

Volume 9, Issue 1 (Continuously Updated- In press 2026)
Func Disabil J 2026, 9(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Barati M, Namiranian K, Jafar Zibaei M, Haddadi J, Taghipour M. Prevalence of Musculoskeletal Disorders Among Physiotherapists in Mazandaran Province: A Cross-sectional Study. Func Disabil J 2026; 9 (1)
URL: http://fdj.iums.ac.ir/article-1-342-en.html
URL: http://fdj.iums.ac.ir/article-1-342-en.html
Mostafa Barati1 

 , Kiarash Namiranian2 , Mohammad Jafar Zibaei3 , Javad Haddadi4 , Mohammad Taghipour *5
, Kiarash Namiranian2 , Mohammad Jafar Zibaei3 , Javad Haddadi4 , Mohammad Taghipour *5
, Kiarash Namiranian2 , Mohammad Jafar Zibaei3 , Javad Haddadi4 , Mohammad Taghipour *5
1- Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Physiotherapy, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Semnan University of Medical Sciences, Semnan, Iran.
5- Mobility Impairment Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,taghipour@mubabol.ac.ir
2- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Physiotherapy, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Semnan University of Medical Sciences, Semnan, Iran.
5- Mobility Impairment Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,
Full-Text [PDF 492 kb]
(7 Downloads)
| Abstract (HTML) (61 Views)
Full-Text: (3 Views)
Introduction
Musculoskeletal disorders (MSDs) are impairments of the musculoskeletal system that primarily arise from occupational activities and workplace conditions [1]. Globally, nearly 1.7 billion people are affected by musculoskeletal problems that significantly limit mobility and agility, reduce quality of life, and often result in early retirement and social participation restrictions [2]. These disorders have become a major cause of workforce reduction in many occupational groups [3]. MSDs commonly involve the joints, muscles, tendons, and nerves, and although they can affect any part of the body, the upper limbs, neck, and back are the most frequently impacted regions [4]. MSDs represent a serious occupational health problem among healthcare workers, particularly nurses and physiotherapists [5]. Near half (47%) of physiotherapists experience MSDs during the first five years of their careers, largely due to insufficient experience in maintaining proper posture during treatment sessions [6].
The development of these disorders is multifactorial, influenced by biomechanical, psychosocial, organizational, individual, and environmental factors [3]. Psychosocial stressors, such as excessive workload, inadequate support from colleagues and supervisors, and high job strain can increase susceptibility to MSDs. Likewise, repetitive movements, poor posture, frequent bending, lifting and transferring patients, and the application of continuous or excessive force place mechanical stress on the body and raise the risk of injury [1, 7]. Prolonged use of specific body parts in certain professions may predispose individuals to MSDs in those areas. Without adequate prevention, such conditions can lead to pain, disability, and significant economic burden for both workers and society. Physiotherapists—despite being experts in treating these conditions—are themselves exposed to high physical strain due to awkward postures, manual therapy, and frequent patient transfers, all of which may contribute to musculoskeletal injuries. Previous studies have identified heavy workload and younger age (below 30 years) as risk factors for these disorders, while incorrect hand positioning is considered a major cause of neuromusculoskeletal problems [8]. Inadequate preventive measures and poor recognition of work-related injuries among physiotherapists can cause gradual reduction of manual work, ultimately affecting both treatment quality and patient outcomes [9]. Researchers have proposed practical strategies to minimize occupational strain, such as adjusting daily activities, engaging in leisure or exercise breaks [10], improving workplace conditions, taking rest periods between treatment sessions, and using height-adjustable treatment tables, lifting belts, transfer boards, splints, or wheelchairs, as well as delegating tasks to assistants and alternating body regions during manual therapy [11].
Given the growing number of rehabilitation professionals and increasing public awareness of the benefits of physiotherapy—which together result in higher workloads and longer working hours—the likelihood of MSDs among physiotherapists in Iran is expected to rise [8]. Mazandaran Province, one of Iran’s largest and most populous regions, has a substantial physiotherapy workforce, yet no prior research has examined the prevalence of these disorders in this population. Therefore, this study aimed to determine the prevalence of MSDs in different body regions and to identify the associated factors among physiotherapists in Mazandaran Province.
Materials and Methods
Study design
This descriptive cross-sectional study titled “prevalence of MSDs among physiotherapists in Mazandaran province” was conducted among licensed physiotherapists working in clinical and hospital settings across the province.
