

Volume 9, Issue 1 (Continuously Updated- In press 2026)
Func Disabil J 2026, 9(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ogunlana M O, Govender P, Oyewole O O, Nwosu I B. Adult Stroke Survivors’ Reintegration to Normal Living: A Scoping Review. Func Disabil J 2026; 9 (1)
URL: http://fdj.iums.ac.ir/article-1-348-en.html
URL: http://fdj.iums.ac.ir/article-1-348-en.html



1- Division of Occupational Therapy, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. , opeoluwamic@yahoo.com
2- Division of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
3- Division of Occupational Therapy, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. & Division of Occupational Therapy, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
4- Department of Medical Rehabilitation, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Awka, Nigeria.
2- Division of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
3- Division of Occupational Therapy, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. & Division of Occupational Therapy, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa.
4- Department of Medical Rehabilitation, Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Awka, Nigeria.
Keywords: Stroke, Community reintegration, Reintegration to normal living (RNL), Rehabilitation, Stroke survivors, Determinants, Interventions
Full-Text [PDF 1716 kb]
(88 Downloads)
| Abstract (HTML) (262 Views)

Full-Text: (48 Views)
Introduction
Cerebrovascular accident, or more commonly, stroke, is the second most common cause of death and disability worldwide. About 84% of the global stroke burden in 2021 was attributed to 23 modifiable risk factors. High systolic blood pressure remains the single most significant driver, contributing to over 56% of all stroke-related disability-adjusted life years (DALYs) [1]. With increasing sophistication in the medical care of stroke incidents, there is a gradual increase in the number of stroke survivors with stroke-related morbidities. These morbidities have necessitated increased utilization of physical rehabilitation facilities. Neurorehabilitation is often a long process that requires protracted periods of intervention, both in inpatient and outpatient facilities. Care is usually continued at home or community level to adapt the intervention to each survivor’s natural environment. Neuro-rehabilitation services are costly when available in the home environment. This has hindered the reintegration of stroke survivors into the community [2].
Reintegration to normal living (RNL) is one of the essential elements of stroke rehabilitation [3]. It is defined as the ‘reorganisation of physical, psychological, and social characteristics so that the individual can resume well-adjusted living after incapacitating illness or trauma’ [4]. Reintegration into normal living is synonymous with functional status—the individual’s typical performance [5]. The return of stroke survivors to family and community life involves engaging in normal roles and contributing to social groups. This successful transition depends on several complex factors [6–9]. The main determinants of reintegration include individual, physical, psychosocial, and environmental domains. Specifically, depressive symptoms and the perception of overall recovery significantly affect social reintegration [6, 10]. While Obembe et al. [8] also revealed that post-stroke depression was significantly associated with reintegration into normal living, they emphasised that motor recovery was equally crucial for community reintegration. Return to instrumental activities of daily living, such as driving a car, is significantly associated with reintegration into normal living among stroke survivors [11]. In a similar scoping review, Engel-Yeger et al. [7] recommended that participation outcomes be recovered as necessary for stroke survivors’ functional recovery. Wesselhoff et al. [12] in a systematic review reported that stroke survivors’ community mobility was significantly decreased compared to those without any neurological impairment. Community reintegration is a key indicator of participation and community mobility for stroke survivors; hence, more recent research has focused on it.
This review critically examined the evidence on RNL following a stroke. Despite these findings, existing literature often focuses on isolated variables rather than providing a holistic map of how physical and environmental factors intersect in the home environment. There remains a lack of clarity on which specific barriers most significantly impede the transition from clinical recovery to community participation. A scoping review methodology was selected to identify research areas on RNL for stroke survivors, using a range of research approaches, and to identify gaps in the current knowledge base to guide future research in the field.
Materials and Methods
This scoping review was based on the framework outlined by Arksey and O’Malley [13], which includes six iterative steps: (i) identifying the research question, (ii) searching for relevant studies, (iii) selecting the studies, (iv) charting the data, (v) collating, summarising, and reporting the results, and (vi) consulting with stakeholders to inform or validate findings. The sixth step, consultation with relevant stakeholders, remains optional and is considered a valued additional step, but has been excluded from this review. Recommendations made by Levac and colleagues [14] were also considered. The PRISMA extension for a scoping review (PRISMA-ScR) checklist was followed to report this study [15]. This protocol was registered on the Open Science Framework.
Step 1: Identifying the research question
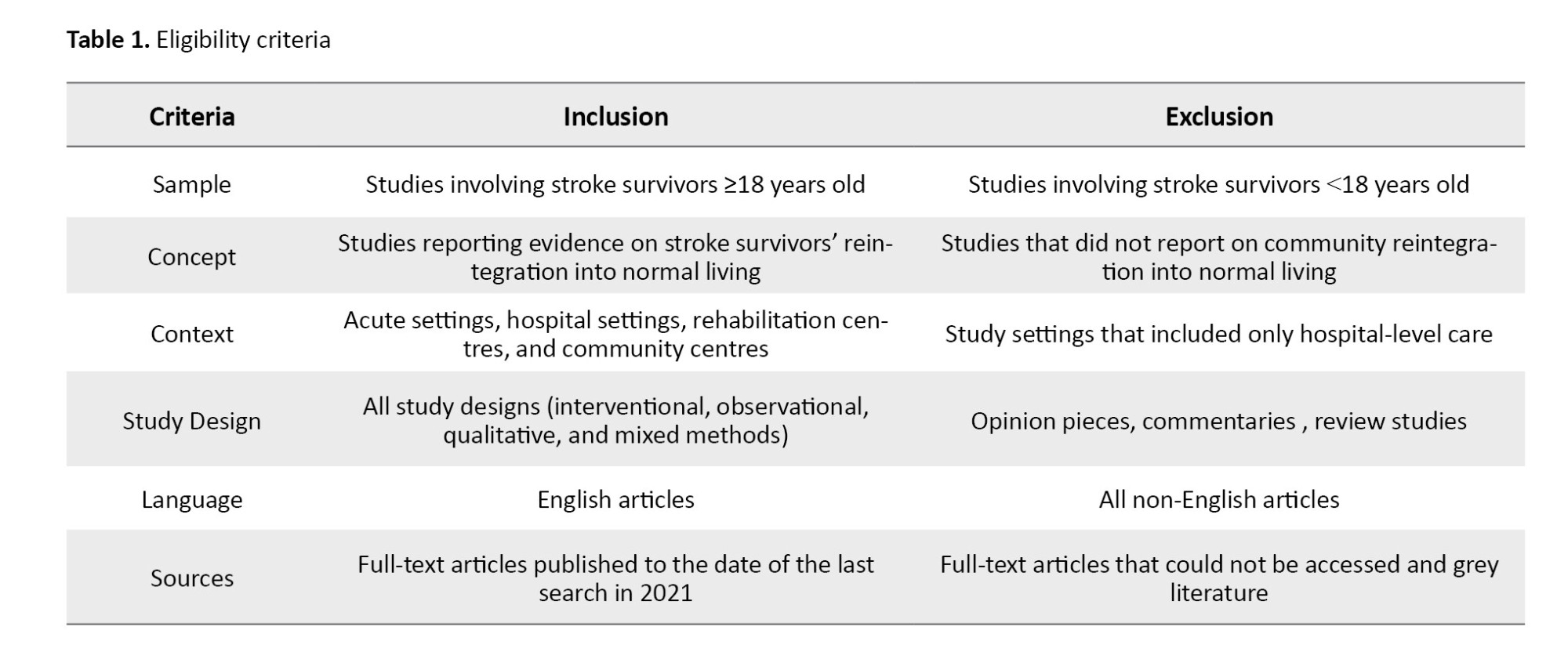
Table 1 illustrates the study's population, concept, and context. This scoping review aimed to answer the following question: “To date, what evidence exists on adult stroke survivor’s RNL?” The sub-questions for this review included the following:
1) To date, what evidence is there on the determinants of reintegration of adult stroke survivors into normal living? 2) What protocols, strategies, and interventions currently facilitate community reintegration for adult stroke survivors? 3) What are the gaps that exist in the reintegration of adult stroke survivors to normal living?
Step 2: Identifying relevant studies
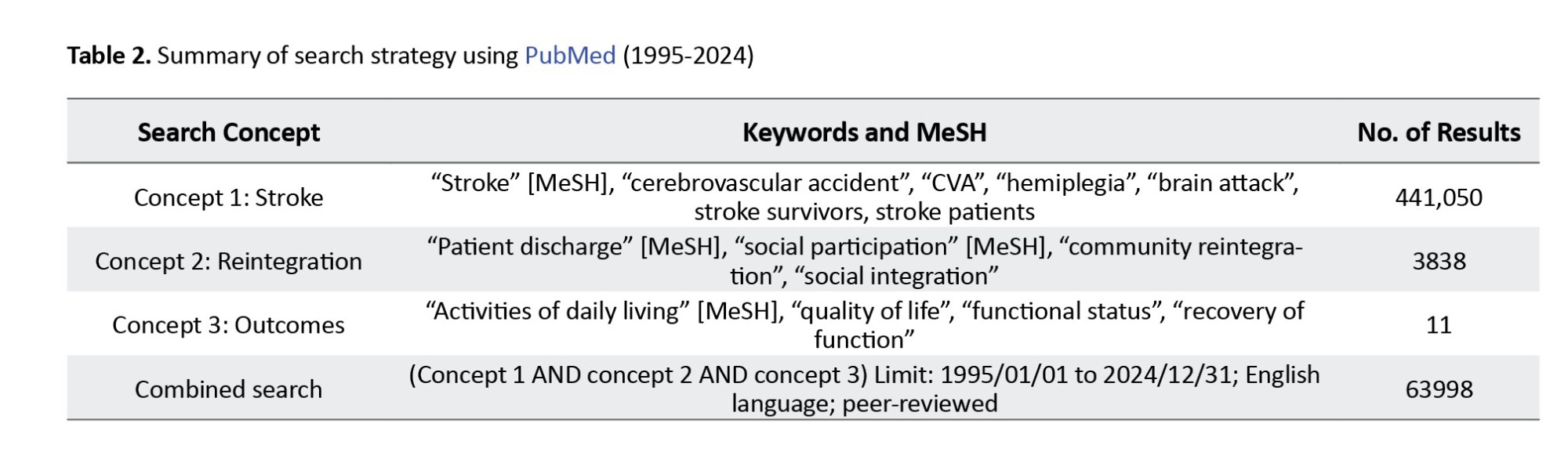
Information Sources: With support from a subject librarian, the authors conducted a systematic search in the following electronic databases: PubMed, cumulated index to nursing and allied health literature (CINAHL), Health source: Nursing/Academic Edition, Web of Science, and Scopus for relevant published literature between January 1995 and December 2024. The initial search was conducted in 2021 and was subsequently updated in January 2025 to include all relevant literature published through December 31, 2024. The search was limited to peer-reviewed English-language articles. Grey literature, including dissertations, policy documents, and unpublished reports, was not included to ensure that the synthesized evidence has undergone rigorous peer review and methodological scrutiny. This study used a comprehensive search strategy that employed keywords, medical subject headings (MeSH), and subject-heading search terms related to key concepts, as well as the Boolean operators “AND” and “OR.” A sample PubMed search is presented in Table 2. A secondary search of relevant articles from the reference lists of the included studies, using a snowball approach, was performed. Training exercises were conducted before the screening process to ensure reliability between reviewers. A single arbitrator/reviewer resolved all discrepancies between reviewers by revisiting the inclusion and exclusion criteria and instituting an additional pilot test. The EndNote reference manager was used to compile all relevant articles and identify duplicate records.
Step 3: Study selection
Eligibility criteria
This review included primary research across various designs, including randomized controlled trials (RCTs), observational studies (cohort and cross-sectional), and qualitative studies, to capture a comprehensive view of reintegration. The study included articles that met the defined eligibility criteria as follows:
Selection process
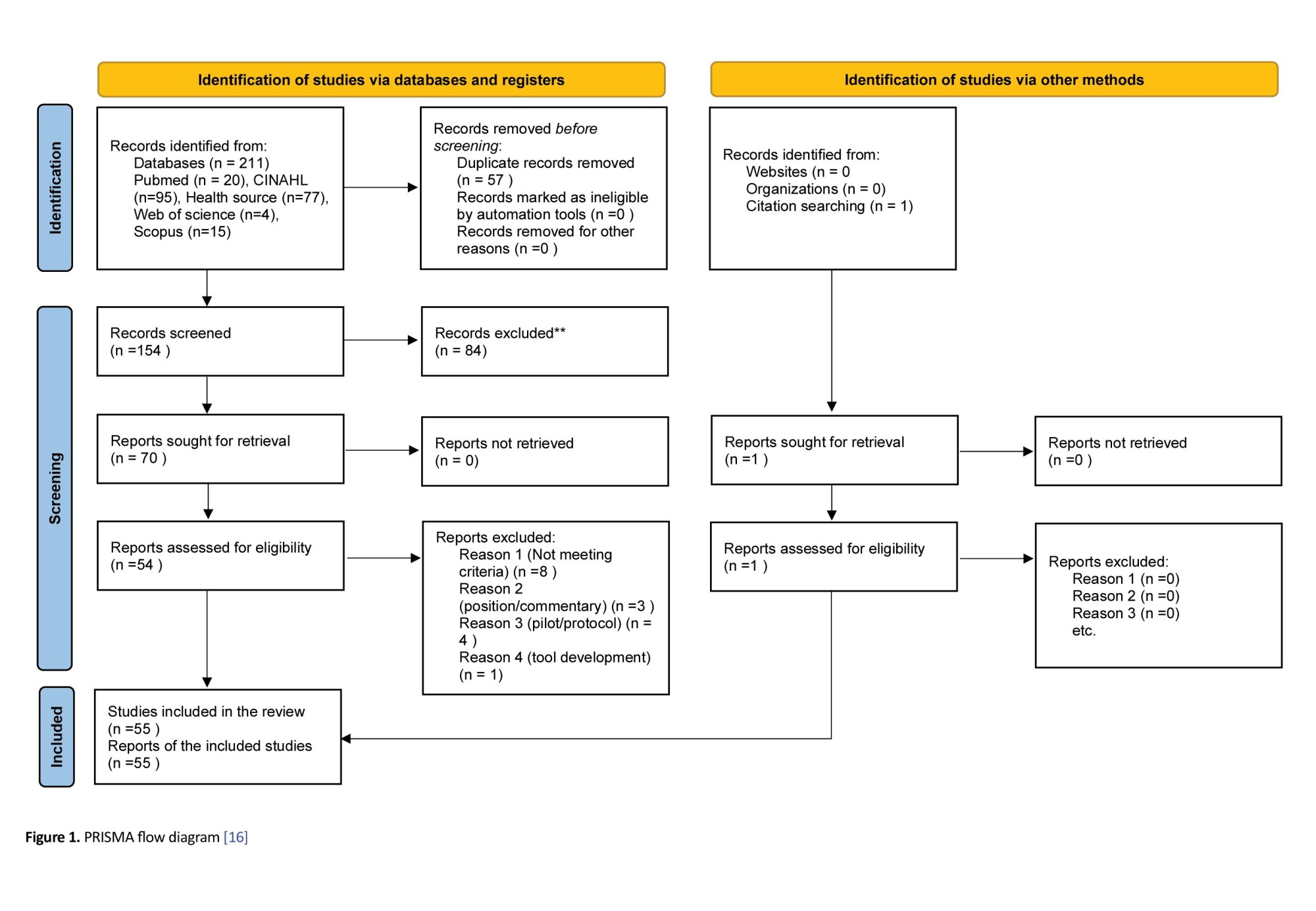
A thorough title screening was conducted by Michael O Ogunlana and Ifeoma Blessing Nwosu in the electronic databases guided by the eligibility criteria. All relevant articles were imported into an EndNote library, and duplicates were removed. The EndNote library was shared among the review team for the next stage of the study selection process. A screening tool was developed using the eligibility criteria for the abstract and full-text screening phases. Two reviewers (Pragashnie Govender and Michael O Ogunlana) independently conducted abstract and full-text screening and grouped them into “include” or “exclude” categories. Discrepancies between Pragashnie Govender and Michael O Ogunlana during the abstract screening phase were addressed through discussion among the review team until consensus was reached. At the full-text phase, Ifeoma Blessing Nwosu and Olufemi O. Oyewole resolved any discrepancies between Pragashnie Govender and Michael O Ogunlana. Where an article could not be accessed freely online, assistance from the institution’s library services was sought. The original authors were also accessed via email for requests for complete texts, if necessary. Cohen's kappa coefficient (κ) statistic was calculated to determine the inter-rater agreement between the reviewers at the end of the full-text screening phase. The PRISMA flow diagram [16] was adopted to report the screening results, as illustrated in Figure 1.
