].
When it comes to coping mechanisms in the case of WRMSDs, physiotherapists mainly modify their clinical practice settings rather than withdrawing from the profession, adapting their techniques or work routines to accommodate the various discomforts experienced or to reduce the risk of further injury. Nevertheless, the implications of persistent WRMSDs, such as reduced quality of care, absenteeism, and long-term disability, remain underreported and warrant further longitudinal research.
Coping strategies and methods of mitigation
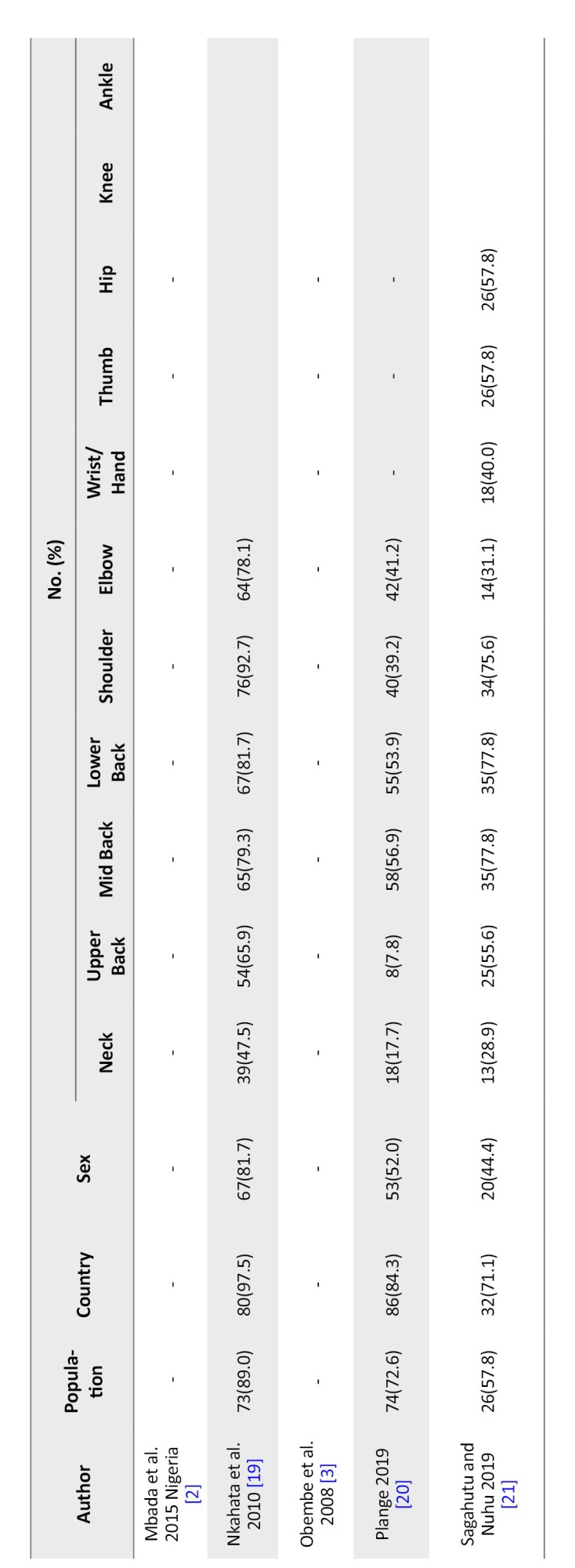
Physiotherapists adopted numerous strategies to mitigate the impact of WRMSDs (Table 2). The most common strategy across multiple studies was modifying patient or therapist position, reported by 97.5% of respondents in Nkhata [19], 91.3% in Adegoke et al. [12], 84.3% in Plange [20], and 71.1% in Sagahutu and Nuhu [21]. This high incidence rate reflects an immediate and practical adaptation that can be implemented during treatment to reduce physical strain.
Another prevalent coping strategy was pausing regularly to stretch or change posture. This was reported by 79.3% in Nkhata et al. [19], 75.7% in Adegoke et al. [12], 77.8% in both Plange [20] and Sagahutu et al. [21], stressing the recognition of microbreaks as a means to prevent prolonged musculoskeletal load.
Adjusting the treatment plinth or bed's height was also frequently reported, with 81.7% [19], 69.5% [12], and 77.8% [21] employing this strategy. This adjustment reduces awkward postures and the risk of cumulative musculoskeletal trauma.
Selection of procedures that minimize discomfort was another frequently employed strategy. For example, 92.7% of physiotherapists in Nkhata et al. [19] and 80.0% in Adegoke et al. [12] reported adapting their techniques to prevent exacerbation of pain. Also, 78.1% [19], 67.8% [12], and 31.1% reported stopping treatment when discomfort arises [21].
Adoption of alternative techniques such as electrotherapy in place of manual therapy was less often reported, with only 7.8% of respondents in Plange [20] and 48.7% in Adegoke et al. [12] indicating such substitutions.
Getting assistance from colleagues for handling heavy patients was reported by 76.6% [12], 89.0% [19], 72.6% [20], and 57.8% [21], revealing interprofessional cooperation as a significant mitigation method. Warming up or stretching before duty was less consistently reported, with only 28.7% [12] and 47.5% [19] using such preventive measures.
Sagahutu and Nuhu's study was the only one to report ergonomic training and occupational hazard prevention, with 57.8% receiving such training. Also, mechanical lifting equipment was reported by only 57.8% in the same study, suggesting limited institutional support or infrastructure for ergonomic practice [21].
Formal treatment interventions, such as seeking treatment from colleagues or health professionals, were reported by only 40.0% [21], indicating a relatively low uptake of such services, possibly due to lack of accessible care, cultural norms, or workload.
Discussion
This scoping review explored evidence from seven studies conducted across SSA on the prevalence, anatomical distribution, effects, and coping strategies associated with WRMSDs among physiotherapists. The findings reiterate the extensive physical toll of clinical physiotherapy practice in this region, reflecting global trends while also revealing region-specific patterns fashioned by systemic, cultural, and infrastructural factors.