Participants and sampling
A complete list of all active and licensed physiotherapists in Mazandaran Province was obtained from official medical registries and used as the sampling frame. All eligible physiotherapists were contacted either in person or electronically and were invited to participate.
Inclusion criteria were holding at least a bachelor’s degree in physiotherapy, active professional practice, and no history of MSDs unrelated to work. Exclusion criteria included a history of musculoskeletal surgery, congenital deformities, neurological or rheumatologic conditions, oncologic diseases, or incomplete questionnaire data.
The required sample size was calculated using the single-population proportion formula with an assumed prevalence of 50%, a 95% confidence level, and a 10% margin of error, resulting in a minimum of 100 participants. To account for potential non-response, more individuals were approached, and of the 110 physiotherapists initially contacted, 101 returned fully completed questionnaires, yielding a response rate of 91.8%. While the possibility of nonresponse bias cannot be entirely excluded, the high response rate reduces the likelihood that prevalence estimates were substantially affected by non-participation.
Data collection
Data were collected using the validated Persian version of the extended Nordic musculoskeletal questionnaire (ENMQ) [12, 13], which assesses the presence of musculoskeletal symptoms in nine body regions over the previous 12 months. The Persian version of this questionnaire has demonstrated satisfactory validity and test re-test reliability [13]. MSDs were defined as self-reported musculoskeletal symptoms perceived to be associated with work tasks or conditions. The questionnaire assessed the presence of symptoms within the past 12 months, consistent with the standard ENMQ structure. Participants also reported whether symptoms interfered with daily activities or work duties, although no direct measurement of pain severity (e.g. VAS score) or days of absenteeism was included. Participants completed the questionnaires anonymously after being informed about the study objectives, confidentiality, and voluntary participation. Both printed and electronic versions of the questionnaire were used to maximize response rate.
Statistical analysis
All data were analyzed using SPSS software, version 24. Descriptive statistics (Mean±SD, and frequency distribution) were used to summarize demographic and clinical characteristics. Associations between categorical variables were assessed using chi-square test or Fisher’s exact test, while independent-sample t-tests were employed to examine relationships between continuous variables (e.g. age) and MSD prevalence. Missing data were handled using pairwise deletion. A significance level of P<0.05 was used for all analyses. Given the exploratory nature of the study, no adjustments were applied for multiple comparisons or potential confounding variables.
Results
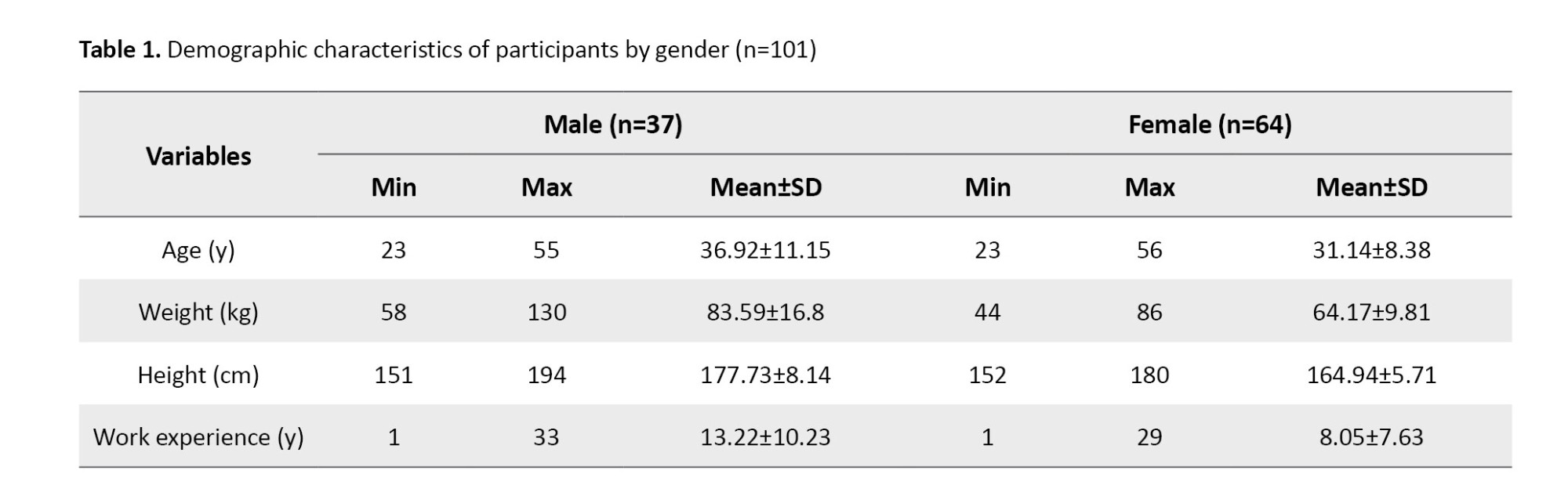
A total of 101 physiotherapists participated in this study, including 64 females (63.4%) and 37 males (36.6%). The mean age of female participants was 31.1±8.3 years (range: 23–56), while that of males was 36.9±11.1 years (range: 23–55). The mean work experience was 8.0±7.6 years for females and 13.2±10.2 years for males.