Step 4: Charting the data
A form was developed in Google Forms for data extraction and piloted to ensure accuracy. After thoroughly reading the full texts, Pragashnie Govender and Michael O Ogunlana extracted all relevant data from the included articles. The data extraction form included the following details: (i) title of the study, (ii) year of publication, (iii) study setting, (iv) aims, (v) country of the study, (vi) study design (vii), study participants (viii), study results, (ix) findings relevant to answer the question, (x) conclusion, and (xi) recommendations. Any discrepancies during data extraction were resolved through discussion among the two extractors (Pragashnie Govender and Michael O Ogunlana), with Olufemi O. Oyewole serving as a third-party arbitrator when consensus could not be reached. The form was continually updated to capture all relevant data to answer the review question.
Step 5: Collating, summarizing, and reporting the results
The review team ensured that the extracted data were exposed to thematic analysis [17]. Relevant themes and sub-themes relating to the study objectives were developed around the following: (i) determinants of reintegration, (ii) protocols, strategies, and interventions available for stroke survivors that assist in community reintegration, and (iii) identified gaps in the successful reintegration of stroke survivors to their relevant communities. This was presented as a narrative of the relevant themes and sub-themes. Where possible, tables and figures were also used to show the results.
Step 6: Methodological quality appraisal
Although not mandatory, the critical appraisal of evidence sources was included in this review to assess methodological quality using the Mixed Methods Appraisal Tool (MMAT) [18]. This instrument has a prescribed set of questions that examine the appropriateness of the different sections reported in each evidence source. A quality score was assigned to each reported study, with ≤50% interpreted as low quality, 51-75% as average quality, and 76-100% as high quality [19]. Two reviewers (Michael O Ogunlana and Olufemi O. Oyewole) independently conducted the quality appraisal to reduce bias. The quality appraisal scores were used to contextualize the strength and reliability of the evidence; however, low-quality studies were not excluded from the thematic analysis, consistent with the inclusive nature of scoping review methodology.
Results
One hundred and fifty-four (154) articles met the eligibility criteria following the deletion of 57 duplicates from the 211 articles identified at the title screening stage, as illustrated in the PRISMA flow diagram (Figure 1). Subsequently, 84 and 16 articles were excluded following abstract and full-text screening, respectively. Reasons for exclusion after full-text screening included: a tool development and validation study in the post-stroke population [20], a tool development and validation study in the post-stroke population [20]; a position paper on the return to driving and reintegration of stroke survivors [21]; Cott et al. [22] wrote a commentary on preparing stroke survivors for reintegration; Jhaveri et al. [23] reported a pilot study on the feasibility of Telerehabilitation for stroke survivors; and Merz et al. [24] reported a factor analysis of the RNL index. Miller et al. [25] published a position paper on the transition of stroke survivors to the home environment, and Plow et al. [26] also published a proposal on a weight management program for stroke survivors. Montgomery et al. [27] and Somerville et al. [28] published protocols on the community reintegration of stroke survivors. Ogourtsova et al. [29] reported clinicians’ opinions on the use of virtual reality in the assessment of hemineglect. Sieber et al. [30] reported an autoethnography on the authors’ personal experience as stroke survivors. Stark et al. [31] reported an unpowered study that examined the feasibility of community-based environmental modification intervention (COMPASS) among stroke survivors. A study [32] reported the inter-rater reliability of the RNL Index; two studies [33, 34] reported the psychometric properties of the subjective index of physical and social outcome (SIPSO); and a study [35] reported the perceptions of stroke survivors about therapeutic relationships and client-centered practice. Overall, 55 studies met the study eligibility criteria for data extraction, including one study identified following an updated search. There was substantial agreement between the reviewers’ responses at the full-text screening stage (Kappa statistic=0.90, P<0.01).
Characteristics of the included studies
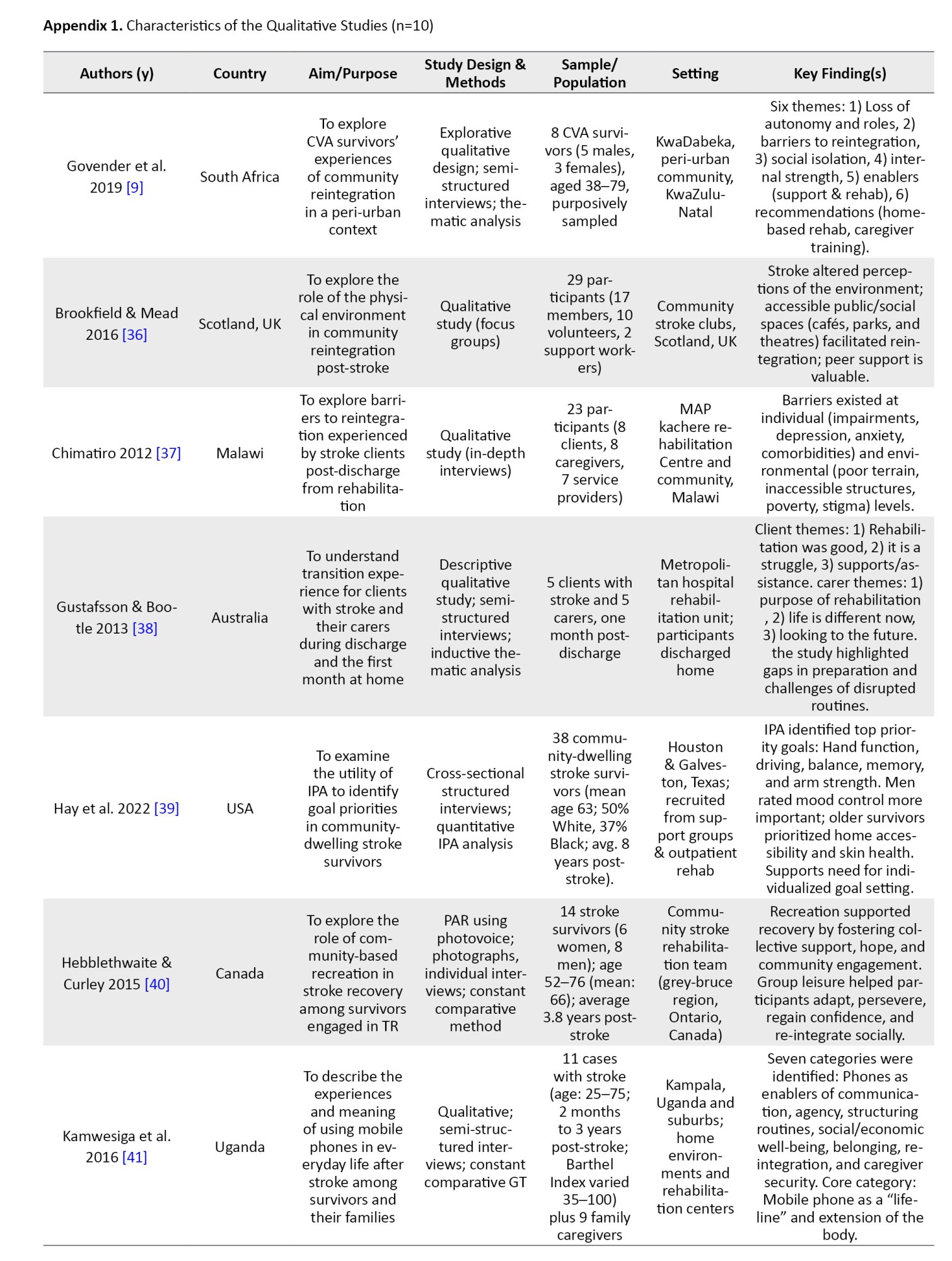
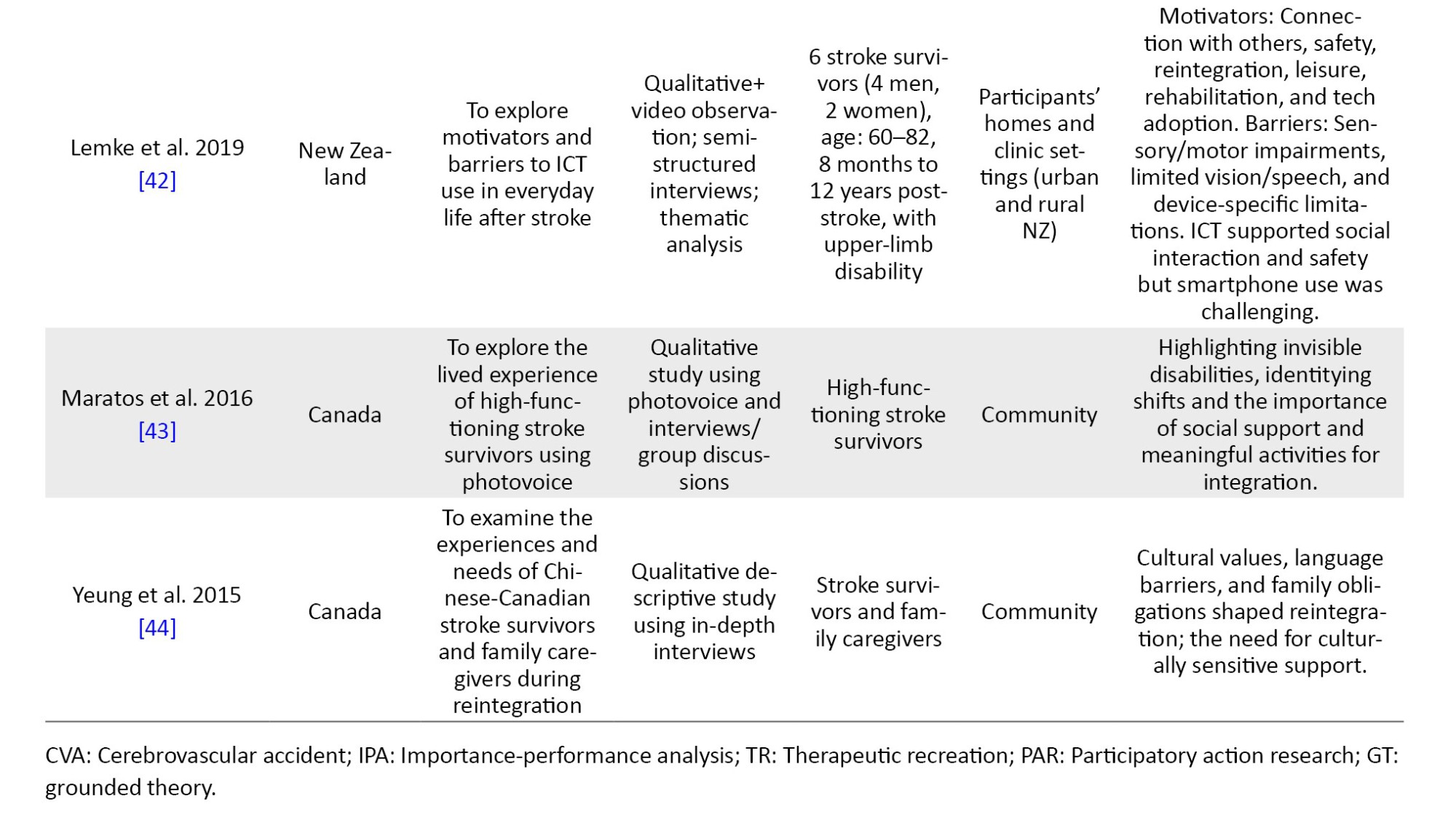
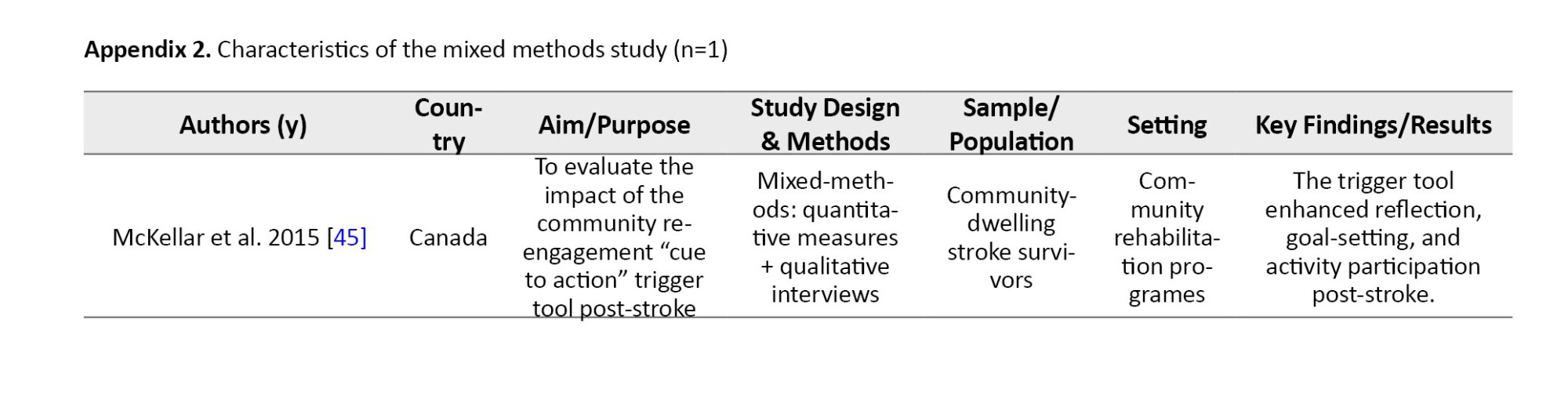
