

Volume 9, Issue 1 (Continuously Updated- In press 2026)
Func Disabil J 2026, 9(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Najafpour M, Heydari S, Salehi R. Exploring Causal Factors of Rehabilitation Dropout From the Perspectives of People With Disabilities and Rehabilitation Service Providers: A Qualitative Study. Func Disabil J 2026; 9 (1)
URL: http://fdj.iums.ac.ir/article-1-333-en.html
URL: http://fdj.iums.ac.ir/article-1-333-en.html



1- Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. & Rehabilitation Research Center, Iran University of Medical Sciences, Tehran, Iran. ,samaheidari@gmail.com
2- Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. & Rehabilitation Research Center, Iran University of Medical Sciences, Tehran, Iran. ,
Keywords: Rehabilitation adherence, Patient dropouts, Disabled persons, Health services accessibility, Financial barriers, Psychological factors
Full-Text [PDF 603 kb]
(119 Downloads)
| Abstract (HTML) (289 Views)
Full-Text: (52 Views)
Introduction
Rehabilitation, as an essential component of the health system and a fundamental human right, plays a key role in improving the quality of life for individuals with disabilities. The World Health Organization (WHO) identifies disability not only as a health issue but also as a development priority and part of human rights [1]. The global initiative “rehabilitation 2030” also emphasizes raising awareness, expanding access to rehabilitation services, and reducing costs [2]. With the increasing prevalence of disability, particularly in developing countries, equitable access to rehabilitation services has become more critical than ever [3].
In general, the treatment and rehabilitation of any disease or disability involve several main stages. These include raising awareness about the disease process and related risk factors, screening for the disease, associated risks or comorbidities, diagnosis, treatment, adherence to prescribed treatment, and control or improvement [4]. In this regard, adherence and continuation of treatment are crucial for achieving effective outcomes. Studies have shown that regular and uninterrupted participation in rehabilitation sessions is one of the most important factors in improving the condition of individuals with various disabilities [5, 6]. Furthermore, consistent participation in rehabilitation contributes to greater independence, reduced dependency, and has a cost-effective impact from an economic perspective [5, 6]. Timely interventions significantly increase their effectiveness [7]. In addition to direct and obvious costs, discontinuing treatment is also a risk factor for a range of adverse and secondary health outcomes [8, 9].
Despite the clear need for persistence and adherence in rehabilitation, some individuals with disabilities [10], or parents and caregivers of children with disabilities, may express dissatisfaction with rehabilitation for various reasons and in some cases withdraw their children from ongoing rehabilitation programs [11]. This issue becomes particularly problematic when early intervention is required, for instance, in children with developmental delays or similar conditions, where the window of opportunity for intervention is limited.
Health plays a crucial role in development, and for individuals with disabilities, achieving the highest possible level of health and quality of life depends on adherence to rehabilitation programs. Regular attendance at rehabilitation sessions enhances treatment effectiveness, reduces economic costs, and improves individual functioning. This is especially important for children and individuals with cognitive disabilities. Given the lack of comprehensive studies on the reasons behind dropout of rehabilitation treatments, the present study aimed to examine the factors influencing this issue from the perspective of individuals with disabilities and rehabilitation service providers.
Materials and Methods
This qualitative study, conducted using conventional content analysis with an inductive approach, explored the experiences and perspectives of individuals with disabilities and rehabilitation service providers regarding the reasons for discontinuation of treatment programs in Tehran.
Participants were selected purposefully, with maximum variation in variables, such as type of disability, age, gender, and level of education, to gather a comprehensive range of views and experiences. Inclusion criteria for individuals with disabilities were having attended at least three rehabilitation sessions, discontinuation of services for a period of three months or more after starting rehabilitation, and willingness to participate in interviews. For service providers, inclusion criteria were possession of a valid medical license in one of the three mentioned fields and at least two years of professional experience. Ineffective cooperation during interviews or voluntary withdrawal were considered exclusion criteria.
Data were collected through in-depth, semi-structured interviews. The interview guide consisted of open-ended, exploratory questions focusing on barriers to continuing rehabilitation services (for example, “What made you stop attending rehabilitation sessions? Please explain.”). The duration of the interviews ranged from 10 to 48 minutes. Prior to participation, written informed consent was obtained from all participants. The time and location of the sessions were mutually agreed upon and conducted in a quiet, calm environment. Participants were free to withdraw from the study at any stage and could contact the interviewer for clarification of any questions. Audio files were securely stored in protected folders with password access. The sampling process lasted for approximately 6 months.