Demographic characteristics
Among the participants, 90(89.1%) were right-handed and 11(10.9%) left-handed. In terms of marital status, 51(50.5%) were single and 50(49.5%) were married. Regarding educational level, 59.4% of females and 37.8% of males held bachelor’s degrees, while 34.4% of females and 45.9% of males had master’s degrees. Table 1 presents the demographic characteristics of participants by gender.
Prevalence of MSDs
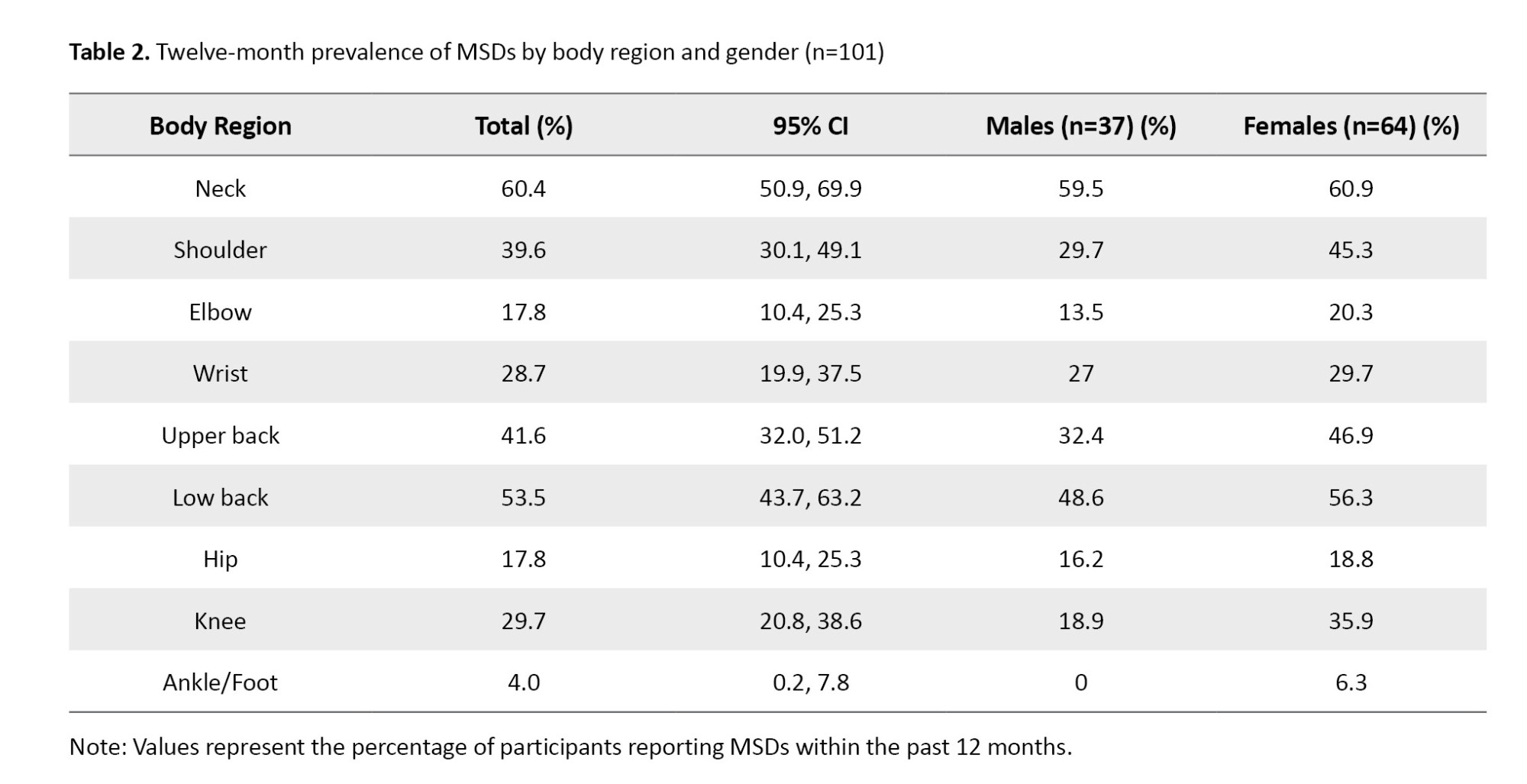
The overall prevalence of MSDs among participants was high. The neck region showed the highest prevalence (60.4%), followed by the low back (53.5%), upper back (41.6%), and shoulder (39.6%). The ankle/foot (4%) was the least affected region. Table 2 summarizes the prevalence of MSDs by body region and gender.