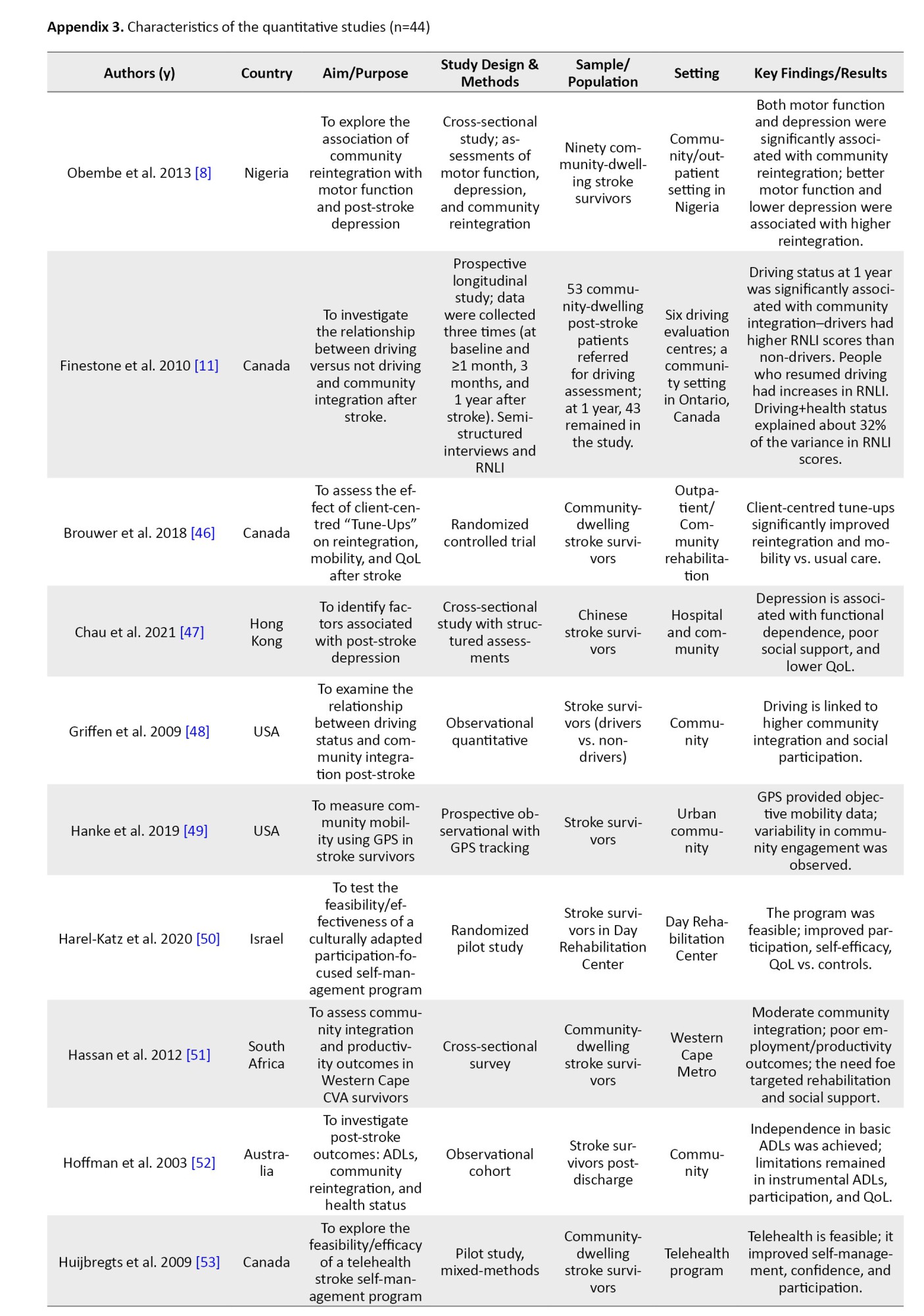
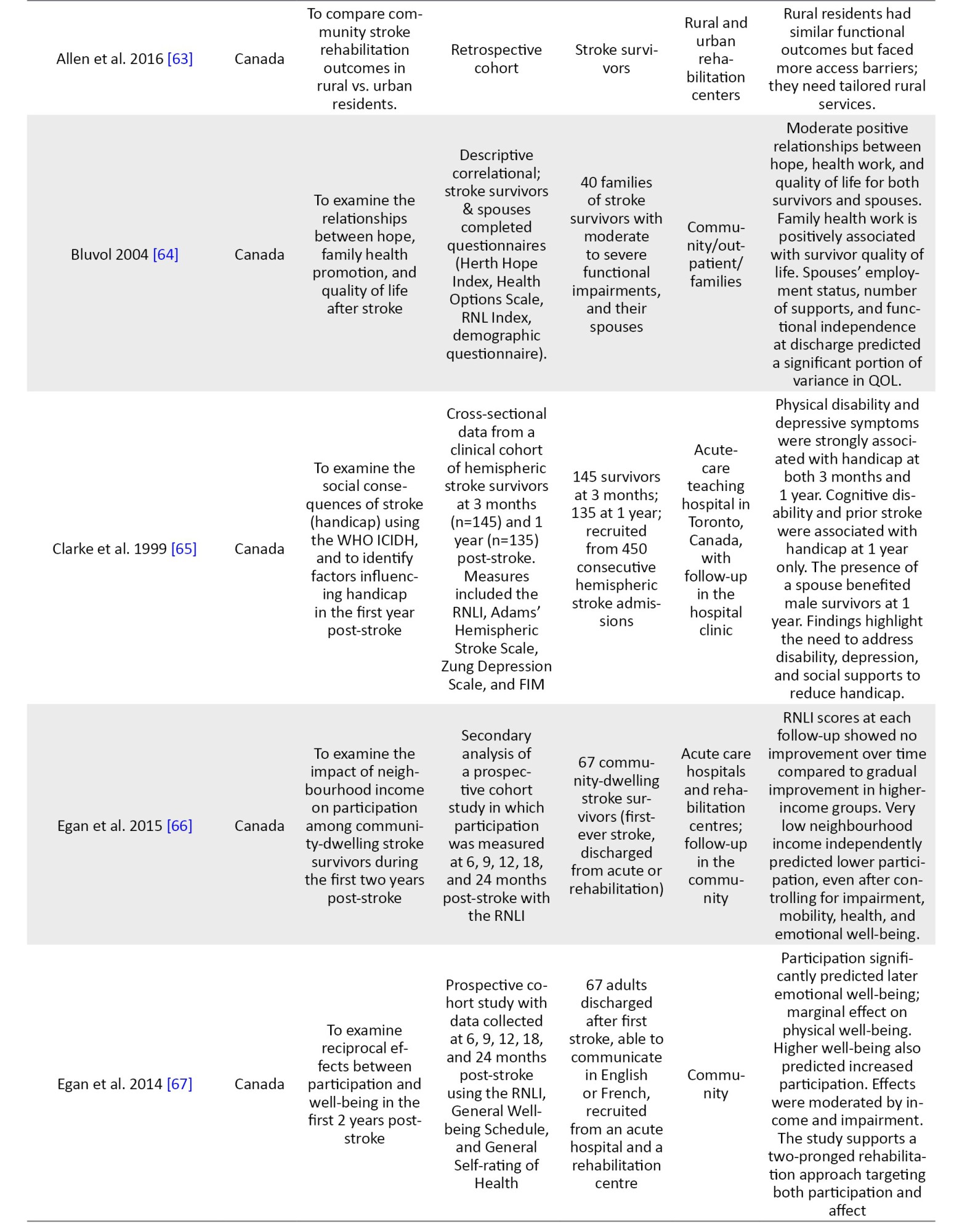
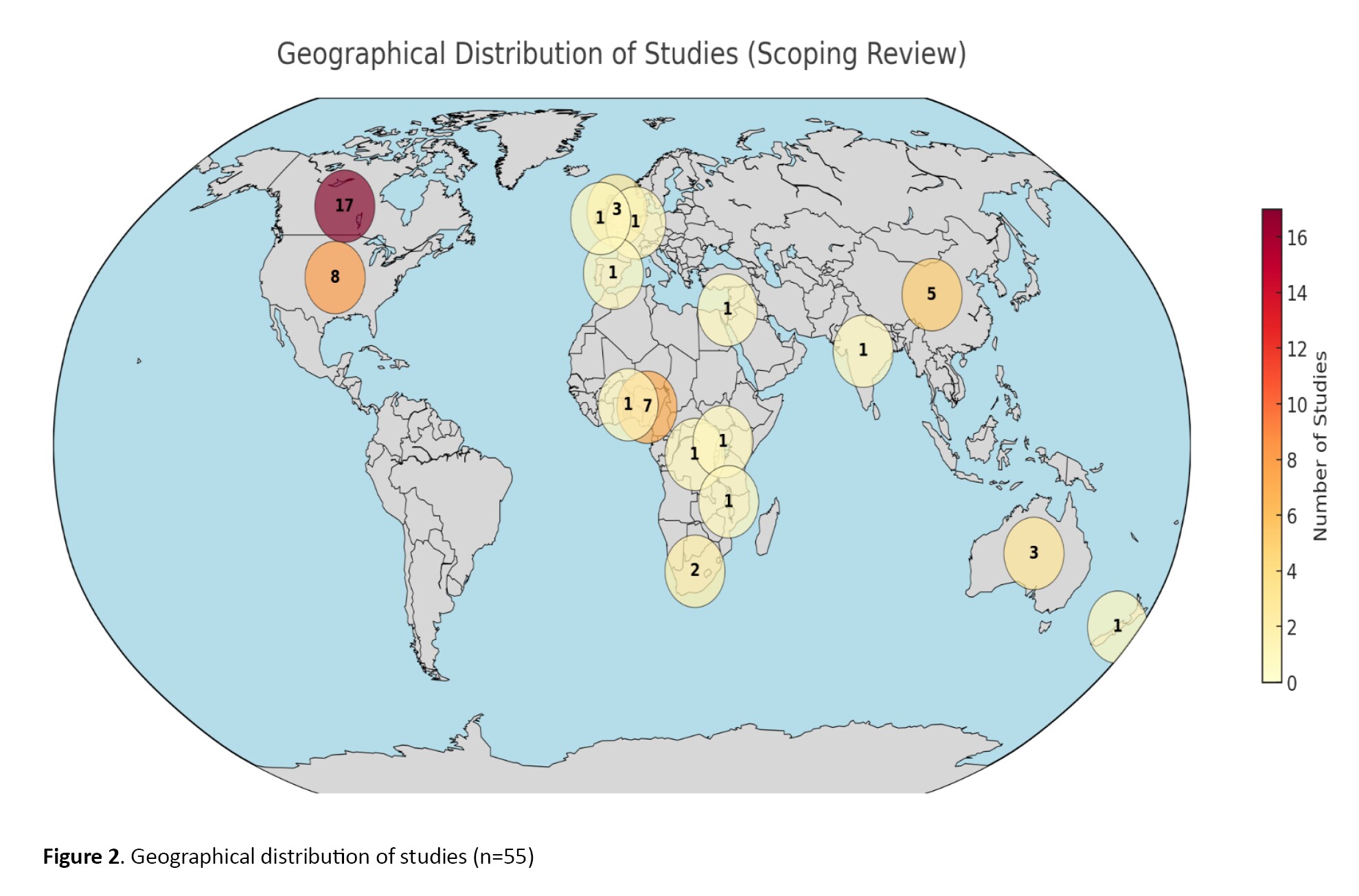
The characteristics of the 55 studies included are summarized in Appendices 1, 2 and 3. Ten studies utilized a qualitative methodology [9, 36–44]. A study used a mixed-methodology [45], while the remaining 44 studies used a quantitative methodology. All included studies were published in English between 1995 and 2024. Twenty-two studies [11, 37, 41, 42, 45–62] were conducted in institutionalized settings, like rehabilitation homes, hospitals, and outpatient care, while the remaining 33 studies were conducted in community settings. Of the 55 studies, 17 were conducted in Canada [11, 40, 43–46, 53, 59, 63–71], eight studies were conducted in the USA [39, 48, 49, 58, 62, 72–74], seven studies were conducted in Nigeria [8, 54–56, 61, 75, 76], four studies were conducted in China [47, 60, 77, 78], three studies were conducted in Australia [38, 52, 79], two studies were conducted in each of South Africa [9, 51], and the United Kingdom [80, 81]. One study was conducted in each of these countries: Netherlands [82], Congo [83], India [84], Israel [50], New Zealand [42], Uganda [41], Spain [85], Benin [86], Ireland [57], Scotland [36], Hong Kong [87], and Malawi [37] (Figure 2).
Quality of evidence
The 55 studies underwent methodological quality assessment using the Mixed Methods Appraisal Tool (MMAT software, version 2018) [18]. Out of the 44 included studies that had a quantitative methodology, the methodological quality appraisal score ranged from 50 to 100%, with 15 studies [8, 46, 58, 61–63, 65, 66, 68, 69, 78, 81–83, 85] scored 100%, 26 studies [11, 47–49, 51–57, 60, 64, 67, 70, 72–77, 79, 80, 84, 86, 87] scored 75%, and three studies [50, 59, 71] scored 50%. Ten studies used a qualitative methodology, with quality appraisal scores ranging from 75% to 100%. Three of these studies [37, 38, 41] scored 100%, and 7 of these studies [9, 36, 39, 40, 42–44] scored 75%. The only mixed-method study [45] scored 100%. Methodological limitations were primarily found in quantitative, non-randomized studies, where pre-stroke functional status was often not accounted for as a confounding variable. In qualitative studies, the most common deficit was a lack of transparency regarding 'researcher reflexivity'—how the researchers' own perspectives may have influenced the data collection and analysis.
Study finding
Determinants of stroke survivors' reintegration into normal living
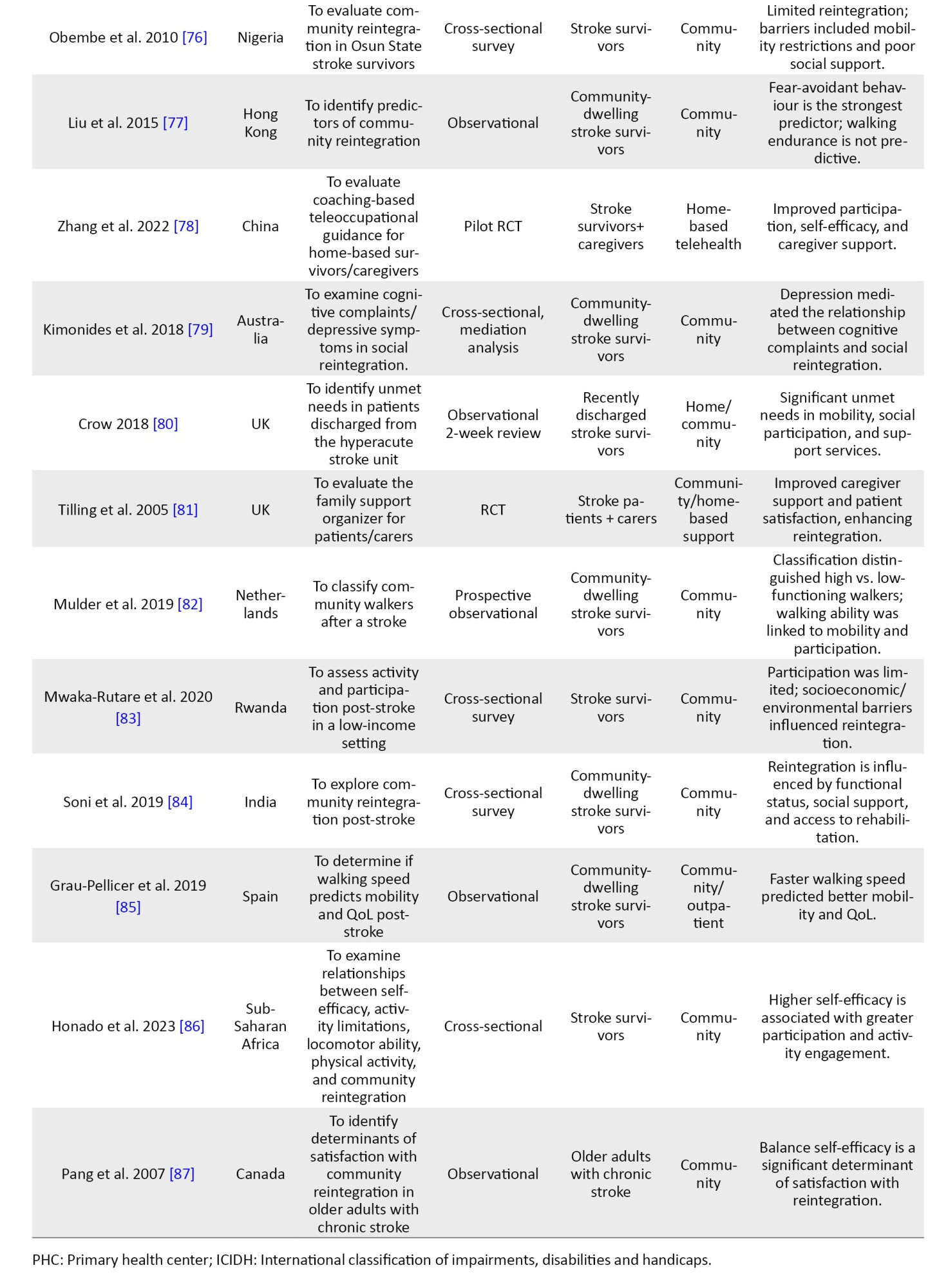
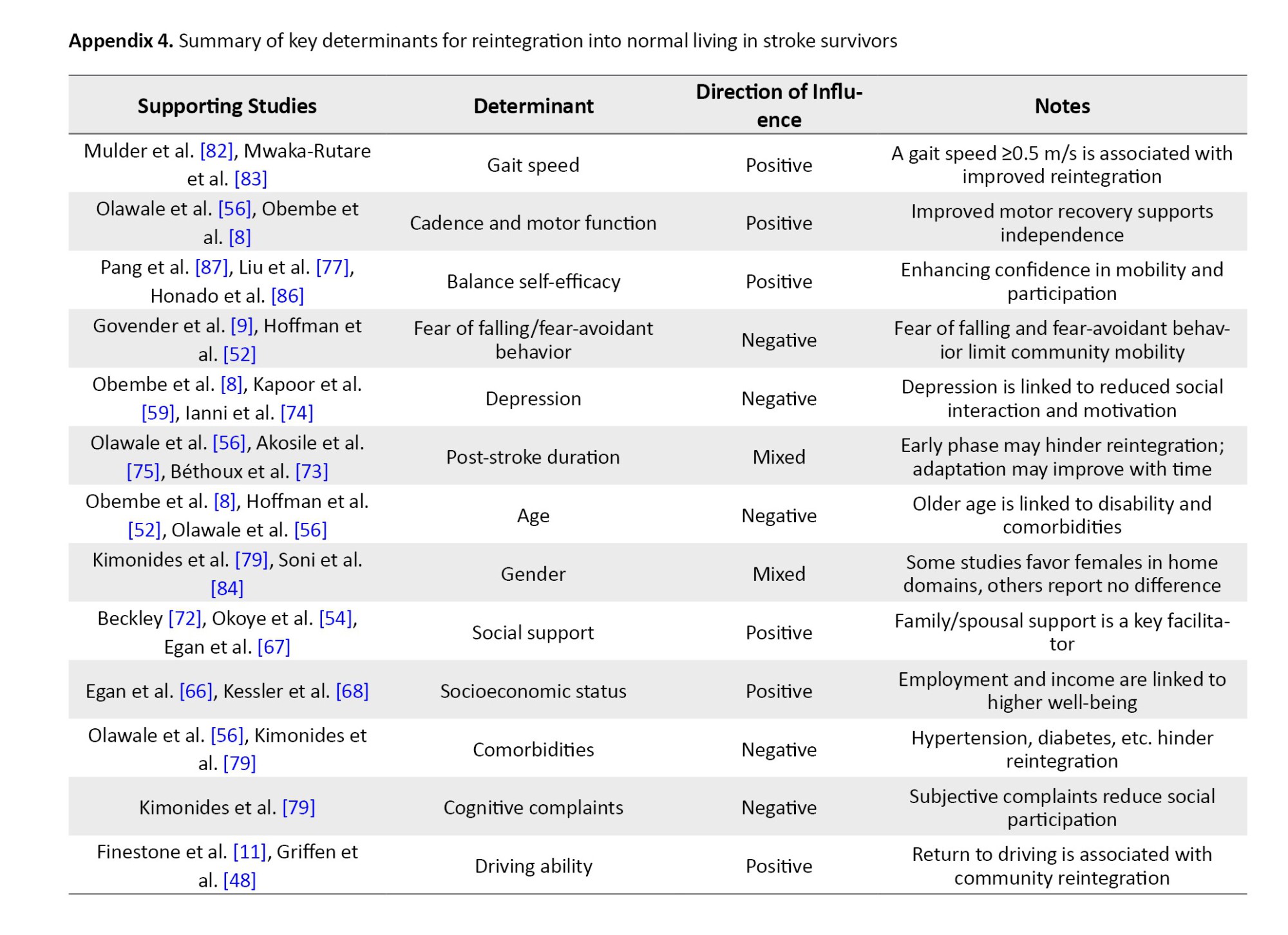
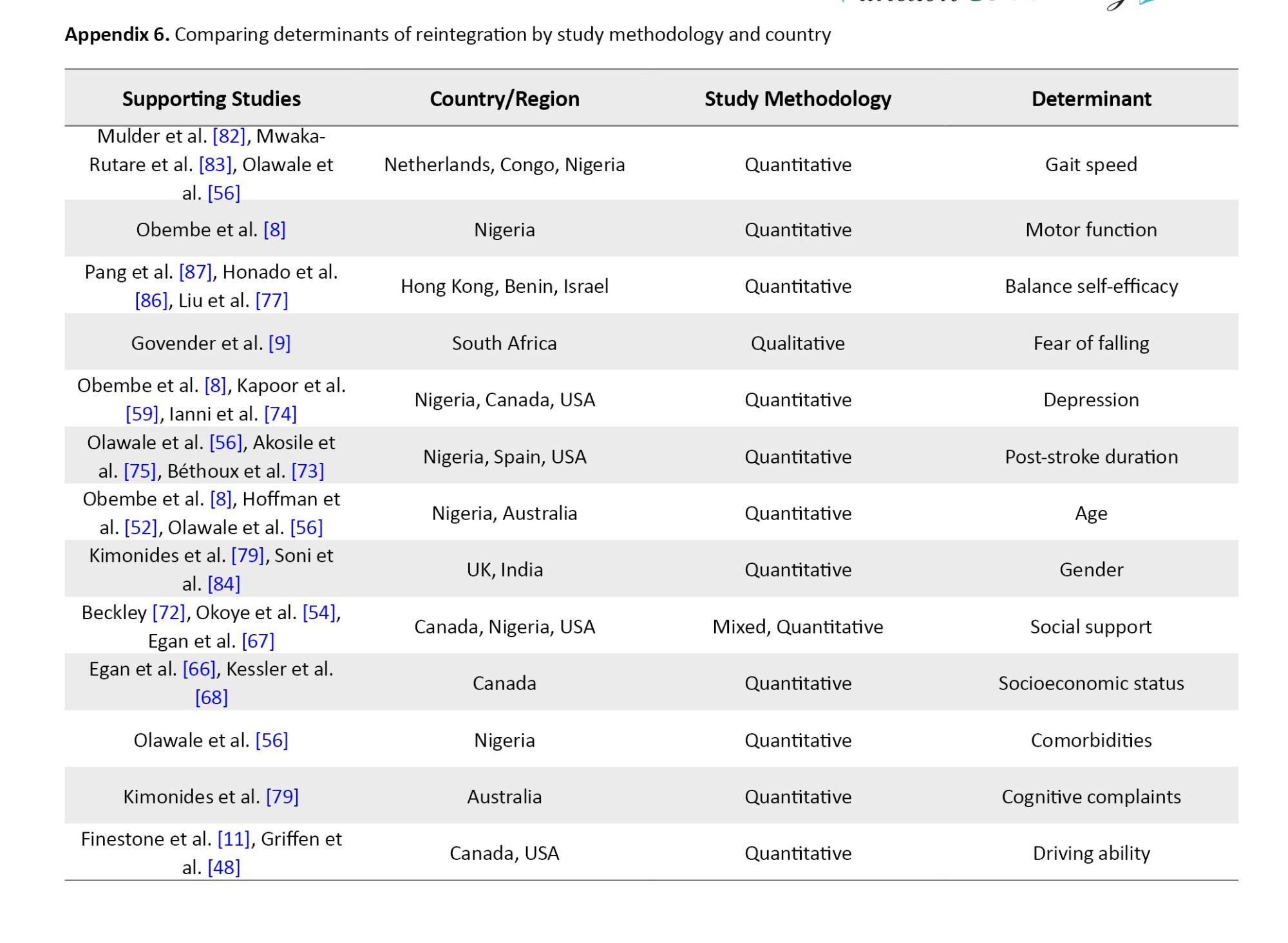
Different authors described the determinants of stroke survivors’ reintegration into normal living in various ways across studies using quantitative methodologies. Some authors described this construct as a predictor of community reintegration; others referred to it as a measure of participation, handicap, satisfaction, and well-being. Mulder et al. [82] concluded that a comfortable gait speed of not less than 0.5 m/s positively predicted community reintegration for stroke survivors. This was supported by other two studies [56, 83]. Mwaka-Rutare et al. [83] reported that higher walking speed improves basic activities of daily living, thereby improving community reintegration, while Olawale et al. [56] focused on increasing cadence (steps per minute) as a positive determinant of community reintegration. Increasing gait speed is also associated with improved motor function, as reported by Obembe et al. [8] as a positive predictor of community reintegration. However, Olawale et al. [56] also reported functional mobility. Hoffman et al. [52] also reported that balance self-efficacy, mobility, and stroke duration positively predict community reintegration. They further identified decreased stride time and fall self-efficacy as negative predictors of community reintegration for stroke survivors.
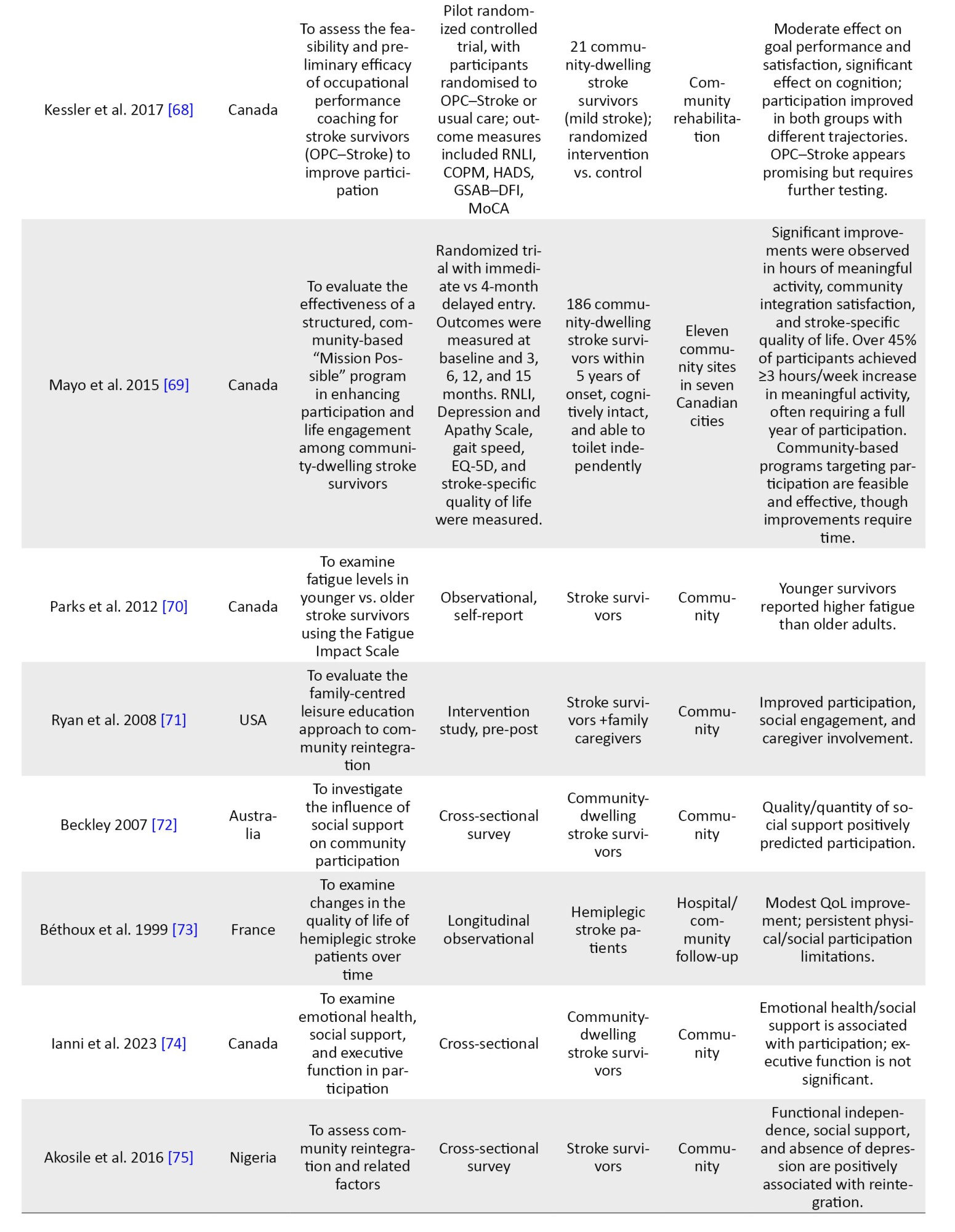
Some researchers [60, 77, 86, 87] examined the roles of balance self-efficacy, participation self-efficacy, absence of fear-avoidant behaviors, and self-efficacy as positive predictors of community reintegration. Pang et al. [87] reported that balance self-efficacy accounted for 6.5% of the variance of community reintegration. Some studies [54, 56, 76] reported increasing post-stroke duration as a positive predictor of community reintegration; however, only one study [73] reported increasing post-stroke duration as a negative predictor of community reintegration. Demographic variables, such as age and gender were also found to significantly influence community reintegration. Increasing age was unanimously described as a negative predictor of community reintegration for stroke survivors [8, 52, 75]. Being female [79] was a positive predictor of home integration, but Soni et al. [84] concluded that gender was not a determinant of community reintegration among stroke survivors.