Prevalence and Anatomical Distribution of WRMSDs
The included studies corroborate findings from international literature that WRMSDs were highly prevalent among physiotherapists in the region. There is consistently high reported WRMSD prevalence among physiotherapists globally, often exceeding 80% annually [5, 6, 10]. Similarly, the present review found widespread musculoskeletal symptoms, with the lower back being the most affected anatomical region. The prevalence of lower back pain ranged from 14.3% [2] to 77.1% [21], aligning with the 50%–80% range reported by physiotherapists in other regions except the lowest range [4–6, 22]. The varied prevalence reported by the included studies may be due to differences in methodologies and WRMSD case definitions. Only three studies have similar case definitions, while the remaining studies have varied in their definitions.
The predominance of lower back, neck, and upper back pain exacerbates the ergonomic challenges inherent in patient handling, prolonged static postures, and manual therapy, which are fundamental components of physiotherapy. These anatomical patterns are consistent with findings from studies in Europe and Asia [4, 6], indicating that, despite contextual differences, the physical demands of physiotherapy universally predispose practitioners to spinal WRMSDs.
Commonly reported in the review of upper limb symptoms (e.g. wrist/hand and thumb pain) were marked by [21] and [10]. The findings support previous international research emphasizing that manual therapy techniques, repetitive tasks, and sustained grip force contribute significantly to upper extremity strain among physiotherapists [5, 6]. Additionally, the prominence of thumb disorders in [21] (31.4%) reflects similar reports in American and Asia contexts, where joint mobilizations and manipulations are routine practice [5, 23].
Lower limb symptoms, though less frequently reported, were still evident in non-negligible proportions (e.g. 16.1% for hip pain and 20.7% for knee pain [10]). This likely results from prolonged standing and dynamic movement during therapy sessions. However, unlike the high burden of spinal and upper limb WRMSDs, lower limb symptoms may reflect more generalized musculoskeletal fatigue rather than work-specific mechanisms. This result was also observed among Egyptian physiotherapists [22].
Gender and professional distribution
Across the studies, gender distribution varied, with some reporting a male-dominated sample [10, 12] and others signifying a female majority [19]. While this disparity may reflect employment patterns within the establishment or national workforce demographics, previous studies have identified gender as a possible risk factor for WRMSDs. Female physiotherapists have been found to report higher WRMSDs prevalence, due to differences in muscle mass, height, ergonomic fit of tools, and job assignments [12]. However, there is a limitation in the direct interpretation of sex-related risks in this context because gender-specific WRMSD analyses were not consistently separated in the reviewed studies.
A reflection of the predominance of inpatient and outpatient clinical practice was observed across all included studies, which were cross-sectional surveys conducted in hospital settings among the physiotherapy workforce in SSA. This clinical setting is vastly essential, as hospital-based physiotherapy often involves time-sensitive workloads, intensive manual therapy and rehabilitation of dependent patients, which are all contributory to cumulative physical stress in the profession [2, 16].
Effects of WRMSDs on professional practice
In a study by Adegoke et al. only a few physiotherapists were reported to have left the profession or changed their area of specialization, despite the high prevalence of WRMSDs. The author further noted that there is a high degree of professional resilience, with 87% of respondents remaining in the profession and 88.4% retaining their specialization [12]. These findings are inconsistent with a study by Khairy et al. among Egyptian physiotherapists, where a greater number (40%) were willing to leave their work because of the high prevalence of WRMSDs [22].
However, it was reported that 62.6% of participants in Adegoke et al.’s study modified and adjusted their treatment techniques due to musculoskeletal symptoms [12]. There is a great deal of adaptability in clinical practice which is found to be common among healthcare workers with WRMSDs, despite the fact that it can lead to suboptimal therapeutic delivery, reduced clinical confidence, and increased cognitive burden, which in turn can affect treatment outcomes [1, 20, 22]. Moreover, the long-term sustainability of continued practice under physical duress is questionable, particularly in resource-constrained systems where workforce shortages may inhibit the redistribution of physically intensive duties. WRMSDs have several occupational consequences. In most reviewed studies, data on the broader professional repercussions of WRMSDs, such as productivity loss, absenteeism, economic cost, and burnout were remarkably omitted. This lapse mirrors a gap in sub-Saharan occupational health research and confines the scope of understanding the systemic effects of WRMSDs.
Coping strategies and mitigation methods
The methods of mitigation adopted by physiotherapists in SSA reflect those recommended in international ergonomic and occupational health guidelines [7, 8, 16]. A universally most prominent reported strategy to cope with WRMSDs was modifying therapist or patient position, with uptake of over 70% in all four studies addressing coping strategies [12, 19–21]. This strategy is supported by the literature, showing that small ergonomic changes, such as repositioning the patient closer or adjusting hand positioning, can significantly reduce biomechanical load [24]. This shows the importance of ergonomic adjustments in workplaces to reduce the negative impact of WRMSDs and enhance productivity and outcomes.
Other coping strategies were also practiced extensively, such as adjusting plinth height, regular microbreaks, and technique modification. These are consistent with preventive frameworks that emphasize task variability and posture alternation to reduce cumulative strain [1, 25]. For instance, studies from Europe and North America show that stretching and posture shifts during treatment have been associated with decreased WRMSD symptoms [5, 24].
However, various vital interventions, such as mechanical lifting devices or ergonomic training, were less frequently reported. This shows limited institutional investment in WRMSD prevention infrastructure, as only one [21] documented its use. These dissimilarities are higher-income settings, where regular ergonomic assessments and access to lifting equipment are often embedded in physiotherapy departments [24].