The prevalence pattern was similar across genders, with slightly higher rates in females in most body regions.
Statistical associations
The independent t-test revealed a significant association between age and wrist pain (P=0.014), indicating that the prevalence of wrist disorders increased with age. However, no significant relationships were observed between MSD prevalence and gender, education level, or hand dominance (P>0.05 for all comparisons).
These findings demonstrate that MSDs are common among physiotherapists, particularly affecting the neck, low back, and upper limbs, and that age is a contributing factor for wrist disorders.
Discussion
The present study showed a high prevalence of MSDs among physiotherapists in Mazandaran Province, particularly in the neck, low back, and upper back. Although this pattern is similar to reports from previous national and international research, methodological differences limit direct comparison. Variations in sampling approaches, workplace environments, and participant characteristics may partly explain discrepancies between studies. International studies often focused solely on hospital-based physiotherapists, whereas the current research included both clinical and private-practice settings with different physical demands. Given the repetitive movements, manual therapy techniques, awkward postures, and prolonged standing required in physiotherapy, it is not surprising that the musculoskeletal system—especially the spine and upper extremities—is subjected to considerable mechanical stress.
The present study indicated that the neck (60.4%) and low back (53.5%) are the most commonly affected regions. Similar trends were reported by Rahimi et al. [6] and Vieira et al. [14], who found high rates of spinal complaints associated with static postures and repetitive manual handling. Abdollahi et al. [15] also reported that shoulder and wrist symptoms were frequent among Iranian physiotherapists, largely due to ergonomic strain and improper hand positioning during treatment procedures.
Although female participants reported slightly higher symptom rates, the present study did not identify any significant gender-related differences. This result aligns with observations by Khairy et al. [7] and Muaidi and Shanb [16], who reported that gender does not play a major role in the development of MSDs among physiotherapists. These consistent patterns suggest that occupational exposure, rather than demographic factors, is the primary determinant of risk.
The present study also showed a significant association between age and wrist pain (P=0.014). Older physiotherapists may experience increased symptoms due to cumulative mechanical load and long-term involvement in manual therapy activities. Similar interpretations were reported by Rozenfeld et al. [10], who noted that repetitive use of the upper limbs and increased professional experience contribute to the development of wrist and hand disorders.
No significant associations were observed between MSD prevalence and factors, such as education level, hand dominance, or marital status. This reinforces the idea that occupational demands outweigh demographic characteristics in influencing MSD occurrence. The high rate of spinal complaints further highlights the need for preventive ergonomic strategies. Physiotherapists often adopt non-neutral postures—including forward head position, trunk flexion, and rounded shoulders—which increase strain on cervical and lumbar structures. Additionally, transferring force primarily through the upper limbs rather than engaging the trunk may lead to overuse injuries in the wrists, elbows, and shoulders. Promoting ergonomic awareness is therefore essential. Rahimi et al. [6] reported that improved knowledge of body mechanics can reduce work-related symptoms among rehabilitation professionals. Periodic ergonomic training, the use of height-adjustable treatment tables and transfer-assist devices, and adequate rest intervals may effectively reduce physical strain. Overall, the present study confirms the widespread occurrence of MSDs among physiotherapists and emphasizes the need for preventive measures focused on ergonomic practice, workload modification, and physical conditioning to support long-term occupational health.