All interviews were audio-recorded and transcribed verbatim. They were then analyzed using conventional content analysis based on the method of Graneheim and Lundman [12]. Initial coding, categorization, and theme extraction were carried out by Mohammad Najafpour. The process included repeated reading of the transcripts to gain an overall understanding, identifying meaning units, condensing and abstracting them, and assigning codes. Subsequently, the codes were compared for similarities and differences, grouped into subcategories, and finally organized into broader categories.
To ensure trustworthiness of the data, Lincoln and Guba’s four criteria were applied: Transferability (through the selection of diverse participants), dependability (rechecking the codes with other researchers), confirmability (review of the results by several research team members), and credibility (through field notes and in-depth analysis of interview transcripts) [13].
Results
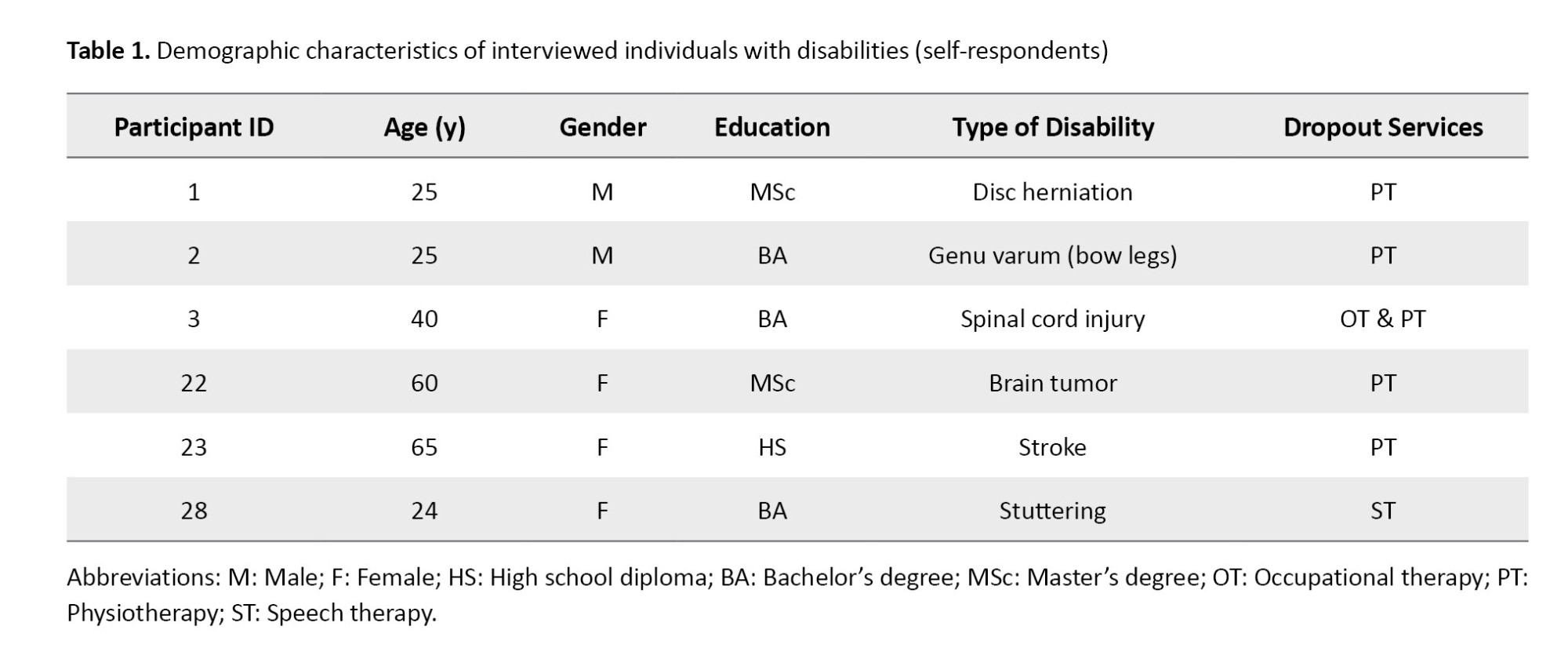
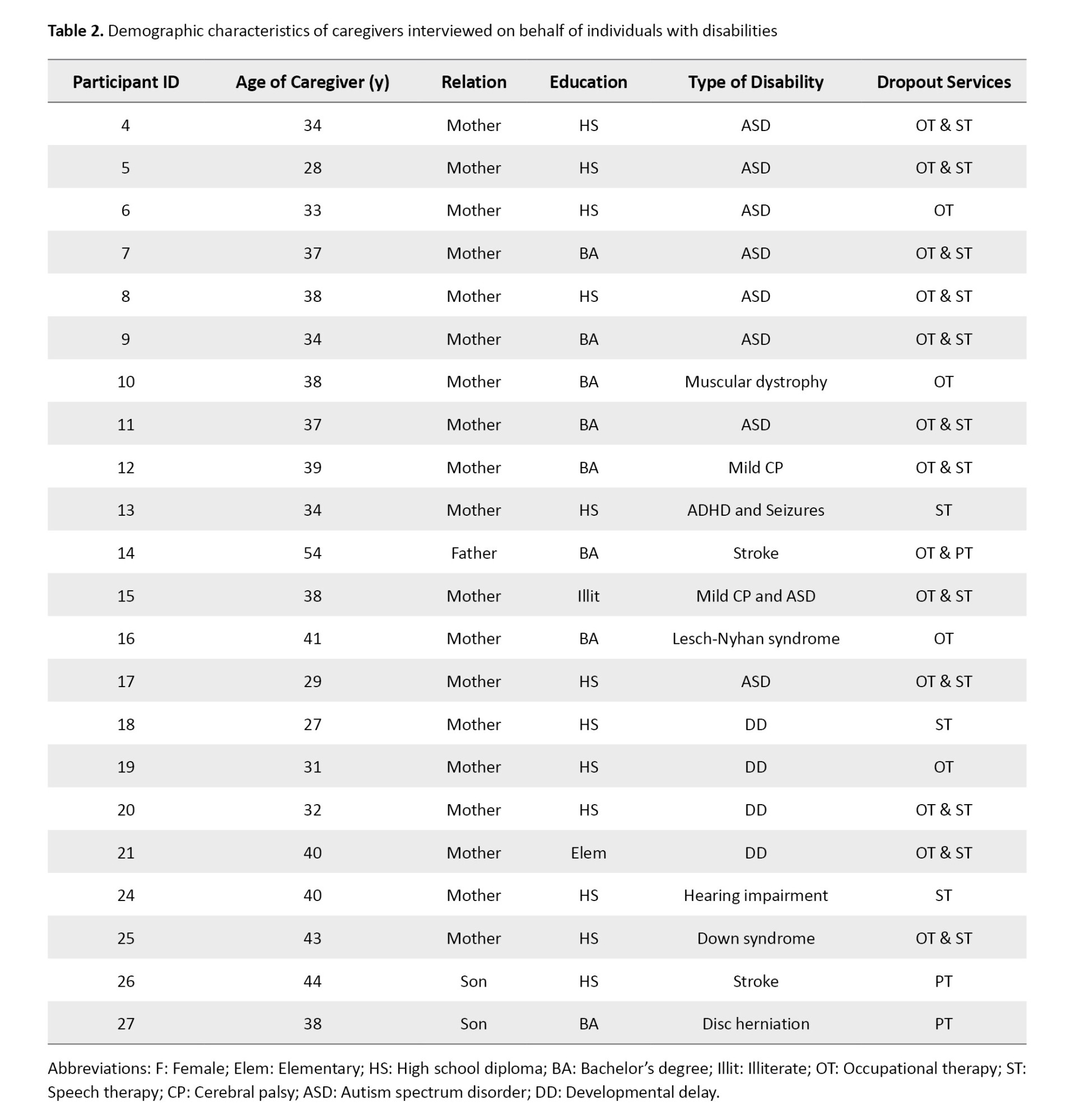
Participants included 28 individuals with various physical motor, developmental, or cognitive disabilities (or their caregivers, in cases where the individual was too young or had insufficient cognitive ability to respond independently), as well as 10 service providers in the fields of physiotherapy, speech therapy, and occupational therapy. The demographic characteristics of individuals with disabilities and caregivers are summarized in Tables 1 and 2.