According to Sagahutu and Nuhu, there is a relatively low rate of physiotherapists (40%) seeking professional treatment for WRMSDs [21]. This is similar to the report from Egypt, where 38.6% physiotherapists consulted a physician for their WRMSDs [22]. This may reflect accessibility, cultural, or financial barriers. Self-care and informal peer consultation may be preferred in some sub-Saharan settings, due to distrust of institutional systems or fear of professional stigma. These results underscore the need for workplace health promotion and confidential reporting pathways to reassure physiotherapists to seek care without fear of reprisal.
Recommendations for practice and policy for low-resource clinical settings
To reduce the incidence and impact of WRMSDs among physiotherapists in SSA, the following recommendations are proposed based on this review:
Integration of Ergonomics Training: Ergonomics should be incorporated into both undergraduate and postgraduate physiotherapy curricula, as well as through continuing professional development [24].
Policy development: Prevention guidelines, mandating periodic workplace safety assessments, and enforcement of occupational health legislation can be developed by national professional bodies and ministries of health to mitigate the effects of WRMSDs.
Promoting a safety culture: Encouraging early reporting, reducing stigma, and fostering collaborative support systems can help mitigate emotional impacts and facilitate timely intervention.
Establish “lift teams” to assist with heavy lifting, promote on-site fitness and stretching programs, and optimize workload management by balancing demanding tasks with less intense activities. The use of low-cost assistive aids, such as gait belts and friction-reducing sheets, should be encouraged. Additionally, fostering a culture of peer support and early reporting of discomfort can facilitate preventive care and help mitigate long-term issues.
Recommendations for practice and policy in high-resource clinical settings
To reduce the incidence and impact of WRMSDs among physiotherapists in SSA, the following recommendations are proposed based on this review:
1) Incorporate occupational health and safety and ergonomics into facility design and integration of ergonomics training: When constructing new facilities or remodeling existing ones, incorporate ergonomic concepts into the design to guarantee sufficient room around beds, suitable floor surfaces, broad doorways, and appropriately positioned fixed equipment. Ergonomics should be incorporated into both undergraduate and postgraduate physiotherapy curricula, as well as through continuing professional development [24]. 2) Institutional Reforms: To reduce exposure to physical stressors, healthcare facilities should invest in lifting equipment, redesigning workspaces to support neutral postures, and instituting job rotation and workload limits. 3) Policy development: Prevention guidelines, mandating periodic workplace safety assessments, and enforcement of occupational health legislation can be developed by national professional bodies and ministries of health to mitigate the effects of WRMSDs.
4) Advanced data gathering and intervention assessment: Make use of resources to carry out thorough research and surveillance on the prevalence and risk factors of WRMSD, using the results to improve and assess the efficacy of preventative measures. 5) Promotion of a safety culture: Promoting early report, reducing stigma, and encouraging collaborative support systems can help mitigate emotional impacts and foster timely intervention. 6) Establish a formal, dedicated safe patient handling (SPH) Program: Create a program with specified guidelines, qualified SPH specialists (also known as “lift-teams”), and the entire array of suitable patient transfer tools (such as ceiling lifts and portable hoists).
7) Required, periodic medical monitoring and fitness-for-work evaluations: Perform routine health and fitness evaluations to spot possible problems early and offer focused assistance or work adjustments.
8. Provide All-Inclusive Support Systems: To guarantee a speedy recovery and return to work following job-related accidents, make occupational health specialists, counseling, and possibly even on-site physiotherapy treatment accessible.
Conclusion
The considerable burden of WRMSDs among physiotherapists in SSA is highlighted by this scoping review, with the lower back, neck, and shoulders most commonly affected. The physical demands of manual therapy, poor ergonomic conditions, and limited access to assistive equipment contribute significantly to the prevalence of WRMSDs. Many physiotherapists adopt self-initiated coping strategies such as modifying posture, delegating tasks, and using electrotherapy, but formal institutional support, including ergonomic training and access to mechanical aids, remains limited. Despite the high incidence of WRMSDs, most physiotherapists continue practicing without changing their specialty or leaving the profession; this may reflect both resilience and the potential for chronic strain-related complications. Structured ergonomic education, policy reforms, and investment in occupational health infrastructure are required to safeguard the well-being and productivity of physiotherapists in the region.
Strengths and limitations of the review
To our knowledge, this is the first scoping review to map the prevalence, patterns, effects, and methods for mitigating WRMSDs among physiotherapists in SSA. This scoping review is not without limitations as the number of studies available from SSA is limited and mainly cross-sectional, restricting causality inference and possible recall bias. In addition, the geographic distribution of studies was uneven, with more than half conducted in Nigeria, potentially skewing region-wide conclusions. Also, language and publication bias may have excluded relevant studies published in non-indexed local journals.
Data availability
Data sharing does not apply to this article as no new data were created or analyzed in this study.
Disclaimer
The views, opinions, assumptions, or any other information presented in this manuscript are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of KwaZulu-Natal, Durban, South Africa.(Code: HSSREC/00007376/2024).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Supervision: Thayananthee Nadasan and Oladapo Olagbegi; Writing the original draft: Grace Emmanuel; Funding acquisition and Resources: Grace Emmanuel; Conceptualization, methodology, investigation, review & editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Badru Oluwaseun, Micheal Ogunlana and Olufemi Oyewole for their assistance in the study.
References
Work-related musculoskeletal disorders (WRMSDs) are injuries or pain in the musculoskeletal system, resulting from repetitive tasks, awkward postures, or excessive physical exertion during work [1]. These disorders constitute a significant occupational health hazard globally, especially among healthcare professionals, such as physiotherapists. The physical demands of manual therapy, prolonged static postures, and repetitive movements put physiotherapists at higher risk of WRMSDs than other healthcare professionals [1–3].
Global studies on WRMSDs show that up to 90% of physiotherapists develop WRMSDs at various points in their careers, with the lower back, neck, and shoulders being the most commonly affected body areas [4–6].
There is limited evidence from sub-Saharan Africa (SSA) regarding the prevalence and risk factors associated with WRMSDs among physiotherapists, which have been extensively studied in high-income countries [5, 7–9].