Conclusion
The present study highlights the substantial burden of MSDs among physiotherapists in Mazandaran Province, underscoring the impact of repetitive manual tasks and non-neutral postures on their occupational health. Although demographic variables showed no meaningful associations with MSD occurrence, the relationship between age and wrist symptoms suggests a cumulative effect of long-term clinical practice. These findings emphasize the importance of integrating ergonomic principles into daily physiotherapy routines. Implementing regular rest breaks, optimizing workstation design, and providing ongoing training in body mechanics may help reduce the risk of MSDs and support safer, more sustainable clinical practice.
Limitations
This study has several limitations. First, its cross-sectional design does not allow for establishing causal relationships between occupational factors and MSDs. Second, data were collected using self-reported questionnaires, which may be subject to recall bias and under- or over-reporting of symptoms. Third, the 12-month recall period may have affected the accuracy of symptom prevalence. Additionally, the study included only physiotherapists who agreed to participate, which may introduce selection bias. Finally, the sample was limited to one province, which may restrict the generalizability of the findings to physiotherapists in other regions of Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Babol University of Medical Sciences, Babol, Iran (Code: IR.MUBABOL.REC.1399.516). All ethical principles were strictly followed in this research. Participation was voluntary, and all participants provided written informed consent prior to data collection. Confidentiality and anonymity of participants were fully guaranteed. Participants were informed of their right to access the study results upon completion.
Funding
This article is extracted from a research project of Babol University of Medical Sciences, Babol, Iran (Project Code: 724132886) and financially supported by Babol University of Medical Sciences, Babol, Iran (Grant No.: 724132886).
Authors' contributions
Conceptualization, supervision, and writing the original draft: Mohammad Taghipour and Mostafa Barati; Methodology: Kiarash Namiranian, Mohammad Jafar Zibaei, and Javad Haddadi; Investigation, review and editing: All authors; Funding acquisition, and resources: Mohammad Taghipour.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all physiotherapists in Mazandaran Province who participated in this study for their valuable time and cooperation.
References
Musculoskeletal disorders (MSDs) are impairments of the musculoskeletal system that primarily arise from occupational activities and workplace conditions [1]. Globally, nearly 1.7 billion people are affected by musculoskeletal problems that significantly limit mobility and agility, reduce quality of life, and often result in early retirement and social participation restrictions [2]. These disorders have become a major cause of workforce reduction in many occupational groups [3]. MSDs commonly involve the joints, muscles, tendons, and nerves, and although they can affect any part of the body, the upper limbs, neck, and back are the most frequently impacted regions [4]. MSDs represent a serious occupational health problem among healthcare workers, particularly nurses and physiotherapists [5]. Near half (47%) of physiotherapists experience MSDs during the first five years of their careers, largely due to insufficient experience in maintaining proper posture during treatment sessions [6].
The development of these disorders is multifactorial, influenced by biomechanical, psychosocial, organizational, individual, and environmental factors [3]. Psychosocial stressors, such as excessive workload, inadequate support from colleagues and supervisors, and high job strain can increase susceptibility to MSDs. Likewise, repetitive movements, poor posture, frequent bending, lifting and transferring patients, and the application of continuous or excessive force place mechanical stress on the body and raise the risk of injury [1, 7]. Prolonged use of specific body parts in certain professions may predispose individuals to MSDs in those areas. Without adequate prevention, such conditions can lead to pain, disability, and significant economic burden for both workers and society. Physiotherapists—despite being experts in treating these conditions—are themselves exposed to high physical strain due to awkward postures, manual therapy, and frequent patient transfers, all of which may contribute to musculoskeletal injuries. Previous studies have identified heavy workload and younger age (below 30 years) as risk factors for these disorders, while incorrect hand positioning is considered a major cause of neuromusculoskeletal problems [8]. Inadequate preventive measures and poor recognition of work-related injuries among physiotherapists can cause gradual reduction of manual work, ultimately affecting both treatment quality and patient outcomes [9]. Researchers have proposed practical strategies to minimize occupational strain, such as adjusting daily activities, engaging in leisure or exercise breaks [10], improving workplace conditions, taking rest periods between treatment sessions, and using height-adjustable treatment tables, lifting belts, transfer boards, splints, or wheelchairs, as well as delegating tasks to assistants and alternating body regions during manual therapy [11].
Given the growing number of rehabilitation professionals and increasing public awareness of the benefits of physiotherapy—which together result in higher workloads and longer working hours—the likelihood of MSDs among physiotherapists in Iran is expected to rise [8]. Mazandaran Province, one of Iran’s largest and most populous regions, has a substantial physiotherapy workforce, yet no prior research has examined the prevalence of these disorders in this population. Therefore, this study aimed to determine the prevalence of MSDs in different body regions and to identify the associated factors among physiotherapists in Mazandaran Province.