Stroke survivors' social status, like living in a higher-income neighbourhood [66], being employed post-stroke [75], having higher levels of well-being through higher incomes [67], and having social (family and spousal) support [54, 65, 72, 74], significantly predicted community reintegration positively. Beckley [72] reported that after controlling for many factors, like age, race, income, and functional limitation, social support was found to be most predictive of community reintegration among stroke survivors. The car driving status was also investigated; researchers [11, 48] reported that the ability to return to driving a car was a positive predictor of community reintegration. The ability to drive post-stroke, when combined with stroke severity, predicted 32% of the possibilities of attaining community reintegration [11], especially among male stroke survivors [48]. The presence of comorbidities, like high blood pressure and T2DM [75], depression/poor emotional health [8, 65, 74, 75, 79], disabilities [65], and dependence on assistive mobility devices [75] were negative predictors of community reintegration. The absence of subjective cognitive complaints was also positively associated with community reintegration [79].
The qualitative research reviewed explored the determinants of community reintegration among stroke survivors. Govender et al. [9] reported the fear of falls and stigma as barriers and family/friend support as enablers to community reintegration. Similarly, Maratos et al. [43] reported that ease of access to social support services, adequate transportation, and accommodation post-stroke enable community reintegration. The need to focus on the transition to a home environment during rehabilitation was reported as an enabler of community reintegration by Gustafsson and Bootle [38], and uneven environmental terrains, altitudes, and inaccessible structures were reported to hinder community reintegration [37]. Kamwesiga et al. [41] reported a focus on the use of mobile phones by stroke survivors as an enabler of social integration that may aid community reintegration. The role of timely education about oriental diets and traditional medicines for stroke survivors' rehabilitation is reported as an enabler of community reintegration [44]. Attainment of rehabilitation goals, like improvement in hand function, balance, driving, and memory are enablers of community reintegration [39]. The use of community-based recreational services is also reported to enhance community reintegration [40]. Accordingly, determinants of reintegration can be categorized into four primary domains: Physical and functional: gait speed and motor recovery were the most frequently cited predictors [8, 56, 82]. Specifically, a gait speed of ≥0.5 m/s served as a critical threshold for community mobility [82, 83]. Psychological: Self-efficacy and the absence of depression were consistently linked to higher participation [8, 65, 87]. Conversely, fear of falling emerged as a primary psychological barrier in qualitative reports [9, 39]. Social: family and spousal support were the strongest predictors of social reintegration across both high- and low-resource settings [54, 72]. Environmental factors, such as car-driving status [11] and neighbourhood income levels [66], significantly influenced the ease of community re-entry. Appendices 1, 2, 3, 4, 5 and 6 present the summary of these findings.
Protocols, strategies, and interventions to support community reintegration for stroke survivors
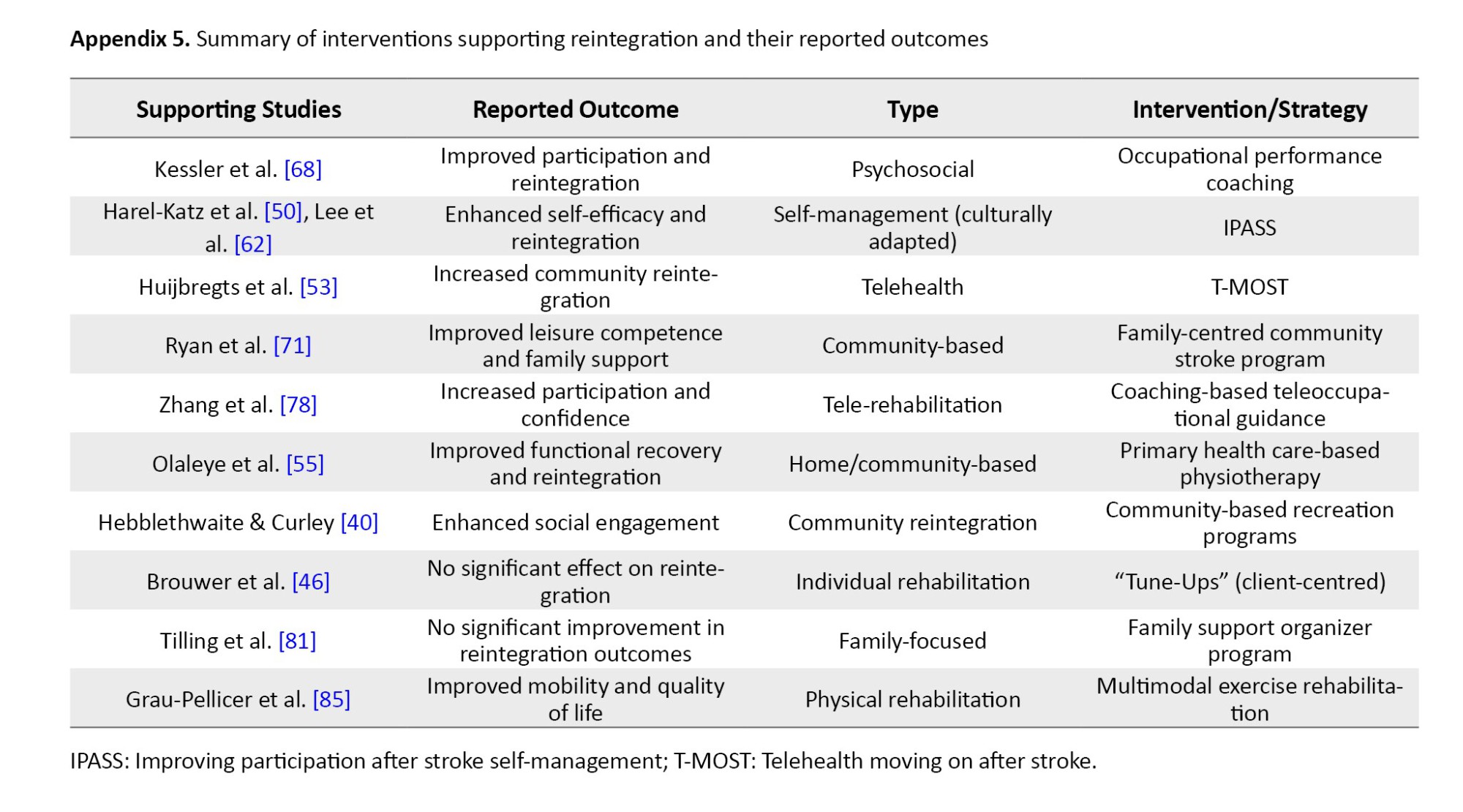
Thirteen articles reviewed described protocols, strategies, and interventions to support stroke survivors in achieving community reintegration. Kessler et al. [68] reported the usefulness of occupational performance coaching in enhancing stroke survivors' achievement of community reintegration. The family-centred community stroke program [71] improved the perception of leisure competence of stroke survivors and their spouses, and was reported to have enabled reintegration into the community. Different versions of the Improving Participation After Stroke Self-Management (IPASS) contributed to enhancing community reintegration. Harel-Katz et al. [50] used the culturally adapted version of IPASS, while Lee et al. [62] used the rehabilitation version of the IPASS in their article. Huijbregts et al. [53] reported the use of a Telehealth stroke self–management program called Telehealth Moving on After Stroke (T-MOST), which helps enhance community reintegration for stroke survivors.