The challenges faced by physiotherapists in this region include limited resources, high workloads, and diverse work environments, which may aggravate the burden of WRMSDs in this population, underscoring the need to consider the prevalence, associated risk factors, and prevention strategies in the sub-Saharan context [2, 3, 10]
The health of physiotherapists is critical to ensure quality patient care and maintaining a sustainable workforce because they play a crucial role in providing rehabilitation care, particularly in low- and middle-income countries where access to specialist care is limited [11]. Understanding the burden of WRMSDs among physiotherapists in SSA is essential to develop targeted interventions and inform occupational health policies [12].
This scoping review aimed to map and synthesize the existing evidence on WRMSDs among physiotherapists in SSA, focusing on prevalence, pattern, effects and methods of mitigating WRMSDs among physiotherapists in the region. In addition, this review aimed to reduce the burden of WRMSDs in this region by identifying research gaps and providing a basis for future research.
Materials and Methods
A scoping review was conducted following the methodological framework of the Joana Briggs Institute guidelines. In accordance with this framework, the five steps used were: Identifying the research question; identifying relevant studies; study selection; charting the data; and collating, summarizing, and reporting the results.
Identification of the research question
The overall aim of the study underpinning the scoping review was to determine the efficacy of an educational program for mitigating WRMSDs among physiotherapists in southwest Nigeria
They were specifically identified as follows:
1) What is the framework of prevalence of WRMSDs among physiotherapists in SSA? 2) What are the patterns of WRMSDs among this population? 3) What are the effects of WRMSDs among SSA physiotherapists? 4) What are the methods used to mitigate WRMSDs among physiotherapists in SSA.
The population, concept, and context framework was used to define the eligibility criteria for the studies for the primary research question. The population included physiotherapists. The concept is on WRMSDs, while the context is within SSA.
Identifying relevant studies
The following electronic databases were used to conduct a search for literature: PubMed, Cochrane Library, Web of Science, and Scopus; the search was from 2005 to November 2024. A search strategy was conducted using the following keywords: ‘physiotherapy’, ‘physical therapy’, ‘physiotherapist’, ‘musculoskeletal disorder,’ ‘Intervention’, ‘SSA’. The Boolean terms ‘AND’, ‘OR,’ and ‘NOT’ were used to separate keywords. An expert librarian at the University of KwaZulu-Natal was consulted during the literature search (Appendices 1 and 2).
Rayyan reference manager was used to manage all the citations.
Eligibility criteria
Inclusion and exclusion criteria were developed to identify key areas of interest.
The inclusion criteria included studies published in peer-reviewed journals, written in English, from 2005 to November 2024, both qualitative and quantitative studies assessing the effectiveness, outcomes, challenges, and best practices of these programs. Also, grey literature, conference abstracts, editorials, letters, and reference lists. The exclusion criteria included studies not directly related to physiotherapists, studies focusing solely on treatment rather than prevention, articles not in the English language, and articles published before 2005.
Study selection
Eligible articles were identified and uploaded to Rayyan, and all duplicate articles were removed. Two independent reviewers screened the titles and abstracts, and the full texts of retrieved articles relevant to the research objectives. A third reviewer screened any excluded citations and resolved any differences between the two reviewers to make a final decision. The library service at the University of KwaZulu-Natal was used to access full-text articles from non-open-access publications.
Charting the data
Relevant data from the included articles were extracted using a piloted Google Form to corroborate the study characteristics and their relevance. The data charting form was regularly updated to include new information that addressed the research question. The following variables were extracted from included studies: Author name(s), publication date, study title, study design, study setting, population, number of males and females, patterns/anatomical distributions, effects, and coping strategies.
Collating, summarizing, and reporting the results
Thematic content analysis was used to analyze the narrative accounts derived from the included studies. Data were extracted on the prevalence, patterns, effects, and methods of WRMSDS mitigation among physiotherapists. The results of this proposed study are presented according to the preferred reporting items for systematic reviews and meta-analysis: Extension for scoping review (PRISMA-ScR) [13].
Results
A total of 732 eligible studies (Cochrane-57, Scopus-49, Web of Science-142, PubMed-467, reference list-7) were identified from the databases and reference lists (Figure 1).
Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart for the screening and selection of studies in this review (Table 1 and Figure 1).
Characteristics of the included studies
A total of 7 published articles between 2005 and 2024 were found eligible for inclusion in our scoping review. The included studies were conducted in different hospital settings, and the population was drawn from male and female physiotherapists.
In this study, 57.1% (4/7) of the included studies were conducted in Nigeria [2, 3, 10, 12] while other studies were from Gambia [19], Ghana [20], and Rwanda [21]. A total of 717 participants included in the included studies.
All 7 included studies were cross-sectional surveys. Of the seven included studies, all of them, as presented in Table 1, showed evidence on the prevalence and pattern of WRMSDs among physiotherapists [2, 3, 10, 12, 19–21]. Only one of the studies provided evidence on effect of WRMSDs [12], and four described coping strategies or methods to mitigate WRMSDs [12, 19–21] (Figure 2 and Table 2).
Gender distribution
Gender distribution varied across studies, though in most samples, male physiotherapists constituted the majority, such as in Adegoke et al. (63.5% male) [12] and Abaraogu et al. (65.7% male) [10], while some, such as Nkhata et al. [19], reported a predominantly female workforce (61.7%).
Prevalence/pattern and anatomical distribution of WRMSDs
There was a high prevalence of WRMSDs among physiotherapists across the SSA studies included in this scoping review. Although this prevalence was not consistently reported as single percentage values across studies, anatomical site-specific prevalence figures provide a reliable estimate of the widespread nature of these disorders among physiotherapists in the region.
Based on the anatomical distribution of WRMSDs, our findings revealed that the lower back is the most affected region among physiotherapists in SSA. The reported prevalence rates were 69.6% [18], 77.1% [19], and 69.8% [12]. Similarly, Nkhata et al. [19] found that 52.4% of physiotherapists in Zambia reported lower back symptoms.