Materials and Methods
Study design
This descriptive cross-sectional study titled “prevalence of MSDs among physiotherapists in Mazandaran province” was conducted among licensed physiotherapists working in clinical and hospital settings across the province.
Participants and sampling
A complete list of all active and licensed physiotherapists in Mazandaran Province was obtained from official medical registries and used as the sampling frame. All eligible physiotherapists were contacted either in person or electronically and were invited to participate.
Inclusion criteria were holding at least a bachelor’s degree in physiotherapy, active professional practice, and no history of MSDs unrelated to work. Exclusion criteria included a history of musculoskeletal surgery, congenital deformities, neurological or rheumatologic conditions, oncologic diseases, or incomplete questionnaire data.
The required sample size was calculated using the single-population proportion formula with an assumed prevalence of 50%, a 95% confidence level, and a 10% margin of error, resulting in a minimum of 100 participants. To account for potential non-response, more individuals were approached, and of the 110 physiotherapists initially contacted, 101 returned fully completed questionnaires, yielding a response rate of 91.8%. While the possibility of nonresponse bias cannot be entirely excluded, the high response rate reduces the likelihood that prevalence estimates were substantially affected by non-participation.
Data collection
Data were collected using the validated Persian version of the extended Nordic musculoskeletal questionnaire (ENMQ) [12, 13], which assesses the presence of musculoskeletal symptoms in nine body regions over the previous 12 months. The Persian version of this questionnaire has demonstrated satisfactory validity and test re-test reliability [13]. MSDs were defined as self-reported musculoskeletal symptoms perceived to be associated with work tasks or conditions. The questionnaire assessed the presence of symptoms within the past 12 months, consistent with the standard ENMQ structure. Participants also reported whether symptoms interfered with daily activities or work duties, although no direct measurement of pain severity (e.g. VAS score) or days of absenteeism was included. Participants completed the questionnaires anonymously after being informed about the study objectives, confidentiality, and voluntary participation. Both printed and electronic versions of the questionnaire were used to maximize response rate.
Statistical analysis
All data were analyzed using SPSS software, version 24. Descriptive statistics (Mean±SD, and frequency distribution) were used to summarize demographic and clinical characteristics. Associations between categorical variables were assessed using chi-square test or Fisher’s exact test, while independent-sample t-tests were employed to examine relationships between continuous variables (e.g. age) and MSD prevalence. Missing data were handled using pairwise deletion. A significance level of P<0.05 was used for all analyses. Given the exploratory nature of the study, no adjustments were applied for multiple comparisons or potential confounding variables.
Results
A total of 101 physiotherapists participated in this study, including 64 females (63.4%) and 37 males (36.6%). The mean age of female participants was 31.1±8.3 years (range: 23–56), while that of males was 36.9±11.1 years (range: 23–55). The mean work experience was 8.0±7.6 years for females and 13.2±10.2 years for males.
Demographic characteristics
Among the participants, 90(89.1%) were right-handed and 11(10.9%) left-handed. In terms of marital status, 51(50.5%) were single and 50(49.5%) were married. Regarding educational level, 59.4% of females and 37.8% of males held bachelor’s degrees, while 34.4% of females and 45.9% of males had master’s degrees. Table 1 presents the demographic characteristics of participants by gender.
Prevalence of MSDs
The overall prevalence of MSDs among participants was high. The neck region showed the highest prevalence (60.4%), followed by the low back (53.5%), upper back (41.6%), and shoulder (39.6%). The ankle/foot (4%) was the least affected region. Table 2 summarizes the prevalence of MSDs by body region and gender.
The prevalence pattern was similar across genders, with slightly higher rates in females in most body regions.
Statistical associations
The independent t-test revealed a significant association between age and wrist pain (P=0.014), indicating that the prevalence of wrist disorders increased with age. However, no significant relationships were observed between MSD prevalence and gender, education level, or hand dominance (P>0.05 for all comparisons).
These findings demonstrate that MSDs are common among physiotherapists, particularly affecting the neck, low back, and upper limbs, and that age is a contributing factor for wrist disorders.