Multimodal exercise rehabilitation program [85], primary healthcare-based physiotherapy intervention [55], getting on with the rest of your life mission possible [69] community re-engagement cue to action trigger tool - CRCATT [45], community-based recreation [40], and coaching-based Tele-occupational guidance [78] were all documented to have enhanced community reintegration among stroke survivors. Client-centred ‘tune-ups” [46] and Family Support Organizer Program [81] are strategies that did not significantly enhance community reintegration. Intervention efficacy appeared to be influenced by delivery mode and intensity. Programs utilizing Telehealth [53, 78] or intensive coaching [68] reported higher participant engagement and significant RNLI improvements compared to one-off 'tune-up' sessions [46], which lacked the sustained intensity required for long-term behavioural change.
Measures of community reintegration
Most articles (56.4%, 31 out of 55) that qualified for this review utilized the Return to Normal Living Index (RNLI) to measure the extent of community reintegration. Other articles measured community reintegration using a Community Ambulation Questionnaire [82], a Community Integration Questionnaire [79], a Community Integration Measure [77], a Direct Measure of Community Mobility [49], and working speed [85]. The Adapted Maleka Stroke Community Reintegration Measure [54] was used to estimate the extent of community reintegration. Tools used in other research include the return-to-work [57], SIPSOs [46], and post-stroke checklist [47, 70, 80]. While the RNLI was the most frequent measure (57%), it focuses heavily on subjective perception. In contrast, tools, like the SIPSO and Maleka measures showed lower adoption rates, likely due to a lack of extensive psychometric validation across diverse cultural contexts compared to the well-established RNLI.
Quantitative synthesis of results
Of the 44 quantitative studies included in this review, several key determinants of RNL were consistently reported. Motor function and mobility indicators, such as gait speed, cadence, and balance, were among the most frequently assessed variables. These were investigated in approximately 16 studies (36%), and nearly all identified them as strong positive predictors of reintegration outcomes. For example, a gait speed of ≥0.5 m/s was linked to better reintegration in studies by Mulder et al. [82] and Mwaka-Rutare et al. [83], while cadence and motor recovery were emphasized in studies from Nigeria by Olawale et al. [56] and Obembe et al. [8]. Depression and emotional health were examined in at least 6 studies (14%). All of these studies reported negative associations between post-stroke depression and reintegration, suggesting that emotional well-being plays a critical role in post-stroke recovery and community participation [59, 74, 75, 79]. Balance between self-efficacy and confidence in performing daily activities was evaluated in 6 quantitative studies (14%), including those by Pang et al. [87], Liu et al. [77], and Honado et al. [86]. These studies found statistically significant positive relationships between self-efficacy scores and reintegration outcomes.
Social support was identified as a facilitating factor in at least 8 quantitative studies (18%), including those by Egan et al. [67], Okoye et al. [54], and Beckley [72]. These studies highlighted that stroke survivors with strong family or spousal support were significantly more likely to achieve higher reintegration scores. Post-stroke duration was assessed in 5 quantitative studies (11%), with mixed findings. While three studies [56, 75] found that longer duration post-stroke improved reintegration, at least one study [73] indicated a decline over time. Comorbidities, such as hypertension, diabetes, and stroke-related complications were reported as barriers to reintegration in approximately 5 studies (11%), with all of them showing negative associations [75, 79]. Demographic variables, particularly age, were commonly analyzed. Older age was found to negatively impact reintegration in at least 5 studies (11%), including those by Hoffman et al. [52] and Olawale et al. [56]. Gender was reported in several studies but showed no consistent pattern; for instance, Kimonides et al. [79] found gender-specific effects, while Soni et al. [84] found no significant association. Driving ability and return to work as indicators of functional independence were studied in 2–3 quantitative studies (4–7%), such as studies by Finestone et al. [11] and Griffen et al. [48], and were found to have positive correlations with reintegration scores. Interventional studies among the 44 quantitative papers numbered about 13(30%). Most of these interventions—including Telehealth, occupational coaching, and structured self-management—reported statistically significant improvements in reintegration scores post-intervention [53, 62, 68, 71]. However, two studies [46, 81] showed no significant effect, suggesting the need for context-specific or more personalised approaches. Regarding measurement tools, the RNLI was the most frequently used instrument, applied in about 25 of the 44 quantitative studies (57%). Other tools included the SIPSO and the community integration questionnaire, though these were used less consistently.
Qualitative synthesis of results
The qualitative studies included in this review provided deep insights into how stroke survivors experience reintegration into their communities [9, 36, 38, 40, 41, 43, 44, 53, 88]. Emotional, social, and environmental dimensions were consistently highlighted as shaping the reintegration process.
A key theme across several studies was the emotional complexity of reintegration [9, 36, 43]. Survivors often expressed fear, anxiety, and frustration about resuming social and occupational roles [9, 43]. For example, Govender et al. [9] emphasized that fear of falling and social stigma restricted survivors’ community mobility, even in the presence of good physical recovery. Similarly, Maratos et al. [43] reported that high-functioning survivors withdrew from public spaces due to internalized emotional and psychological challenges.
Environmental and societal barriers were another frequent theme [9, 36, 41, 88]. Studies conducted in low-resource settings, such as Malawi [88] and Uganda [41], identified poor infrastructure, inaccessible public transport, and lack of rehabilitation continuity as key constraints. These structural limitations restricted survivors’ ability to fully participate in community life [41, 88]. Brookfield et al. [36] also described how physical environments could either facilitate or obstruct reintegration, depending on their design and accessibility.
Social relationships emerged as a vital component of successful reintegration [38, 44, 53]. Survivors emphasized the importance of family, caregivers, and peers in supporting their transition from rehabilitation to home and community [38, 44]. In Yeung et al.’s study [44] involving Chinese-Canadian stroke survivors, family support was essential to rebuilding confidence and promoting functional participation. In contrast, the absence of such support was linked to emotional isolation and reduced community participation [44]. Some studies reported that survivors relied on personal agency and adaptive coping strategies to reclaim autonomy [40, 41]. These included spiritual practices, goal-setting, and use of mobile phones to enhance communication and independence [41]. Hebblethwaite and Curley [40] highlighted how community recreation activities served as meaningful platforms for survivors to reestablish identity and social connection.
Finally, studies examining survivors’ feedback on rehabilitation interventions showed that while structured programs were helpful, many participants preferred person-centered, flexible, and emotionally attuned approaches [36, 53]. Ryan et al. [71] and Huijbregts et al. [53] both reported a mismatch between professional goals and survivor expectations, reinforcing the need for holistic and individualised models of care [36, 53].
Discussion
The present scoping review aimed at mapping the evidence of stroke survivors’ reintegration into community living. The available resources and evidence on factors that determine reintegration into normal living among stroke survivors were highlighted in the scoping review. Different authors described the determinants of stroke survivors’ reintegration into normal living in various ways across studies using both quantitative and qualitative methodologies. RNL is a multifaceted process influenced by the intersection of physical, psychological, and social domains. In the physical domain, mobility functions—specifically gait speed, cadence, and motor recovery—showed strong associations with successful reintegration [8, 56, 82, 83]. Notably, a gait speed threshold of 0.5 m/s appears to be a critical indicator for community-level ambulation [82, 83]. While these findings suggest that maximizing motor recovery before discharge is vital, the cross-sectional nature of most included studies means these should be viewed as correlates rather than direct causes of reintegration.
Evidence from previous studies suggests that balance efficacy and the absence of fear- avoidant behavior are significant determinants of stroke survivors’ community reintegration [56, 77, 86, 87]. Stroke survivors have expressed fear of falls as a barrier to their community reintegration [9]. Most stroke survivors are elderly, and fall risk is reported to be high among the elderly [88, 89]. Thus, this should be addressed before discharge home. All stroke survivors should be prepared for home discharge, focusing on balance efficacy, proper education on fall risk, self-efficacy, and fear-avoidant behavior to enhance better community reintegration. Beyond physical capacity, psychological readiness is paramount. Our review highlights that balance self-efficacy and the absence of fear-avoidant behaviours are significant predictors of participation [56, 77, 86, 87]. Qualitative insights further clarify this, revealing that even survivors with high physical function may withdraw from social spaces due to a fear of falling or the stigma associated with visible disability [9, 43]. This psychological burden is often exacerbated by environmental barriers. Qualitative evidence suggests that uneven terrains and inaccessible public structures do not just hinder physical movement; they actively discourage social participation [37, 38]. Transitioning from institutional care to the home environment requires a shift in focus from "impairment-based" recovery to "environment-specific" adaptation.
It is noteworthy that some included studies reported that an increase in post-stroke duration is a positive predictor of community reintegration among stroke survivors [54, 56, 76]. Stroke survivors have probably mastered their environment, thus limiting the risk of falls and fear-avoidant behaviour. They may improve their motor function over time and can now engage more in physical activities, such as driving a car, which they could not do before. The ability to return to driving a vehicle has been reported as a positive predictor of community reintegration [11, 48]. However, the gains of longer post-stroke duration are reduced by comorbidities associated with stroke incidents. As expected, comorbidities, such as high blood pressure, diabetes, and depression compromized community reintegration among stroke survivors [8, 74, 75, 79]. This suggests that comorbidities should be considered and treated promptly while stroke survivors undergo rehabilitation.
Better social support and improved social status were also discovered to influence good community reintegration among stroke survivors [54, 66, 67, 72, 74, 75]. These underscore the importance of all stakeholders, including spouses, family members, friends, and governments, providing adequate social support. Ease of access to social support for all stroke survivors should be enhanced and promoted by all stakeholders. Efforts should be directed toward rehabilitation to improve post-stroke employment and enhance financial independence, as this may allow survivors to live in higher-income neighbourhoods and achieve higher levels of well-being, all of which have been reported as positive factors for community reintegration [66, 67].
Demographics, such as age and gender were also identified as determinants of community reintegration among stroke survivors. Increased age was associated with poor community reintegration [8, 75]. Probably, older people are more prone to disabilities and more dependent on assistive mobility, which explains the observation. Disabilities and dependence on assistive mobility devices have been noticed to hamper community reintegration [65, 75]. This implies that while preparing older people with stroke for home, all support needed to facilitate smoother community reintegration should be provided, and all factors that could limit it, such as depression, disabilities, and comorbidities, should be addressed before discharge. Though there are conflicting reports about gender influence on community reintegration among stroke survivors, all stroke survivors should be given equal attention while preparing for home.
The home and community environments matter, as they have been suggested to influence reintegration. The focus on transitioning to a home environment during rehabilitation was reported as an enabler of community reintegration [38]. Uneven environmental terrains, altitudes, and inaccessible structures should be addressed before discharge, as these have been reported to hinder community reintegration [37]. The present scoping review highlighted helpful strategies and interventions to support stroke survivors in achieving community reintegration. Strategies, such as occupational performance coaching and family-centred community stroke programs have been documented as enablers of community reintegration among stroke survivors [68, 71]. The success of interventions, such as occupational coaching [68] and telehealth-based self-management [53] likely stems from their ability to provide sustained, contextualised support in the survivor's natural environment. In contrast, 'tune-up' strategies [46]—which are often brief or isolated—may fail because they do not address the complex, evolving psychosocial barriers that survivors face months after discharge. This suggests that for rehabilitation to be effective, it must be longitudinal and adaptive rather than episodic. Adding these strategies will enhance community reintegration, improve quality of life, and provide social support.
The studies included in this scoping review are well distributed across continents and countries, and most are of higher quality. However, a few limitations are worth mentioning. First, the significant heterogeneity of outcome measures—ranging from the RNLI to self-developed questionnaires—hinders the ability to compare findings across different geographic regions. Second, excluding grey literature while maintaining peer-reviewed standards introduces a potential publication bias, particularly by omitting localized policy reports from low- and middle-income countries. Finally, because most included studies were cross-sectional, we cannot definitively establish a temporal causal relationship between the identified determinants and reintegration outcomes.
Conclusion
This scoping review highlights the multifaceted nature of reintegration into normal living among adult stroke survivors, revealing a complex interplay of physical, psychological, social, and environmental determinants. Key factors, such as gait speed, motor function, balance self-efficacy, social support, and post-stroke duration are critical facilitators of success, while comorbidities, depression, environmental inaccessibility, and advanced age remain significant barriers. Although community-based, person-centred interventions involving caregivers show promise, their long-term effectiveness remains unestablished. Furthermore, the heterogeneity of outcome measures and the inconsistent application of validated tools, such as the reintegration to normal living index (RNLI), hinder meaningful cross-study comparisons. To address these gaps, we recommend standardizing reintegration outcome measures to enable global data synthesis. Most critically, the primary research priority moving forward must be the conduct of high-quality RCTs to evaluate scalable, culturally sensitive, community-based interventions, particularly within low- and middle-income countries.
Future research should focus on these underrepresented populations to design interventions that holistically integrate physical, emotional, and social rehabilitation. Ultimately, effective community reintegration must become a central objective of stroke rehabilitation. Stakeholders—including clinicians, policymakers, and community organizations—must work collaboratively to implement evidence-informed strategies that support survivors' return to meaningful roles and improved quality of life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of KwaZulu-Natal, Westville-KZN, South Africa (Code: 00008037).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors drafted the initial protocol, critically reviewed it for intellectual content, subsequently revized it for publication, and read and approved the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
References
Cerebrovascular accident, or more commonly, stroke, is the second most common cause of death and disability worldwide. About 84% of the global stroke burden in 2021 was attributed to 23 modifiable risk factors. High systolic blood pressure remains the single most significant driver, contributing to over 56% of all stroke-related disability-adjusted life years (DALYs) [1]. With increasing sophistication in the medical care of stroke incidents, there is a gradual increase in the number of stroke survivors with stroke-related morbidities. These morbidities have necessitated increased utilization of physical rehabilitation facilities. Neurorehabilitation is often a long process that requires protracted periods of intervention, both in inpatient and outpatient facilities. Care is usually continued at home or community level to adapt the intervention to each survivor’s natural environment. Neuro-rehabilitation services are costly when available in the home environment. This has hindered the reintegration of stroke survivors into the community [2].
Reintegration to normal living (RNL) is one of the essential elements of stroke rehabilitation [3]. It is defined as the ‘reorganisation of physical, psychological, and social characteristics so that the individual can resume well-adjusted living after incapacitating illness or trauma’ [4]. Reintegration into normal living is synonymous with functional status—the individual’s typical performance [5]. The return of stroke survivors to family and community life involves engaging in normal roles and contributing to social groups. This successful transition depends on several complex factors [6–9]. The main determinants of reintegration include individual, physical, psychosocial, and environmental domains. Specifically, depressive symptoms and the perception of overall recovery significantly affect social reintegration [6, 10]. While Obembe et al. [8] also revealed that post-stroke depression was significantly associated with reintegration into normal living, they emphasised that motor recovery was equally crucial for community reintegration. Return to instrumental activities of daily living, such as driving a car, is significantly associated with reintegration into normal living among stroke survivors [11]. In a similar scoping review, Engel-Yeger et al. [7] recommended that participation outcomes be recovered as necessary for stroke survivors’ functional recovery. Wesselhoff et al. [12] in a systematic review reported that stroke survivors’ community mobility was significantly decreased compared to those without any neurological impairment. Community reintegration is a key indicator of participation and community mobility for stroke survivors; hence, more recent research has focused on it.
This review critically examined the evidence on RNL following a stroke. Despite these findings, existing literature often focuses on isolated variables rather than providing a holistic map of how physical and environmental factors intersect in the home environment. There remains a lack of clarity on which specific barriers most significantly impede the transition from clinical recovery to community participation. A scoping review methodology was selected to identify research areas on RNL for stroke survivors, using a range of research approaches, and to identify gaps in the current knowledge base to guide future research in the field.
Materials and Methods
This scoping review was based on the framework outlined by Arksey and O’Malley [13], which includes six iterative steps: (i) identifying the research question, (ii) searching for relevant studies, (iii) selecting the studies, (iv) charting the data, (v) collating, summarising, and reporting the results, and (vi) consulting with stakeholders to inform or validate findings. The sixth step, consultation with relevant stakeholders, remains optional and is considered a valued additional step, but has been excluded from this review. Recommendations made by Levac and colleagues [14] were also considered. The PRISMA extension for a scoping review (PRISMA-ScR) checklist was followed to report this study [15]. This protocol was registered on the Open Science Framework.