Neck and upper back pain were the next most commonly reported symptoms. In Abaraogu et al. [10] study, neck pain was reported to be 41.9% while in Sagahutu and Nuhu's study, there was a prevalence rate of 34.3% [21]. Meanwhile, a higher prevalence rate of upper back pain was reported in Sagahutu and Nuhu (57.1%) [21] and Plange (38.2%) [20]. These results underscore a recurrent theme across studies: concentrated musculoskeletal strain in regions heavily involved in manual therapy and patient handling.
Upper back symptoms were also common, with a higher percentage of samples observed in Sagahutu and Nuhu (57.1%) [21], followed by plange at 38.2% [20]. A moderate prevalence rate of musculoskeletal complaints was reported for the shoulder, wrist/hand, and thumb. For instance, wrist/hand symptoms were reported to be 28.3% in Abaraogu et al. [10] and 31.4% in Sagahutu and Nuhu [21]. In comparison, shoulder discomfort was reported to be 30.5% of respondents in Nkhata et al. [19] and 30.1% in Abaraogu et al. [10].
Distal upper limb symptoms were extensively reported in the wrist/hand and thumb. For example, wrist/hand disorders were reported to be 31.4% [21] in Sagahutu and Nuhu's sample and 28.3% [10] in Abaraogu's et al. A less commonly reported symptom site is thumb strain. However, there was a high prevalent rate of this in Sagahutu and Nuhu at 31.4% [21]. In Plange at 15.7% [20], this could probably be due to repetitive manual therapy practices, such as joint mobilizations and manipulations when handling patients.
Symptoms in the lower limbs (hip, knee, and ankle) were rarely reported, yet significant. Abaraogu et al. [10] indicated that 16.1% of participants experienced hip pain and 20.7% had knee pain. Plange similarly noted a 16.7% [20] prevalence of knee pain, while the Sagahutu and Nuhu [21] study documented no cases of lower ankle involvement (0%) but observed a higher incidence of knee involvement (14.6%) [21]. Overall, these prevalence patterns underscore the physically demanding nature of physiotherapy in these contexts and the strain placed on various anatomical regions during clinical practice.
Effects of WRMSDs
Despite the high prevalent rate and widespread distribution of WRMSDs among physiotherapists, most remained in the profession or changed their area of practice. According to a study by Adegoke et al. a greater percentage (62.6%) of physiotherapists modifies or changes their treatment techniques due to the effect of WRMSDs. However, despite these health challenges, 88.4% did not change their area of specialization, and 87.0% remained in the profession (Figure 2). This may be because each physiotherapist loves the area of practice in which they specialize. Furthermore, these results highlight the professional resilience of physiotherapists in SSA. However, they also pinpoint the potential risk of ongoing physical strain if adequate interventions and institutional support are deficient [12].
When it comes to coping mechanisms in the case of WRMSDs, physiotherapists mainly modify their clinical practice settings rather than withdrawing from the profession, adapting their techniques or work routines to accommodate the various discomforts experienced or to reduce the risk of further injury. Nevertheless, the implications of persistent WRMSDs, such as reduced quality of care, absenteeism, and long-term disability, remain underreported and warrant further longitudinal research.
Coping strategies and methods of mitigation
Physiotherapists adopted numerous strategies to mitigate the impact of WRMSDs (Table 2). The most common strategy across multiple studies was modifying patient or therapist position, reported by 97.5% of respondents in Nkhata [19], 91.3% in Adegoke et al. [12], 84.3% in Plange [20], and 71.1% in Sagahutu and Nuhu [21]. This high incidence rate reflects an immediate and practical adaptation that can be implemented during treatment to reduce physical strain.
Another prevalent coping strategy was pausing regularly to stretch or change posture. This was reported by 79.3% in Nkhata et al. [19], 75.7% in Adegoke et al. [12], 77.8% in both Plange [20] and Sagahutu et al. [21], stressing the recognition of microbreaks as a means to prevent prolonged musculoskeletal load.
Adjusting the treatment plinth or bed's height was also frequently reported, with 81.7% [19], 69.5% [12], and 77.8% [21] employing this strategy. This adjustment reduces awkward postures and the risk of cumulative musculoskeletal trauma.
Selection of procedures that minimize discomfort was another frequently employed strategy. For example, 92.7% of physiotherapists in Nkhata et al. [19] and 80.0% in Adegoke et al. [12] reported adapting their techniques to prevent exacerbation of pain. Also, 78.1% [19], 67.8% [12], and 31.1% reported stopping treatment when discomfort arises [21].
Adoption of alternative techniques such as electrotherapy in place of manual therapy was less often reported, with only 7.8% of respondents in Plange [20] and 48.7% in Adegoke et al. [12] indicating such substitutions.
Getting assistance from colleagues for handling heavy patients was reported by 76.6% [12], 89.0% [19], 72.6% [20], and 57.8% [21], revealing interprofessional cooperation as a significant mitigation method. Warming up or stretching before duty was less consistently reported, with only 28.7% [12] and 47.5% [19] using such preventive measures.
Sagahutu and Nuhu's study was the only one to report ergonomic training and occupational hazard prevention, with 57.8% receiving such training. Also, mechanical lifting equipment was reported by only 57.8% in the same study, suggesting limited institutional support or infrastructure for ergonomic practice [21].
Formal treatment interventions, such as seeking treatment from colleagues or health professionals, were reported by only 40.0% [21], indicating a relatively low uptake of such services, possibly due to lack of accessible care, cultural norms, or workload.
Discussion
This scoping review explored evidence from seven studies conducted across SSA on the prevalence, anatomical distribution, effects, and coping strategies associated with WRMSDs among physiotherapists. The findings reiterate the extensive physical toll of clinical physiotherapy practice in this region, reflecting global trends while also revealing region-specific patterns fashioned by systemic, cultural, and infrastructural factors.