Discussion
The present study showed a high prevalence of MSDs among physiotherapists in Mazandaran Province, particularly in the neck, low back, and upper back. Although this pattern is similar to reports from previous national and international research, methodological differences limit direct comparison. Variations in sampling approaches, workplace environments, and participant characteristics may partly explain discrepancies between studies. International studies often focused solely on hospital-based physiotherapists, whereas the current research included both clinical and private-practice settings with different physical demands. Given the repetitive movements, manual therapy techniques, awkward postures, and prolonged standing required in physiotherapy, it is not surprising that the musculoskeletal system—especially the spine and upper extremities—is subjected to considerable mechanical stress.
The present study indicated that the neck (60.4%) and low back (53.5%) are the most commonly affected regions. Similar trends were reported by Rahimi et al. [6] and Vieira et al. [14], who found high rates of spinal complaints associated with static postures and repetitive manual handling. Abdollahi et al. [15] also reported that shoulder and wrist symptoms were frequent among Iranian physiotherapists, largely due to ergonomic strain and improper hand positioning during treatment procedures.
Although female participants reported slightly higher symptom rates, the present study did not identify any significant gender-related differences. This result aligns with observations by Khairy et al. [7] and Muaidi and Shanb [16], who reported that gender does not play a major role in the development of MSDs among physiotherapists. These consistent patterns suggest that occupational exposure, rather than demographic factors, is the primary determinant of risk.
The present study also showed a significant association between age and wrist pain (P=0.014). Older physiotherapists may experience increased symptoms due to cumulative mechanical load and long-term involvement in manual therapy activities. Similar interpretations were reported by Rozenfeld et al. [10], who noted that repetitive use of the upper limbs and increased professional experience contribute to the development of wrist and hand disorders.
No significant associations were observed between MSD prevalence and factors, such as education level, hand dominance, or marital status. This reinforces the idea that occupational demands outweigh demographic characteristics in influencing MSD occurrence. The high rate of spinal complaints further highlights the need for preventive ergonomic strategies. Physiotherapists often adopt non-neutral postures—including forward head position, trunk flexion, and rounded shoulders—which increase strain on cervical and lumbar structures. Additionally, transferring force primarily through the upper limbs rather than engaging the trunk may lead to overuse injuries in the wrists, elbows, and shoulders. Promoting ergonomic awareness is therefore essential. Rahimi et al. [6] reported that improved knowledge of body mechanics can reduce work-related symptoms among rehabilitation professionals. Periodic ergonomic training, the use of height-adjustable treatment tables and transfer-assist devices, and adequate rest intervals may effectively reduce physical strain. Overall, the present study confirms the widespread occurrence of MSDs among physiotherapists and emphasizes the need for preventive measures focused on ergonomic practice, workload modification, and physical conditioning to support long-term occupational health.
Conclusion
The present study highlights the substantial burden of MSDs among physiotherapists in Mazandaran Province, underscoring the impact of repetitive manual tasks and non-neutral postures on their occupational health. Although demographic variables showed no meaningful associations with MSD occurrence, the relationship between age and wrist symptoms suggests a cumulative effect of long-term clinical practice. These findings emphasize the importance of integrating ergonomic principles into daily physiotherapy routines. Implementing regular rest breaks, optimizing workstation design, and providing ongoing training in body mechanics may help reduce the risk of MSDs and support safer, more sustainable clinical practice.
Limitations
This study has several limitations. First, its cross-sectional design does not allow for establishing causal relationships between occupational factors and MSDs. Second, data were collected using self-reported questionnaires, which may be subject to recall bias and under- or over-reporting of symptoms. Third, the 12-month recall period may have affected the accuracy of symptom prevalence. Additionally, the study included only physiotherapists who agreed to participate, which may introduce selection bias. Finally, the sample was limited to one province, which may restrict the generalizability of the findings to physiotherapists in other regions of Iran.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Babol University of Medical Sciences, Babol, Iran (Code: IR.MUBABOL.REC.1399.516). All ethical principles were strictly followed in this research. Participation was voluntary, and all participants provided written informed consent prior to data collection. Confidentiality and anonymity of participants were fully guaranteed. Participants were informed of their right to access the study results upon completion.
Funding
This article is extracted from a research project of Babol University of Medical Sciences, Babol, Iran (Project Code: 724132886) and financially supported by Babol University of Medical Sciences, Babol, Iran (Grant No.: 724132886).
Authors' contributions
Conceptualization, supervision, and writing the original draft: Mohammad Taghipour and Mostafa Barati; Methodology: Kiarash Namiranian, Mohammad Jafar Zibaei, and Javad Haddadi; Investigation, review and editing: All authors; Funding acquisition, and resources: Mohammad Taghipour.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all physiotherapists in Mazandaran Province who participated in this study for their valuable time and cooperation.