Step 1: Identifying the research question
Table 1 illustrates the study's population, concept, and context. This scoping review aimed to answer the following question: “To date, what evidence exists on adult stroke survivor’s RNL?” The sub-questions for this review included the following:
1) To date, what evidence is there on the determinants of reintegration of adult stroke survivors into normal living? 2) What protocols, strategies, and interventions currently facilitate community reintegration for adult stroke survivors? 3) What are the gaps that exist in the reintegration of adult stroke survivors to normal living?
Step 2: Identifying relevant studies
Information Sources: With support from a subject librarian, the authors conducted a systematic search in the following electronic databases: PubMed, cumulated index to nursing and allied health literature (CINAHL), Health source: Nursing/Academic Edition, Web of Science, and Scopus for relevant published literature between January 1995 and December 2024. The initial search was conducted in 2021 and was subsequently updated in January 2025 to include all relevant literature published through December 31, 2024. The search was limited to peer-reviewed English-language articles. Grey literature, including dissertations, policy documents, and unpublished reports, was not included to ensure that the synthesized evidence has undergone rigorous peer review and methodological scrutiny. This study used a comprehensive search strategy that employed keywords, medical subject headings (MeSH), and subject-heading search terms related to key concepts, as well as the Boolean operators “AND” and “OR.” A sample PubMed search is presented in Table 2. A secondary search of relevant articles from the reference lists of the included studies, using a snowball approach, was performed. Training exercises were conducted before the screening process to ensure reliability between reviewers. A single arbitrator/reviewer resolved all discrepancies between reviewers by revisiting the inclusion and exclusion criteria and instituting an additional pilot test. The EndNote reference manager was used to compile all relevant articles and identify duplicate records.
Step 3: Study selection
Eligibility criteria
This review included primary research across various designs, including randomized controlled trials (RCTs), observational studies (cohort and cross-sectional), and qualitative studies, to capture a comprehensive view of reintegration. The study included articles that met the defined eligibility criteria as follows:
Selection process
A thorough title screening was conducted by Michael O Ogunlana and Ifeoma Blessing Nwosu in the electronic databases guided by the eligibility criteria. All relevant articles were imported into an EndNote library, and duplicates were removed. The EndNote library was shared among the review team for the next stage of the study selection process. A screening tool was developed using the eligibility criteria for the abstract and full-text screening phases. Two reviewers (Pragashnie Govender and Michael O Ogunlana) independently conducted abstract and full-text screening and grouped them into “include” or “exclude” categories. Discrepancies between Pragashnie Govender and Michael O Ogunlana during the abstract screening phase were addressed through discussion among the review team until consensus was reached. At the full-text phase, Ifeoma Blessing Nwosu and Olufemi O. Oyewole resolved any discrepancies between Pragashnie Govender and Michael O Ogunlana. Where an article could not be accessed freely online, assistance from the institution’s library services was sought. The original authors were also accessed via email for requests for complete texts, if necessary. Cohen's kappa coefficient (κ) statistic was calculated to determine the inter-rater agreement between the reviewers at the end of the full-text screening phase. The PRISMA flow diagram [16] was adopted to report the screening results, as illustrated in Figure 1.
Step 4: Charting the data
A form was developed in Google Forms for data extraction and piloted to ensure accuracy. After thoroughly reading the full texts, Pragashnie Govender and Michael O Ogunlana extracted all relevant data from the included articles. The data extraction form included the following details: (i) title of the study, (ii) year of publication, (iii) study setting, (iv) aims, (v) country of the study, (vi) study design (vii), study participants (viii), study results, (ix) findings relevant to answer the question, (x) conclusion, and (xi) recommendations. Any discrepancies during data extraction were resolved through discussion among the two extractors (Pragashnie Govender and Michael O Ogunlana), with Olufemi O. Oyewole serving as a third-party arbitrator when consensus could not be reached. The form was continually updated to capture all relevant data to answer the review question.
Step 5: Collating, summarizing, and reporting the results
The review team ensured that the extracted data were exposed to thematic analysis [17]. Relevant themes and sub-themes relating to the study objectives were developed around the following: (i) determinants of reintegration, (ii) protocols, strategies, and interventions available for stroke survivors that assist in community reintegration, and (iii) identified gaps in the successful reintegration of stroke survivors to their relevant communities. This was presented as a narrative of the relevant themes and sub-themes. Where possible, tables and figures were also used to show the results.
Step 6: Methodological quality appraisal
Although not mandatory, the critical appraisal of evidence sources was included in this review to assess methodological quality using the Mixed Methods Appraisal Tool (MMAT) [18]. This instrument has a prescribed set of questions that examine the appropriateness of the different sections reported in each evidence source. A quality score was assigned to each reported study, with ≤50% interpreted as low quality, 51-75% as average quality, and 76-100% as high quality [19]. Two reviewers (Michael O Ogunlana and Olufemi O. Oyewole) independently conducted the quality appraisal to reduce bias. The quality appraisal scores were used to contextualize the strength and reliability of the evidence; however, low-quality studies were not excluded from the thematic analysis, consistent with the inclusive nature of scoping review methodology.
Results
One hundred and fifty-four (154) articles met the eligibility criteria following the deletion of 57 duplicates from the 211 articles identified at the title screening stage, as illustrated in the PRISMA flow diagram (Figure 1). Subsequently, 84 and 16 articles were excluded following abstract and full-text screening, respectively. Reasons for exclusion after full-text screening included: a tool development and validation study in the post-stroke population [20], a tool development and validation study in the post-stroke population [20]; a position paper on the return to driving and reintegration of stroke survivors [21]; Cott et al. [22] wrote a commentary on preparing stroke survivors for reintegration; Jhaveri et al. [23] reported a pilot study on the feasibility of Telerehabilitation for stroke survivors; and Merz et al. [24] reported a factor analysis of the RNL index. Miller et al. [25] published a position paper on the transition of stroke survivors to the home environment, and Plow et al. [26] also published a proposal on a weight management program for stroke survivors. Montgomery et al. [27] and Somerville et al. [28] published protocols on the community reintegration of stroke survivors. Ogourtsova et al. [29] reported clinicians’ opinions on the use of virtual reality in the assessment of hemineglect. Sieber et al. [30] reported an autoethnography on the authors’ personal experience as stroke survivors. Stark et al. [31] reported an unpowered study that examined the feasibility of community-based environmental modification intervention (COMPASS) among stroke survivors. A study [32] reported the inter-rater reliability of the RNL Index; two studies [33, 34] reported the psychometric properties of the subjective index of physical and social outcome (SIPSO); and a study [35] reported the perceptions of stroke survivors about therapeutic relationships and client-centered practice. Overall, 55 studies met the study eligibility criteria for data extraction, including one study identified following an updated search. There was substantial agreement between the reviewers’ responses at the full-text screening stage (Kappa statistic=0.90, P<0.01).
Characteristics of the included studies
The characteristics of the 55 studies included are summarized in Appendices 1, 2 and 3. Ten studies utilized a qualitative methodology [9, 36–44]. A study used a mixed-methodology [45], while the remaining 44 studies used a quantitative methodology. All included studies were published in English between 1995 and 2024. Twenty-two studies [11, 37, 41, 42, 45–62] were conducted in institutionalized settings, like rehabilitation homes, hospitals, and outpatient care, while the remaining 33 studies were conducted in community settings. Of the 55 studies, 17 were conducted in Canada [11, 40, 43–46, 53, 59, 63–71], eight studies were conducted in the USA [39, 48, 49, 58, 62, 72–74], seven studies were conducted in Nigeria [8, 54–56, 61, 75, 76], four studies were conducted in China [47, 60, 77, 78], three studies were conducted in Australia [38, 52, 79], two studies were conducted in each of South Africa [9, 51], and the United Kingdom [80, 81]. One study was conducted in each of these countries: Netherlands [82], Congo [83], India [84], Israel [50], New Zealand [42], Uganda [41], Spain [85], Benin [86], Ireland [57], Scotland [36], Hong Kong [87], and Malawi [37] (Figure 2).
Quality of evidence
The 55 studies underwent methodological quality assessment using the Mixed Methods Appraisal Tool (MMAT software, version 2018) [18]. Out of the 44 included studies that had a quantitative methodology, the methodological quality appraisal score ranged from 50 to 100%, with 15 studies [8, 46, 58, 61–63, 65, 66, 68, 69, 78, 81–83, 85] scored 100%, 26 studies [11, 47–49, 51–57, 60, 64, 67, 70, 72–77, 79, 80, 84, 86, 87] scored 75%, and three studies [50, 59, 71] scored 50%. Ten studies used a qualitative methodology, with quality appraisal scores ranging from 75% to 100%. Three of these studies [37, 38, 41] scored 100%, and 7 of these studies [9, 36, 39, 40, 42–44] scored 75%. The only mixed-method study [45] scored 100%. Methodological limitations were primarily found in quantitative, non-randomized studies, where pre-stroke functional status was often not accounted for as a confounding variable. In qualitative studies, the most common deficit was a lack of transparency regarding 'researcher reflexivity'—how the researchers' own perspectives may have influenced the data collection and analysis.
Study finding
Determinants of stroke survivors' reintegration into normal living
Different authors described the determinants of stroke survivors’ reintegration into normal living in various ways across studies using quantitative methodologies. Some authors described this construct as a predictor of community reintegration; others referred to it as a measure of participation, handicap, satisfaction, and well-being. Mulder et al. [82] concluded that a comfortable gait speed of not less than 0.5 m/s positively predicted community reintegration for stroke survivors. This was supported by other two studies [56, 83]. Mwaka-Rutare et al. [83] reported that higher walking speed improves basic activities of daily living, thereby improving community reintegration, while Olawale et al. [56] focused on increasing cadence (steps per minute) as a positive determinant of community reintegration. Increasing gait speed is also associated with improved motor function, as reported by Obembe et al. [8] as a positive predictor of community reintegration. However, Olawale et al. [56] also reported functional mobility. Hoffman et al. [52] also reported that balance self-efficacy, mobility, and stroke duration positively predict community reintegration. They further identified decreased stride time and fall self-efficacy as negative predictors of community reintegration for stroke survivors.
Some researchers [60, 77, 86, 87] examined the roles of balance self-efficacy, participation self-efficacy, absence of fear-avoidant behaviors, and self-efficacy as positive predictors of community reintegration. Pang et al. [87] reported that balance self-efficacy accounted for 6.5% of the variance of community reintegration. Some studies [54, 56, 76] reported increasing post-stroke duration as a positive predictor of community reintegration; however, only one study [73] reported increasing post-stroke duration as a negative predictor of community reintegration. Demographic variables, such as age and gender were also found to significantly influence community reintegration. Increasing age was unanimously described as a negative predictor of community reintegration for stroke survivors [8, 52, 75]. Being female [79] was a positive predictor of home integration, but Soni et al. [84] concluded that gender was not a determinant of community reintegration among stroke survivors.
Stroke survivors' social status, like living in a higher-income neighbourhood [66], being employed post-stroke [75], having higher levels of well-being through higher incomes [67], and having social (family and spousal) support [54, 65, 72, 74], significantly predicted community reintegration positively. Beckley [72] reported that after controlling for many factors, like age, race, income, and functional limitation, social support was found to be most predictive of community reintegration among stroke survivors. The car driving status was also investigated; researchers [11, 48] reported that the ability to return to driving a car was a positive predictor of community reintegration. The ability to drive post-stroke, when combined with stroke severity, predicted 32% of the possibilities of attaining community reintegration [11], especially among male stroke survivors [48]. The presence of comorbidities, like high blood pressure and T2DM [75], depression/poor emotional health [8, 65, 74, 75, 79], disabilities [65], and dependence on assistive mobility devices [75] were negative predictors of community reintegration. The absence of subjective cognitive complaints was also positively associated with community reintegration [79].
The qualitative research reviewed explored the determinants of community reintegration among stroke survivors. Govender et al. [9] reported the fear of falls and stigma as barriers and family/friend support as enablers to community reintegration. Similarly, Maratos et al. [43] reported that ease of access to social support services, adequate transportation, and accommodation post-stroke enable community reintegration. The need to focus on the transition to a home environment during rehabilitation was reported as an enabler of community reintegration by Gustafsson and Bootle [38], and uneven environmental terrains, altitudes, and inaccessible structures were reported to hinder community reintegration [37]. Kamwesiga et al. [41] reported a focus on the use of mobile phones by stroke survivors as an enabler of social integration that may aid community reintegration. The role of timely education about oriental diets and traditional medicines for stroke survivors' rehabilitation is reported as an enabler of community reintegration [44]. Attainment of rehabilitation goals, like improvement in hand function, balance, driving, and memory are enablers of community reintegration [39]. The use of community-based recreational services is also reported to enhance community reintegration [40]. Accordingly, determinants of reintegration can be categorized into four primary domains: Physical and functional: gait speed and motor recovery were the most frequently cited predictors [8, 56, 82]. Specifically, a gait speed of ≥0.5 m/s served as a critical threshold for community mobility [82, 83]. Psychological: Self-efficacy and the absence of depression were consistently linked to higher participation [8, 65, 87]. Conversely, fear of falling emerged as a primary psychological barrier in qualitative reports [9, 39]. Social: family and spousal support were the strongest predictors of social reintegration across both high- and low-resource settings [54, 72]. Environmental factors, such as car-driving status [11] and neighbourhood income levels [66], significantly influenced the ease of community re-entry. Appendices 1, 2, 3, 4, 5 and 6 present the summary of these findings.
Protocols, strategies, and interventions to support community reintegration for stroke survivors
Thirteen articles reviewed described protocols, strategies, and interventions to support stroke survivors in achieving community reintegration. Kessler et al. [68] reported the usefulness of occupational performance coaching in enhancing stroke survivors' achievement of community reintegration. The family-centred community stroke program [71] improved the perception of leisure competence of stroke survivors and their spouses, and was reported to have enabled reintegration into the community. Different versions of the Improving Participation After Stroke Self-Management (IPASS) contributed to enhancing community reintegration. Harel-Katz et al. [50] used the culturally adapted version of IPASS, while Lee et al. [62] used the rehabilitation version of the IPASS in their article. Huijbregts et al. [53] reported the use of a Telehealth stroke self–management program called Telehealth Moving on After Stroke (T-MOST), which helps enhance community reintegration for stroke survivors.
Multimodal exercise rehabilitation program [85], primary healthcare-based physiotherapy intervention [55], getting on with the rest of your life mission possible [69] community re-engagement cue to action trigger tool - CRCATT [45], community-based recreation [40], and coaching-based Tele-occupational guidance [78] were all documented to have enhanced community reintegration among stroke survivors. Client-centred ‘tune-ups” [46] and Family Support Organizer Program [81] are strategies that did not significantly enhance community reintegration. Intervention efficacy appeared to be influenced by delivery mode and intensity. Programs utilizing Telehealth [53, 78] or intensive coaching [68] reported higher participant engagement and significant RNLI improvements compared to one-off 'tune-up' sessions [46], which lacked the sustained intensity required for long-term behavioural change.
Measures of community reintegration
Most articles (56.4%, 31 out of 55) that qualified for this review utilized the Return to Normal Living Index (RNLI) to measure the extent of community reintegration. Other articles measured community reintegration using a Community Ambulation Questionnaire [82], a Community Integration Questionnaire [79], a Community Integration Measure [77], a Direct Measure of Community Mobility [49], and working speed [85]. The Adapted Maleka Stroke Community Reintegration Measure [54] was used to estimate the extent of community reintegration. Tools used in other research include the return-to-work [57], SIPSOs [46], and post-stroke checklist [47, 70, 80]. While the RNLI was the most frequent measure (57%), it focuses heavily on subjective perception. In contrast, tools, like the SIPSO and Maleka measures showed lower adoption rates, likely due to a lack of extensive psychometric validation across diverse cultural contexts compared to the well-established RNLI.
Quantitative synthesis of results
Of the 44 quantitative studies included in this review, several key determinants of RNL were consistently reported. Motor function and mobility indicators, such as gait speed, cadence, and balance, were among the most frequently assessed variables. These were investigated in approximately 16 studies (36%), and nearly all identified them as strong positive predictors of reintegration outcomes. For example, a gait speed of ≥0.5 m/s was linked to better reintegration in studies by Mulder et al. [82] and Mwaka-Rutare et al. [83], while cadence and motor recovery were emphasized in studies from Nigeria by Olawale et al. [56] and Obembe et al. [8]. Depression and emotional health were examined in at least 6 studies (14%). All of these studies reported negative associations between post-stroke depression and reintegration, suggesting that emotional well-being plays a critical role in post-stroke recovery and community participation [59, 74, 75, 79]. Balance between self-efficacy and confidence in performing daily activities was evaluated in 6 quantitative studies (14%), including those by Pang et al. [87], Liu et al. [77], and Honado et al. [86]. These studies found statistically significant positive relationships between self-efficacy scores and reintegration outcomes.