Prevalence and Anatomical Distribution of WRMSDs
The included studies corroborate findings from international literature that WRMSDs were highly prevalent among physiotherapists in the region. There is consistently high reported WRMSD prevalence among physiotherapists globally, often exceeding 80% annually [5, 6, 10]. Similarly, the present review found widespread musculoskeletal symptoms, with the lower back being the most affected anatomical region. The prevalence of lower back pain ranged from 14.3% [2] to 77.1% [21], aligning with the 50%–80% range reported by physiotherapists in other regions except the lowest range [4–6, 22]. The varied prevalence reported by the included studies may be due to differences in methodologies and WRMSD case definitions. Only three studies have similar case definitions, while the remaining studies have varied in their definitions.
The predominance of lower back, neck, and upper back pain exacerbates the ergonomic challenges inherent in patient handling, prolonged static postures, and manual therapy, which are fundamental components of physiotherapy. These anatomical patterns are consistent with findings from studies in Europe and Asia [4, 6], indicating that, despite contextual differences, the physical demands of physiotherapy universally predispose practitioners to spinal WRMSDs.
Commonly reported in the review of upper limb symptoms (e.g. wrist/hand and thumb pain) were marked by [21] and [10]. The findings support previous international research emphasizing that manual therapy techniques, repetitive tasks, and sustained grip force contribute significantly to upper extremity strain among physiotherapists [5, 6]. Additionally, the prominence of thumb disorders in [21] (31.4%) reflects similar reports in American and Asia contexts, where joint mobilizations and manipulations are routine practice [5, 23].
Lower limb symptoms, though less frequently reported, were still evident in non-negligible proportions (e.g. 16.1% for hip pain and 20.7% for knee pain [10]). This likely results from prolonged standing and dynamic movement during therapy sessions. However, unlike the high burden of spinal and upper limb WRMSDs, lower limb symptoms may reflect more generalized musculoskeletal fatigue rather than work-specific mechanisms. This result was also observed among Egyptian physiotherapists [22].
Gender and professional distribution
Across the studies, gender distribution varied, with some reporting a male-dominated sample [10, 12] and others signifying a female majority [19]. While this disparity may reflect employment patterns within the establishment or national workforce demographics, previous studies have identified gender as a possible risk factor for WRMSDs. Female physiotherapists have been found to report higher WRMSDs prevalence, due to differences in muscle mass, height, ergonomic fit of tools, and job assignments [12]. However, there is a limitation in the direct interpretation of sex-related risks in this context because gender-specific WRMSD analyses were not consistently separated in the reviewed studies.
A reflection of the predominance of inpatient and outpatient clinical practice was observed across all included studies, which were cross-sectional surveys conducted in hospital settings among the physiotherapy workforce in SSA. This clinical setting is vastly essential, as hospital-based physiotherapy often involves time-sensitive workloads, intensive manual therapy and rehabilitation of dependent patients, which are all contributory to cumulative physical stress in the profession [2, 16].
Effects of WRMSDs on professional practice
In a study by Adegoke et al. only a few physiotherapists were reported to have left the profession or changed their area of specialization, despite the high prevalence of WRMSDs. The author further noted that there is a high degree of professional resilience, with 87% of respondents remaining in the profession and 88.4% retaining their specialization [12]. These findings are inconsistent with a study by Khairy et al. among Egyptian physiotherapists, where a greater number (40%) were willing to leave their work because of the high prevalence of WRMSDs [22].
However, it was reported that 62.6% of participants in Adegoke et al.’s study modified and adjusted their treatment techniques due to musculoskeletal symptoms [12]. There is a great deal of adaptability in clinical practice which is found to be common among healthcare workers with WRMSDs, despite the fact that it can lead to suboptimal therapeutic delivery, reduced clinical confidence, and increased cognitive burden, which in turn can affect treatment outcomes [1, 20, 22]. Moreover, the long-term sustainability of continued practice under physical duress is questionable, particularly in resource-constrained systems where workforce shortages may inhibit the redistribution of physically intensive duties. WRMSDs have several occupational consequences. In most reviewed studies, data on the broader professional repercussions of WRMSDs, such as productivity loss, absenteeism, economic cost, and burnout were remarkably omitted. This lapse mirrors a gap in sub-Saharan occupational health research and confines the scope of understanding the systemic effects of WRMSDs.
Coping strategies and mitigation methods
The methods of mitigation adopted by physiotherapists in SSA reflect those recommended in international ergonomic and occupational health guidelines [7, 8, 16]. A universally most prominent reported strategy to cope with WRMSDs was modifying therapist or patient position, with uptake of over 70% in all four studies addressing coping strategies [12, 19–21]. This strategy is supported by the literature, showing that small ergonomic changes, such as repositioning the patient closer or adjusting hand positioning, can significantly reduce biomechanical load [24]. This shows the importance of ergonomic adjustments in workplaces to reduce the negative impact of WRMSDs and enhance productivity and outcomes.
Other coping strategies were also practiced extensively, such as adjusting plinth height, regular microbreaks, and technique modification. These are consistent with preventive frameworks that emphasize task variability and posture alternation to reduce cumulative strain [1, 25]. For instance, studies from Europe and North America show that stretching and posture shifts during treatment have been associated with decreased WRMSD symptoms [5, 24].
However, various vital interventions, such as mechanical lifting devices or ergonomic training, were less frequently reported. This shows limited institutional investment in WRMSD prevention infrastructure, as only one [21] documented its use. These dissimilarities are higher-income settings, where regular ergonomic assessments and access to lifting equipment are often embedded in physiotherapy departments [24].
According to Sagahutu and Nuhu, there is a relatively low rate of physiotherapists (40%) seeking professional treatment for WRMSDs [21]. This is similar to the report from Egypt, where 38.6% physiotherapists consulted a physician for their WRMSDs [22]. This may reflect accessibility, cultural, or financial barriers. Self-care and informal peer consultation may be preferred in some sub-Saharan settings, due to distrust of institutional systems or fear of professional stigma. These results underscore the need for workplace health promotion and confidential reporting pathways to reassure physiotherapists to seek care without fear of reprisal.