References
- Govaerts R, Tassignon B, Ghillebert J, Serrien B, De Bock S, Ampe T, et al. Prevalence and incidence of work-related musculoskeletal disorders in secondary industries of 21st century Europe: A systematic review and meta-analysis. BMC Musculoskelet Disord. 2021; 22(1):751. [DOI:10.1186/s12891-021-04615-9] [PMID]
- WHO. Musculoskeletal conditions [Internet]. 2022 [Updated 2022 July 14]. Available from: [Link]
- Yang F, Di N, Guo WW, Ding WB, Jia N, Zhang H, et al. The prevalence and risk factors of work related musculoskeletal disorders among electronics manufacturing workers: A cross-sectional analytical study in China. BMC Public Health. 2023; 23(1):10. [DOI:10.1186/s12889-022-14952-6] [PMID]
- Levy BS. Occupational and environmental health: Recognizing and preventing disease and injury. Philadelphia: Lippincott Williams & Wilkins; 2006. [Link]
- Bryndal A, Glowinski S, Grochulska A. Influence of occupation on the prevalence of spinal pain among physiotherapists and nurses. J Clin Med. 2022; 11(19):5600. [DOI:10.3390/jcm11195600] [PMID]
- Rahimi F, Kazemi K, Zahednejad S, López-López D, Calvo-Lobo C. Prevalence of work-related musculoskeletal disorders in Iranian physical therapists: A cross-sectional study. J Manipulative Physiol Ther. 2018; 41(6):503-7. [DOI:10.1016/j.jmpt.2018.02.003] [PMID]
- Khairy WA, Bekhet AH, Sayed B, Elmetwally SE, Elsayed AM, Jahan AM. Prevalence, profile, and response to work-related musculoskeletal disorders among Egyptian physiotherapists. Open Access Maced J Med Sci. 2019; 7(10):1692-9. [DOI:10.3889/oamjms.2019.335] [PMID]
- Amini M, Shamili A, Yarahmadi R, Jafari H. [A systematic review of work-related problems among occupational therapists and physical therapists (Persian)]. Modern Rehabil. 2012; 6(1):1-11. [Link]
- Tennent TD, Beach WR, Meyers JF. A review of the special tests associated with shoulder examination. Part I: The rotator cuff tests. Am J Sports Med. 2003; 31(1):154-60. [DOI:10.1177/03635465030310011101] [PMID]
- Rozenfeld V, Ribak J, Danziger J, Tsamir J, Carmeli E. Prevalence, risk factors and preventive strategies in work-related musculoskeletal disorders among Israeli physical therapists. Physiother Res Int. 2010; 15(3):176-84. [DOI:10.1002/pri.440] [PMID]
- Chung SH, Her JG, Ko T, Ko J, Kim H, Lee JS, et al. Work-related musculoskeletal disorders among Korean physical therapists. J Phys Ther Sci. 2013; 25(1):55-9. [DOI:10.1589/jpts.25.55]
- Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987; 18(3):233-7. [DOI:10.1016/0003-6870(87)90010-X] [PMID]
- Mokhtarinia H, Shafiee A, Pashmdarfard M. Translation and localization of the extended Nordic musculoskeletal questionnaire and the evaluation of the face validity and test-retest reliability of its Persian version. J Ergon. 2015; 3(3):21-9. [Link]
- Vieira ER, Schneider P, Guidera C, Gadotti IC, Brunt D. Work-related musculoskeletal disorders among physical therapists: A systematic review. J Back Musculoskelet Rehabil. 2016; 29(3):417-28. [DOI:10.3233/BMR-150649] [PMID]
- Abdollahi I, Mohseni Bandpei M, Firoozi S. [The prevalence of upper extremity disorders in physiotherapists of Tehran City (Persian)]. J Rehabil. 2012; 12(4):47-53. [Link]
- Muaidi QI, Shanb AA. Prevalence causes and impact of work related musculoskeletal disorders among physical therapists. J Back Musculoskelet Rehabil. 2016; 29(4):763-9. [DOI:10.3233/BMR-160687] [PMID]
Type of Study: Research |
Subject:
Physiotherapy
Received: 2025/10/28 | Accepted: 2025/12/8 | Published: 2026/03/11
Received: 2025/10/28 | Accepted: 2025/12/8 | Published: 2026/03/11
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.