Social support was identified as a facilitating factor in at least 8 quantitative studies (18%), including those by Egan et al. [67], Okoye et al. [54], and Beckley [72]. These studies highlighted that stroke survivors with strong family or spousal support were significantly more likely to achieve higher reintegration scores. Post-stroke duration was assessed in 5 quantitative studies (11%), with mixed findings. While three studies [56, 75] found that longer duration post-stroke improved reintegration, at least one study [73] indicated a decline over time. Comorbidities, such as hypertension, diabetes, and stroke-related complications were reported as barriers to reintegration in approximately 5 studies (11%), with all of them showing negative associations [75, 79]. Demographic variables, particularly age, were commonly analyzed. Older age was found to negatively impact reintegration in at least 5 studies (11%), including those by Hoffman et al. [52] and Olawale et al. [56]. Gender was reported in several studies but showed no consistent pattern; for instance, Kimonides et al. [79] found gender-specific effects, while Soni et al. [84] found no significant association. Driving ability and return to work as indicators of functional independence were studied in 2–3 quantitative studies (4–7%), such as studies by Finestone et al. [11] and Griffen et al. [48], and were found to have positive correlations with reintegration scores. Interventional studies among the 44 quantitative papers numbered about 13(30%). Most of these interventions—including Telehealth, occupational coaching, and structured self-management—reported statistically significant improvements in reintegration scores post-intervention [53, 62, 68, 71]. However, two studies [46, 81] showed no significant effect, suggesting the need for context-specific or more personalised approaches. Regarding measurement tools, the RNLI was the most frequently used instrument, applied in about 25 of the 44 quantitative studies (57%). Other tools included the SIPSO and the community integration questionnaire, though these were used less consistently.
Qualitative synthesis of results
The qualitative studies included in this review provided deep insights into how stroke survivors experience reintegration into their communities [9, 36, 38, 40, 41, 43, 44, 53, 88]. Emotional, social, and environmental dimensions were consistently highlighted as shaping the reintegration process.
A key theme across several studies was the emotional complexity of reintegration [9, 36, 43]. Survivors often expressed fear, anxiety, and frustration about resuming social and occupational roles [9, 43]. For example, Govender et al. [9] emphasized that fear of falling and social stigma restricted survivors’ community mobility, even in the presence of good physical recovery. Similarly, Maratos et al. [43] reported that high-functioning survivors withdrew from public spaces due to internalized emotional and psychological challenges.
Environmental and societal barriers were another frequent theme [9, 36, 41, 88]. Studies conducted in low-resource settings, such as Malawi [88] and Uganda [41], identified poor infrastructure, inaccessible public transport, and lack of rehabilitation continuity as key constraints. These structural limitations restricted survivors’ ability to fully participate in community life [41, 88]. Brookfield et al. [36] also described how physical environments could either facilitate or obstruct reintegration, depending on their design and accessibility.
Social relationships emerged as a vital component of successful reintegration [38, 44, 53]. Survivors emphasized the importance of family, caregivers, and peers in supporting their transition from rehabilitation to home and community [38, 44]. In Yeung et al.’s study [44] involving Chinese-Canadian stroke survivors, family support was essential to rebuilding confidence and promoting functional participation. In contrast, the absence of such support was linked to emotional isolation and reduced community participation [44]. Some studies reported that survivors relied on personal agency and adaptive coping strategies to reclaim autonomy [40, 41]. These included spiritual practices, goal-setting, and use of mobile phones to enhance communication and independence [41]. Hebblethwaite and Curley [40] highlighted how community recreation activities served as meaningful platforms for survivors to reestablish identity and social connection.
Finally, studies examining survivors’ feedback on rehabilitation interventions showed that while structured programs were helpful, many participants preferred person-centered, flexible, and emotionally attuned approaches [36, 53]. Ryan et al. [71] and Huijbregts et al. [53] both reported a mismatch between professional goals and survivor expectations, reinforcing the need for holistic and individualised models of care [36, 53].
Discussion
The present scoping review aimed at mapping the evidence of stroke survivors’ reintegration into community living. The available resources and evidence on factors that determine reintegration into normal living among stroke survivors were highlighted in the scoping review. Different authors described the determinants of stroke survivors’ reintegration into normal living in various ways across studies using both quantitative and qualitative methodologies. RNL is a multifaceted process influenced by the intersection of physical, psychological, and social domains. In the physical domain, mobility functions—specifically gait speed, cadence, and motor recovery—showed strong associations with successful reintegration [8, 56, 82, 83]. Notably, a gait speed threshold of 0.5 m/s appears to be a critical indicator for community-level ambulation [82, 83]. While these findings suggest that maximizing motor recovery before discharge is vital, the cross-sectional nature of most included studies means these should be viewed as correlates rather than direct causes of reintegration.
Evidence from previous studies suggests that balance efficacy and the absence of fear- avoidant behavior are significant determinants of stroke survivors’ community reintegration [56, 77, 86, 87]. Stroke survivors have expressed fear of falls as a barrier to their community reintegration [9]. Most stroke survivors are elderly, and fall risk is reported to be high among the elderly [88, 89]. Thus, this should be addressed before discharge home. All stroke survivors should be prepared for home discharge, focusing on balance efficacy, proper education on fall risk, self-efficacy, and fear-avoidant behavior to enhance better community reintegration. Beyond physical capacity, psychological readiness is paramount. Our review highlights that balance self-efficacy and the absence of fear-avoidant behaviours are significant predictors of participation [56, 77, 86, 87]. Qualitative insights further clarify this, revealing that even survivors with high physical function may withdraw from social spaces due to a fear of falling or the stigma associated with visible disability [9, 43]. This psychological burden is often exacerbated by environmental barriers. Qualitative evidence suggests that uneven terrains and inaccessible public structures do not just hinder physical movement; they actively discourage social participation [37, 38]. Transitioning from institutional care to the home environment requires a shift in focus from "impairment-based" recovery to "environment-specific" adaptation.
It is noteworthy that some included studies reported that an increase in post-stroke duration is a positive predictor of community reintegration among stroke survivors [54, 56, 76]. Stroke survivors have probably mastered their environment, thus limiting the risk of falls and fear-avoidant behaviour. They may improve their motor function over time and can now engage more in physical activities, such as driving a car, which they could not do before. The ability to return to driving a vehicle has been reported as a positive predictor of community reintegration [11, 48]. However, the gains of longer post-stroke duration are reduced by comorbidities associated with stroke incidents. As expected, comorbidities, such as high blood pressure, diabetes, and depression compromized community reintegration among stroke survivors [8, 74, 75, 79]. This suggests that comorbidities should be considered and treated promptly while stroke survivors undergo rehabilitation.
Better social support and improved social status were also discovered to influence good community reintegration among stroke survivors [54, 66, 67, 72, 74, 75]. These underscore the importance of all stakeholders, including spouses, family members, friends, and governments, providing adequate social support. Ease of access to social support for all stroke survivors should be enhanced and promoted by all stakeholders. Efforts should be directed toward rehabilitation to improve post-stroke employment and enhance financial independence, as this may allow survivors to live in higher-income neighbourhoods and achieve higher levels of well-being, all of which have been reported as positive factors for community reintegration [66, 67].
Demographics, such as age and gender were also identified as determinants of community reintegration among stroke survivors. Increased age was associated with poor community reintegration [8, 75]. Probably, older people are more prone to disabilities and more dependent on assistive mobility, which explains the observation. Disabilities and dependence on assistive mobility devices have been noticed to hamper community reintegration [65, 75]. This implies that while preparing older people with stroke for home, all support needed to facilitate smoother community reintegration should be provided, and all factors that could limit it, such as depression, disabilities, and comorbidities, should be addressed before discharge. Though there are conflicting reports about gender influence on community reintegration among stroke survivors, all stroke survivors should be given equal attention while preparing for home.
The home and community environments matter, as they have been suggested to influence reintegration. The focus on transitioning to a home environment during rehabilitation was reported as an enabler of community reintegration [38]. Uneven environmental terrains, altitudes, and inaccessible structures should be addressed before discharge, as these have been reported to hinder community reintegration [37]. The present scoping review highlighted helpful strategies and interventions to support stroke survivors in achieving community reintegration. Strategies, such as occupational performance coaching and family-centred community stroke programs have been documented as enablers of community reintegration among stroke survivors [68, 71]. The success of interventions, such as occupational coaching [68] and telehealth-based self-management [53] likely stems from their ability to provide sustained, contextualised support in the survivor's natural environment. In contrast, 'tune-up' strategies [46]—which are often brief or isolated—may fail because they do not address the complex, evolving psychosocial barriers that survivors face months after discharge. This suggests that for rehabilitation to be effective, it must be longitudinal and adaptive rather than episodic. Adding these strategies will enhance community reintegration, improve quality of life, and provide social support.
The studies included in this scoping review are well distributed across continents and countries, and most are of higher quality. However, a few limitations are worth mentioning. First, the significant heterogeneity of outcome measures—ranging from the RNLI to self-developed questionnaires—hinders the ability to compare findings across different geographic regions. Second, excluding grey literature while maintaining peer-reviewed standards introduces a potential publication bias, particularly by omitting localized policy reports from low- and middle-income countries. Finally, because most included studies were cross-sectional, we cannot definitively establish a temporal causal relationship between the identified determinants and reintegration outcomes.
Conclusion
This scoping review highlights the multifaceted nature of reintegration into normal living among adult stroke survivors, revealing a complex interplay of physical, psychological, social, and environmental determinants. Key factors, such as gait speed, motor function, balance self-efficacy, social support, and post-stroke duration are critical facilitators of success, while comorbidities, depression, environmental inaccessibility, and advanced age remain significant barriers. Although community-based, person-centred interventions involving caregivers show promise, their long-term effectiveness remains unestablished. Furthermore, the heterogeneity of outcome measures and the inconsistent application of validated tools, such as the reintegration to normal living index (RNLI), hinder meaningful cross-study comparisons. To address these gaps, we recommend standardizing reintegration outcome measures to enable global data synthesis. Most critically, the primary research priority moving forward must be the conduct of high-quality RCTs to evaluate scalable, culturally sensitive, community-based interventions, particularly within low- and middle-income countries.
Future research should focus on these underrepresented populations to design interventions that holistically integrate physical, emotional, and social rehabilitation. Ultimately, effective community reintegration must become a central objective of stroke rehabilitation. Stakeholders—including clinicians, policymakers, and community organizations—must work collaboratively to implement evidence-informed strategies that support survivors' return to meaningful roles and improved quality of life.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of KwaZulu-Natal, Westville-KZN, South Africa (Code: 00008037).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors drafted the initial protocol, critically reviewed it for intellectual content, subsequently revized it for publication, and read and approved the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
References
- Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J, Lindsay P, et al. World stroke organization: global stroke fact sheet 2025. Int J Stroke. 2025; 20(2):132-44. [DOI:10.1177/17474930241308142] [PMID]
- Jennum P, Iversen HK, Ibsen R, Kjellberg J. Cost of stroke: A controlled national study evaluating societal effects on patients and their partners. BMC Health Serv Res. 2015; 15:466. [DOI:10.1186/s12913-015-1100-0] [PMID]
- Bhogal SK, Teasell RW, Foley NC, Speechley MR. Community reintegration after stroke. Top Stroke Rehabil. 2003; 10(2):107-29. [DOI:10.1310/F50L-WEWE-6AJ4-64FK] [PMID]
- Wood-Dauphinee S, Williams JI. Reintegration to normal living as a proxy to quality of life. J Chronic Dis. 1987; 40(6):491-502. [DOI:10.1016/0021-9681(87)90005-1] [PMID]
- World Health Organization. International classification of functioning, disability and health (ICF) [Internet]. 2001 [Updated 25 Feb 2022]. Available from: [Link]
- Baseman S, Fisher K, Ward L, Bhattacharya A. The relationship of physical function to social integration after stroke. J Neurosci Nurs. 2010; 42(5):237-44. [DOI:10.1097/JNN.0b013e3181ecafea] [PMID]
- Engel-Yeger B, Tse T, Josman N, Baum C, Carey LM. Scoping review: The trajectory of recovery of participation outcomes following stroke. Behav Neurol. 2018; 2018:5472018. [DOI:10.1155/2018/5472018] [PMID]
- Obembe A, Mapayi B, Johnson O, Agunbiade T, Emechete A. Community reintegration in stroke survivors: Relationship with motor function and depression. Hong Kong Physiother J. 2013; 31(2):69-74. [DOI:10.1016/j.hkpj.2013.04.001]
- Govender P, Naidoo D, Bricknell K, Ayob Z, Message H, Njoko S. 'No one prepared me to go home': Cerebrovascular accident survivors' experiences of community reintegration in a peri-urban context. Afr J Prim Health Care Fam Med. 2019; 11(1):e1-8. [DOI:10.4102/phcfm.v11i1.1806] [PMID]
- Murtezani A, Hundozi H, Gashi S, Osmani T, Krasniqi V, Rama B. Factors associated with reintegration to normal living after stroke. Med Arh. 2009; 63(4):216-9. [Link]
- Finestone HM, Guo M, O'Hara P, Greene-Finestone L, Marshall SC, Hunt L, et al. Driving and reintegration into the community in patients after stroke. PM R. 2010; 2(6):497-503. [DOI:10.1016/j.pmrj.2010.03.030] [PMID]
- Wesselhoff S, Hanke TA, Evans CC. Community mobility after stroke: A systematic review. Top Stroke Rehabil. 2018; 25(3):224-38. [DOI:10.1080/10749357.2017.1419617] [PMID]
- Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Method. 2005; 8:19-32. [DOI:10.1080/1364557032000119616]
- Levac D, Colquhoun H, O'Brien KK. Scoping studies: Advancing the methodology. Implement Sci. 2010; 5:69. [DOI:10.1186/1748-5908-5-69] [PMID]
- Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018; 169(7):467-73. [DOI:10.7326/M18-0850] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. [DOI:10.1136/bmj.n71] [PMID]