Recommendations for practice and policy for low-resource clinical settings
To reduce the incidence and impact of WRMSDs among physiotherapists in SSA, the following recommendations are proposed based on this review:
Integration of Ergonomics Training: Ergonomics should be incorporated into both undergraduate and postgraduate physiotherapy curricula, as well as through continuing professional development [24].
Policy development: Prevention guidelines, mandating periodic workplace safety assessments, and enforcement of occupational health legislation can be developed by national professional bodies and ministries of health to mitigate the effects of WRMSDs.
Promoting a safety culture: Encouraging early reporting, reducing stigma, and fostering collaborative support systems can help mitigate emotional impacts and facilitate timely intervention.
Establish “lift teams” to assist with heavy lifting, promote on-site fitness and stretching programs, and optimize workload management by balancing demanding tasks with less intense activities. The use of low-cost assistive aids, such as gait belts and friction-reducing sheets, should be encouraged. Additionally, fostering a culture of peer support and early reporting of discomfort can facilitate preventive care and help mitigate long-term issues.
Recommendations for practice and policy in high-resource clinical settings
To reduce the incidence and impact of WRMSDs among physiotherapists in SSA, the following recommendations are proposed based on this review:
1) Incorporate occupational health and safety and ergonomics into facility design and integration of ergonomics training: When constructing new facilities or remodeling existing ones, incorporate ergonomic concepts into the design to guarantee sufficient room around beds, suitable floor surfaces, broad doorways, and appropriately positioned fixed equipment. Ergonomics should be incorporated into both undergraduate and postgraduate physiotherapy curricula, as well as through continuing professional development [24]. 2) Institutional Reforms: To reduce exposure to physical stressors, healthcare facilities should invest in lifting equipment, redesigning workspaces to support neutral postures, and instituting job rotation and workload limits. 3) Policy development: Prevention guidelines, mandating periodic workplace safety assessments, and enforcement of occupational health legislation can be developed by national professional bodies and ministries of health to mitigate the effects of WRMSDs.
4) Advanced data gathering and intervention assessment: Make use of resources to carry out thorough research and surveillance on the prevalence and risk factors of WRMSD, using the results to improve and assess the efficacy of preventative measures. 5) Promotion of a safety culture: Promoting early report, reducing stigma, and encouraging collaborative support systems can help mitigate emotional impacts and foster timely intervention. 6) Establish a formal, dedicated safe patient handling (SPH) Program: Create a program with specified guidelines, qualified SPH specialists (also known as “lift-teams”), and the entire array of suitable patient transfer tools (such as ceiling lifts and portable hoists).
7) Required, periodic medical monitoring and fitness-for-work evaluations: Perform routine health and fitness evaluations to spot possible problems early and offer focused assistance or work adjustments.
8. Provide All-Inclusive Support Systems: To guarantee a speedy recovery and return to work following job-related accidents, make occupational health specialists, counseling, and possibly even on-site physiotherapy treatment accessible.
Conclusion
The considerable burden of WRMSDs among physiotherapists in SSA is highlighted by this scoping review, with the lower back, neck, and shoulders most commonly affected. The physical demands of manual therapy, poor ergonomic conditions, and limited access to assistive equipment contribute significantly to the prevalence of WRMSDs. Many physiotherapists adopt self-initiated coping strategies such as modifying posture, delegating tasks, and using electrotherapy, but formal institutional support, including ergonomic training and access to mechanical aids, remains limited. Despite the high incidence of WRMSDs, most physiotherapists continue practicing without changing their specialty or leaving the profession; this may reflect both resilience and the potential for chronic strain-related complications. Structured ergonomic education, policy reforms, and investment in occupational health infrastructure are required to safeguard the well-being and productivity of physiotherapists in the region.
Strengths and limitations of the review
To our knowledge, this is the first scoping review to map the prevalence, patterns, effects, and methods for mitigating WRMSDs among physiotherapists in SSA. This scoping review is not without limitations as the number of studies available from SSA is limited and mainly cross-sectional, restricting causality inference and possible recall bias. In addition, the geographic distribution of studies was uneven, with more than half conducted in Nigeria, potentially skewing region-wide conclusions. Also, language and publication bias may have excluded relevant studies published in non-indexed local journals.
Data availability
Data sharing does not apply to this article as no new data were created or analyzed in this study.
Disclaimer
The views, opinions, assumptions, or any other information presented in this manuscript are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of KwaZulu-Natal, Durban, South Africa.(Code: HSSREC/00007376/2024).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Supervision: Thayananthee Nadasan and Oladapo Olagbegi; Writing the original draft: Grace Emmanuel; Funding acquisition and Resources: Grace Emmanuel; Conceptualization, methodology, investigation, review & editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Badru Oluwaseun, Micheal Ogunlana and Olufemi Oyewole for their assistance in the study.