- Saldana J. The coding manual for qualitative researchers. fourth. Thousand Oaks: SAGE Publications Ltd; 2021. [Link]
- Hong QN, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018; 34(4):285-91. [DOI:10.3233/EFI-180221]
- Kalideen L, Govender P, van Wyk JM, Kuupiel D. Mapping evidence on standards and quality of care for older persons in long-term care facilities: A scoping review protocol. Syst Rev. 2021; 10(1):153. [DOI:10.1186/s13643-021-01709-2] [PMID]
- Babulal GM, Tabor Connor L. The measure of stroke environment (MOSE): Development and validation of the MOSE in post-stroke populations with and without aphasia. Top Stroke Rehabil. 2016; 23(5):348-57. [DOI:10.1080/10749357.2016.1143697] [PMID]
- Burns SP, Schwartz JK, Scott SL, Devos H, Kovic M, Hong I, et al. Interdisciplinary approaches to facilitate return to driving and return to work in mild stroke: A position paper. Arch Phys Med Rehabil. 2018; 99(11):2378-88. [DOI:10.1016/j.apmr.2018.01.032] [PMID]
- Cott CA, Wiles R, Devitt R. Continuity, transition and participation: preparing clients for life in the community post-stroke. Disabil Rehabil. 2007; 29(20-21):1566-74.[DOI:10.1080/09638280701618588] [PMID]
- Jhaveri MM, Benjamin-Garner R, Rianon N, Sherer M, Francisco G, Vahidy F, et al. Telemedicine-guided education on secondary stroke and fall prevention following inpatient rehabilitation for Texas patients with stroke and their caregivers: A feasibility pilot study. BMJ Open. 2017; 7(9):e017340. [DOI:10.1136/bmjopen-2017-017340] [PMID]
- Merz ZC, Van Patten R, Mulhauser K, Fucetola R. Exploratory factor analysis of the reintegration to normal living index in a stroke population. Top Stroke Rehabil. 2017; 24(2):158-62. [DOI:10.1080/10749357.2016.1215398] [PMID]
- Miller KK, Lin SH, Neville M. From hospital to home to participation: A position paper on transition planning poststroke. Arch Phys Med Rehabil. 2019; 100(6):1162-75. [DOI:10.1016/j.apmr.2018.10.017] [PMID]
- Plow M, Moore SM, Kirwan JP, Frost F, Katzan I, Jaeger S, et al. Randomized controlled pilot study of a SystemCHANGE™ weight management intervention in stroke survivors: Rationale and protocol. Trials. 2013; 14:130. [DOI:10.1186/1745-6215-14-130] [PMID]
- Montgomery P, Jermyn D, Bailey P, Nangia P, Egan M, Mossey S. Community reintegration of stroke survivors: The effect of a community navigation intervention. J Adv Nurs. 2015; 71(1):214-25. [DOI:10.1111/jan.12471] [PMID]
- Somerville E, Minor B, Keglovits M, Yan Y, Stark S. Effect of a novel transition program on disability after stroke: A trial protocol. JAMA Netw Open. 2019; 2(10):e1912356. [DOI:10.1001/jamanetworkopen.2019.12356] [PMID]
- Ogourtsova T, Archambault PS, Lamontagne A. Exploring barriers and facilitators to the clinical use of virtual reality for post-stroke unilateral spatial neglect assessment. Disabil Rehabil. 2019; 41(3):284-92. [DOI:10.1080/09638288.2017.1387292] [PMID]
- Sieber R. Return to university after a stroke: An autoethnography. Am J Occup Ther. 2018; 72 (4_Supplement_1):7211515284p1. [DOI:10.5014/ajot.2018.72S1-PO7028]
- Stark S, Keglovits M, Somerville E, Hu YL, Conte J, et al. Feasibility of a novel intervention to improve participation after stroke. Br J Occup Ther. 2018; 81(2):116-24. [DOI:10.1177/0308022617736704] [PMID]
- Tooth LR, McKenna KT, Smith M, O'Rourke PK. Reliability of scores between stroke patients and significant others on the reintegration to normal living (RNL) index. Disabil Rehabil. 2003; 25(9):433-40. [DOI:10.1080/0963828031000069726] [PMID]
- Trigg R, Wood VA. The subjective index of physical and social outcome (SIPSO): A new measure for use with stroke patients. Clin Rehabil. 2000; 14(3):288-99. [DOI:10.1191/026921500678119607] [PMID]
- Trigg R, Wood VA. The validation of the subjective index of physical and social outcome (SIPSO). Clin Rehabil. 2003; 17(3):283-9. [DOI:10.1191/0269215503cr609oa] [PMID]
- Walder K, Molineux M. Listening to the client voice - A constructivist grounded theory study of the experiences of client-centred practice after stroke. Aust Occup Ther J. 2020; 67(2):100-9.[DOI:10.1111/1440-1630.12627] [PMID]
- Brookfield K, Mead G. Physical environments and community reintegration post stroke: Qualitative insights from stroke clubs. Disabil Soc. 2016; 31:1013-29. [DOI:10.1080/09687599.2016.1223606]
- Chimatiro G, Rhoda A. Environmental barriers to reintegration experienced by stroke clients post discharge from a rehabilitation centre in Malawi. S Afri J Physiother. 2014; 70:18-23. [DOI:10.4102/sajp.v70i1.260]
- Gustafsson L, Bootle K. Client and carer experience of transition home from inpatient stroke rehabilitation. Disabil Rehabil. 2013; 35(16):1380-6. [DOI:10.3109/09638288.2012.740134] [PMID]
- Hay CC, Pappadis MR, Sander AM, Weller SC, Wang W, Reistetter TA. Important-performance analysis to conceptualize goal priorities in community dwelling stroke survivors. Top Stroke Rehabil. 2022; 29(4):310-20. [DOI:10.1080/10749357.2021.1928838] [PMID]
- Hebblethwaite S, Curley L. Exploring the role of community recreation in stroke recovery using participatory action research and photovoice. Ther Recreation J. 2015; 49(1):1-17. [Link]
- Kamwesiga JT, Tham K, Guidetti S. Experiences of using mobile phones in everyday life among persons with stroke and their families in Uganda - A qualitative study. Disabil Rehabil. 2017; 39(5):438-49. [DOI:10.3109/09638288.2016.1146354] [PMID]
- Lemke M, Rodríguez Ramírez E, Robinson B, Signal N. Motivators and barriers to using information and communication technology in everyday life following stroke: A qualitative and video observation study. Disabil Rehabil. 2020; 42(14):1954-62. [DOI:10.1080/09638288.2018.1543460] [PMID]
- Maratos M, Huynh L, Tan J, Lui J, Jarus T. Picture this: Exploring the lived experience of high-functioning stroke survivors using photovoice. Qual Health Res. 2016; 26(8):1055-66. [DOI:10.1177/1049732316648114] [PMID]
- Yeung EH, Szeto A, Richardson D, Lai SH, Lim E, Cameron JI. The experiences and needs of Chinese-Canadian stroke survivors and family caregivers as they re-integrate into the community. Health Soc Care Community. 2015; 23(5):523-31. [DOI:10.1111/hsc.12164] [PMID]
- McKellar J, Cheung D, Huijbregts M, Cameron J. The impact of a community re-engagement cue to action trigger tool on re-engaging in activities post-stroke: A mixed-methods study. Top Stroke Rehabil. 2015; 22(2):134-43. [DOI:10.1179/1074935714Z.0000000038] [PMID]
- Brouwer B, Bryant D, Garland SJ. Effectiveness of client-centered "tune-ups" on community reintegration, mobility, and quality of life after stroke: A randomized controlled trial. Arch Phys Med Rehabil. 2018; 99(7):1325-32. [DOI:10.1016/j.apmr.2017.12.034] [PMID]
- Chau JPC, Lo SHS, Zhao J, Choi KC, Lam SKY, Butt L, et al. Factors associated with post-stroke depression in chinese stroke survivors. J Stroke Cerebrovasc Dis. 2021; 30(11):106076. [DOI:10.1016/j.jstrokecerebrovasdis.2021.106076] [PMID]
- Griffen JA, Rapport LJ, Bryer RC, Scott CA. Driving status and community integration after stroke. Top Stroke Rehabil. 2009; 16(3):212-21. [DOI:10.1310/tsr1603-212] [PMID]
- Hanke TA, Hwang S, Keller S, Zielke D, Hailey T, Nathaniel K, et al. Measuring community mobility in survivors of stroke using global positioning system technology: A prospective observational study. J Neurol Phys Ther. 2019; 43(3):175-85. [DOI:10.1097/NPT.0000000000000279] [PMID]
- Harel-Katz H, Adar T, Milman U, Carmeli E. Examining the feasibility and effectiveness of a culturally adapted participation-focused stroke self-management program in a day-rehabilitation setting: A randomized pilot study. Top Stroke Rehabil. 2020; 27(8):577-89. [DOI:10.1080/10749357.2020.1738676] [PMID]
- Hassan S, Visagie S, Mji G. The achievement of community integration and productivity outcomes by CVA survivors in the western cape metro health district. S h Afr J Occup Ther. 2012; 42:11-6. [Link]
- Hoffmann T, McKenna K, Cooke D, Tooth L. Outcomes after stroke: Basic and instrumental activities of daily living, community reintegration and generic health status. Aust Occup Ther J. 2003; 50(4):225-33. [DOI:10.1046/j.1440-1630.2003.00376.x]
- Huijbregts MP, McEwen S, Taylor D. Exploring the feasibility and efficacy of a telehealth stroke self-management programme: A pilot study. Physiother Can. 2009; 61(4):210-20. [DOI:10.3138/physio.61.4.210] [PMID]
- Okoye EC, Okoro SC, Akosile CO, Onwuakagba IU, Ihegihu EY, Ihegihu CC. Informal caregivers' well-being and care recipients' quality of life and community reintegration - findings from a stroke survivor sample. Scand J Caring Sci. 2019; 33(3):641-50. [DOI:10.1111/scs.12657] [PMID]
- Olaleye OA, Hamzat TK, Owolabi MO. Development and evaluation of the primary healthcare-based physiotherapy Intervention and its effects on selected indices of stroke recovery. Int J Ther Rehabil. 2013; 20(9):443-9. [DOI:10.12968/ijtr.2013.20.9.443]
- Olawale OA, Usman JS, Oke KI, Osundiya OC. Evaluation of predictive factors influencing community reintegration in adult patients with stroke. J Neurosci Rural Pract. 2018; 9(1):6-10. [DOI:10.4103/jnrp.jnrp_386_17] [PMID]
- Walsh ME, Galvin R, Loughnane C, Macey C, Horgan NF. Community reintegration and long-term need in the first five years after stroke: results from a national survey. Disabil Rehabil. 2015;37:1834-8. [DOI:10.3109/09638288.2014.981302] [PMID]
- Wolf T, Brey J, Baum C, Connor L. Activity participation differences between younger and older individuals with stroke. Brain Impairment. 2012; 13(1):16-23. [DOI:10.1017/BrImp.2012.1]
- Kapoor A, Lanctôt KL, Bayley M, Kiss A, Herrmann N, Murray BJ, et al. "Good outcome" isn't good enough: cognitive impairment, depressive symptoms, and social restrictions in physically recovered stroke patients. Stroke. 2017; 48(6):1688-90. [DOI:10.1161/STROKEAHA.117.016728] [PMID]
- Lo SHS, Chau JPC, Lam SKY, Saran R, Choi KC, Zhao J, et al. Association between participation self-efficacy and participation in stroke survivors. BMC Neurol. 2022; 22(1):361. [DOI:10.1186/s12883-022-02883-z] [PMID]
- Olaleye OA, Hamzat TK, Owolabi MO. Stroke rehabilitation: Should physiotherapy intervention be provided at a primary health care centre or the patients' place of domicile? Disabil Rehabil. 2014; 36(1):49-54. [DOI:10.3109/09638288.2013.777804] [PMID]
- Lee D, Fischer H, Zera S, Robertson R, Hammel J. Examining a participation-focused stroke self-management intervention in a day rehabilitation setting: A quasi-experimental pilot study. Top Stroke Rehabil. 2017; 24(8):601-7. [DOI:10.1080/10749357.2017.1375222] [PMID]
- Allen L, McIntyre A, Janzen S, Richardson M, Meyer M, Ure D, et al. Community stroke rehabilitation: How do rural residents fare compared with their urban counterparts? Can J Neurol Sci. 2016; 43(1):98-104. [DOI:10.1017/cjn.2015.324] [PMID]
- Bluvol A, Ford-Gilboe M. Hope, health work and quality of life in families of stroke survivors. J Adv Nurs. 2004; 48(4):322-32. [DOI:10.1111/j.1365-2648.2004.03004.x] [PMID]
- Clarke PJ, Black SE, Badley EM, Lawrence JM, Williams JI. Handicap in stroke survivors. Disabil Rehabil. 1999; 21(3):116-23. [DOI:10.1080/096382899297855] [PMID]
- Egan M, Kubina LA, Dubouloz CJ, Kessler D, Kristjansson E, Sawada M. Very low neighbourhood income limits participation post stroke: Preliminary evidence from a cohort study. BMC Public Health. 2015; 15:528. [DOI:10.1186/s12889-015-1872-5] [PMID]
- Egan M, Davis CG, Dubouloz CJ, Kessler D, Kubina LA. Participation and well-being poststroke: Evidence of reciprocal effects. Arch Phys Med Rehabil. 2014; 95(2):262-8. [DOI:10.1016/j.apmr.2013.08.013] [PMID]
- Kessler D, Egan M, Dubouloz CJ, McEwen S, Graham FP. Occupational performance coaching for stroke survivors: A pilot randomized controlled trial. Am J Occup Ther. 2017; 71(3):7103190020p1-7. [DOI:10.5014/ajot.2017.024216] [PMID]
- Mayo NE, Anderson S, Barclay R, Cameron JI, Desrosiers J, Eng JJ, et al. Getting on with the rest of your life following stroke: A randomized trial of a complex intervention aimed at enhancing life participation post stroke. Clin Rehabil. 2015; 29(12):1198-211. [DOI:10.1177/0269215514565396] [PMID]
- Parks NE, Eskes GA, Gubitz GJ, Reidy Y, Christian C, Phillips SJ. Fatigue impact scale demonstrates greater fatigue in younger stroke survivors. Can J Neurol Sci. 2012; 39(5):619-25. [DOI:10.1017/S0317167100015353] [PMID]
- Ryan CA, Stiell KM, Gailey GF, Makinen JA. Evaluating a family centered approach to leisure education and community reintegration following a stroke. Ther Recreat J. 2008; 42(2):119. [Link]
- Beckley MN. The influence of the quality and quantity of social support in the promotion of community participation following stroke. Aust Occup Ther J. 2007; 54:215-20. [DOI:10.1111/j.1440-1630.2007.00643.x]
- Béthoux F, Calmels P, Gautheron V. Changes in the quality of life of hemiplegic stroke patients with time: A preliminary report. Am J Phys Med Rehabil. 1999; 78(1):19-23. [DOI:10.1097/00002060-199901000-00006] [PMID]
- Ianni C, Magee L, Dagli C, Nicholas ML, Connor LT. Self-reported emotional health and social support but not executive function are associated with participation after stroke. Top Stroke Rehabil. 2023; 30(6):568-77. [DOI:10.1080/10749357.2022.2110192] [PMID]
- Akosile C, Nworah C, Okoye E, Adegoke B, Umunnah J, Fabunmi A. Community reintegration and related factors in a Nigerian stroke sample. Afr Health Sci. 2016; 16(3):772-80. [DOI:10.4314/ahs.v16i3.18] [PMID]
- Obembe A, Fasuyi T. Community reintegration in Nigerian stroke survivors. Int J Stroke. 2010; 5(5):428. [DOI:10.1111/j.1747-4949.2010.00477.x] [PMID]
- Liu TW, Ng SS, Kwong PW, Ng GY. Fear avoidance behavior, not walking endurance, predicts the community reintegration of community-dwelling stroke survivors. Arch Phys Med Rehabil. 2015; 96(9):1684-90. [DOI:10.1016/j.apmr.2015.05.005] [PMID]
- Zhang L, Yan YN, Sun ZX, Yan DR, Chen YW, Lin KC, et al. Effects of coaching-based teleoccupational guidance for home-based stroke survivors and their family caregivers: A pilot randomised controlled trial. Int J Environ Res Public Health. 2022; 19(23):16355. [DOI:10.3390/ijerph192316355] [PMID]
- Kimonides S, Cavuoto MG, De Silva L, Kinsella GJ. The role of subjective cognitive complaints and depressive symptoms in social re-integration following stroke: A mediation explanation in a cross-sectional sample. Top Stroke Rehabil. 2018; 1-7. [DOI:10.1080/10749357.2018.1489570] [PMID]
- Crow J. A 2-week stroke review identifies unmet needs in patients discharged home from a hyperacute stroke unit. Br J Neurosci Nurs. 2018; 14:29-35. [DOI:10.12968/bjnn.2018.14.1.29]
- Tilling K, Coshall C, McKevitt C, Daneski K, Wolfe C. A family support organiser for stroke patients and their carers: A randomised controlled trial. Cerebrovasc Dis. 2005; 20(2):85-91. [DOI:10.1159/000086511] [PMID]
- Mulder M, Nijland RH, van de Port IG, van Wegen EE, Kwakkel G. Prospectively classifying community walkers after stroke: Who are they? Arch Phys Med Rehabil. 2019; 100(11):2113-8. [DOI:10.1016/j.apmr.2019.04.017] [PMID]
- Mwaka-Rutare C, Perreault K, Abedi-Mukutenga P, Masuga-Musafiri W, Batcho CS. Activity and participation in stroke survivors in a low-income setting: A cross-sectional study. Physiother Res Int. 2020; 25(4):e1846. [DOI:10.1002/pri.1846] [PMID]
- Soni M, Patel P, Amin D, Mahla R. Gender specific comparison of activity limitation, participation restriction and community re integration among stroke patients. Ind J Physiother Occup Ther. 2019; 13(1):155–9.
- Grau-Pellicer M, Chamarro-Lusar A, Medina-Casanovas J, Serdà Ferrer BC. Walking speed as a predictor of community mobility and quality of life after stroke. Top Stroke Rehabil. 2019; 26(5):349-358. [DOI:10.1080/10749357.2019.1605751] [PMID]
- Honado AS, Atigossou OLG, Roy JS, Daneault JF, Batcho CS. Relationships between self-efficacy and post-stroke activity limitations, locomotor ability, physical activity, and community reintegration in Sub-Saharan Africa: A cross-sectional study. Int J Environ Res Public Health. 2023; 20(3):2286. [DOI:10.3390/ijerph20032286] [PMID]
- Pang MYC, Eng JJ, Miller WC. Determinants of satisfaction with community reintegration in older adults with chronic stroke: role of balance self-efficacy. Phys Ther. 2007; 87:282-91. [DOI:10.2522/ptj.20060142] [PMID]
- Whitney DG, Dutt-Mazumder A, Peterson MD, Krishnan C. Fall risk in stroke survivors: effects of stroke plus dementia and reduced motor functional capacity. J Neurol Sci. 2019; 401:95-100. [DOI:10.1016/j.jns.2019.04.035] [PMID]
- Wing JJ, Burke JF, Clarke PJ, Feng C, Skolarus LE. The role of the environment in falls among stroke survivors. Arch Gerontol Geriatr. 2017; 72:1-5. [DOI:10.1016/j.archger.2017.04.007] [PMID]
Type of Study: Review Article |
Subject:
Rehabilitation management
Received: 2026/01/7 | Accepted: 2026/02/18 | Published: 2026/03/10
Received: 2026/01/7 | Accepted: 2026/02/18 | Published: 2026/03/10
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.