References
- Passier L, McPhail S. Work related musculoskeletal disorders amongst therapists in physically demanding roles: Qualitative analysis of risk factors and strategies for prevention. BMC Musculoskelet Disord. 2011; 12(1):24. [DOI:10.1186/1471-2474-12-24]
- Mbada C, Adejuyigbe O, Omole J, Idowu O, Okafor U, Adekanla B, et al. Assessment of knowledge, attitude and perception of Nigerian physiotherapists on manual handling techniques. J Environ Occup Health. 2015; 4(4):203-9. [DOI:10.5455/jeos.20151217013219]
- Obembe A, Onigbinde A, Johnson O, Emechete A, Oyinlola M. Occupational injuries among physical therapists in South-West, Nigeria. Niger J Med Rehabil. 2008; 13(1):25-30. [DOI:10.34058/njmr.v13i1.2.38]
- Chen CY, Lu SR, Yang SY, Liang F, Wang JJ, Ho CH, et al. Work-related musculoskeletal disorders among physical therapists in Taiwan. Medicine 2022; 101:e28885. [DOI:10.1097/MD.0000000000028885] [PMID]
- Gorce P, Jacquier-Bret J. Global prevalence of musculoskeletal disorders among physiotherapists: A systematic review and meta-analysis. BMC Musculoskelet Disord. 2023; 24(1):265. [DOI:10.1186/s12891-023-06345-6] [PMID]
- Vieira ER, Schneider P, Guidera C, Gadotti IC, Brunt D. Work-related musculoskeletal disorders among physical therapists: A systematic review. J Back Musculoskelet Rehabil. 2016; 29(3):417-28. [DOI:10.3233/BMR-150649] [PMID]
- Cromie JE, Robertson VJ, Best MO. Occupational health and safety in physiotherapy: guidelines for practice. Aust J Physiother. 2001; 47(1):43-51. [DOI:10.1016/s0004-9514(14)60297-x] [PMID]
- Lima M, Serranheira F. Absenteeism and presenteeism costs from occupational accidents with WRMSDS in a Portuguese hospital. Dyna. 2016; 83:27-30. [DOI:10.15446/dyna.v83n196.56605]
- Sirisawasd S, Taptagaporn S, Boonshuyar C, Earde P. Interventions commonly used to prevent work-related musculoskeletal disorders among healthcare workers. J Health Res. 2018; 32(5):371-83. [DOI:10.1108/JHR-08-2018-044]
- Abaraogu UO, Ezema CI, Nwosu CK. Job stress dimension and work-related musculoskeletal disorders among southeast Nigerian physiotherapists. Int J Occup Saf Ergon. 2017; 23(3):404-9. [DOI:10.1080/10803548.2016.1219476] [PMID]
- Cornelia B. The role of rehabilitation within low resource settings. Physiopedia [Internet]. 2025 [Updated 2026 January 4]. Available from: [Link]
- Adegoke BO, Akodu AK, Oyeyemi AL. Work-related musculoskeletal disorders among Nigerian physiotherapists. BMC Musculoskelet Disord. 2008; 9:112 [DOI:10.1186/1471-2474-9-112] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. [DOI:10.1136/bmj.n71] [PMID]
- Ogunlana MO, Govender P, Oyewole OO. Prevalence and patterns of musculoskeletal pain among undergraduate students of occupational therapy and physiotherapy in a South African university. Hong Kong Physiother J. 2021; 41(1):35-43. [DOI:10.1142/S1013702521500037] [PMID]
- Vincent-Onabajo GO, Nweze E, Kachalla Gujba F, Ali Masta M, Usman Ali M, Alhaji Modu A, et al. Prevalence of low back pain among undergraduate physiotherapy students in Nigeria. Pain Res Treat. 2016; 2016:1230384. [DOI:10.1155/2016/1230384] [PMID]
- Adje M, Odebiyi DO, Okafor UA, Kalu ME. Ergonomic principles in patient handling: Knowledge and practice of physiotherapists in Nigeria. Work. 2019; 64(4):825-32. [DOI:10.3233/WOR-193044] [PMID]
- Ganiyu SO, Olabode JA, Stanley MM, Muhammad I. Patterns of occurrence of work-related musculoskeletal disorders and its correlation with ergonomic hazards among health care professionals. Niger J Experiment Clin Biosci. 2015; 3(1):18-23. [DOI:10.4103/2348-0149.158153]
- Edith I, Eunice N, Stella U, Obidike O, Daniel M, Olatubosun A. Work-related musculoskeletal disorder among health workers: A cross-sectional survey of national orthopaedic hospital, Enugu. J Sci Res Stud. 2017; 4(11):318-32. [Link]
- Nkhata LA, Zyaambo C, Nzala SH, Siziya S. Work-related musculoskeletal disorders: Prevalence, contributing factors and coping strategies among physiotherapy personnel in Lusaka, Kitwe and Ndola districts, Zambia. Med J Zambia. 2010; 37(4):262-7. [DOI:10.4314/mjz.v37i4]
- Plange EB. Work-related musculoskeletal disorders among physiotherapists in Ghana: Prevalence, perceived causes and coping strategies [master thesis]. Accra: University of Ghana, 2019. [Link]
- Sagahutu JB, Nuhu A. A descriptive study on work related musculoskeletal disorders (WMDs) among physiotherapy practitioners in Kigali city: Prevalence, risk factors and preventive strategies. Niger J Med Rehabil. 2019; 20(1):1-16. [DOI:10.34058/njmr.v20i1.173]
- Khairy WA, Bekhet AH, Sayed B, Elmetwally SE, Elsayed AM, Jahan AM. Prevalence, profile, and response to work-related musculoskeletal disorders among egyptian physiotherapists. Open Access Maced J Med Sci. 2019; 7(10):1692-9. [DOI:10.3889/oamjms.2019.335] [PMID]
- Chen N, Fong DYT, Wong JYH. Secular trends in musculoskeletal rehabilitation needs in 191 countries and territories from 1990 to 2019. JAMA Netw Open. 2022; 5(1):e2144198. [DOI:10.1001/jamanetworkopen.2021.44198] [PMID]
- The Chartered Society of Physiotherapy. Guidance on manual handling in physiotherapy. 4th ed. London: The Chartered Society of Physiotherapy; 2014. [Link]
- Sharan D, Ajeesh PS. Injury prevention in physiotherapists-A scientific review. Work. 2012; 41(Suppl 1):1855-9. [DOI:10.3233/WOR-2012-0397-1855] [PMID]
Type of Study: Review Article |
Subject:
Physiotherapy
Received: 2025/10/31 | Accepted: 2025/11/29 | Published: 2025/03/2
Received: 2025/10/31 | Accepted: 2025/11/29 | Published: 2025/03/2
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.