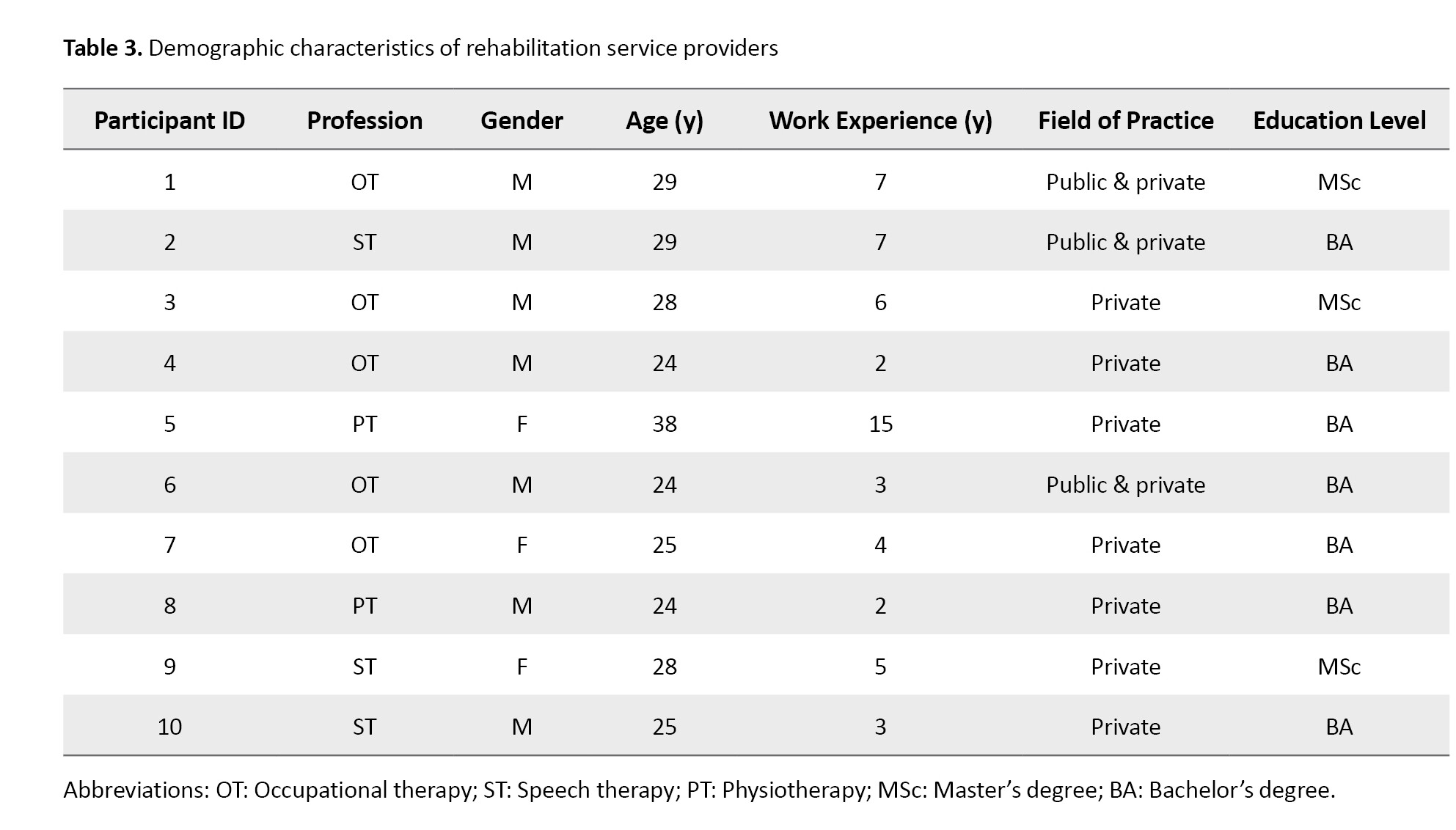
The characteristics of rehabilitation service providers are shown in Table 3.
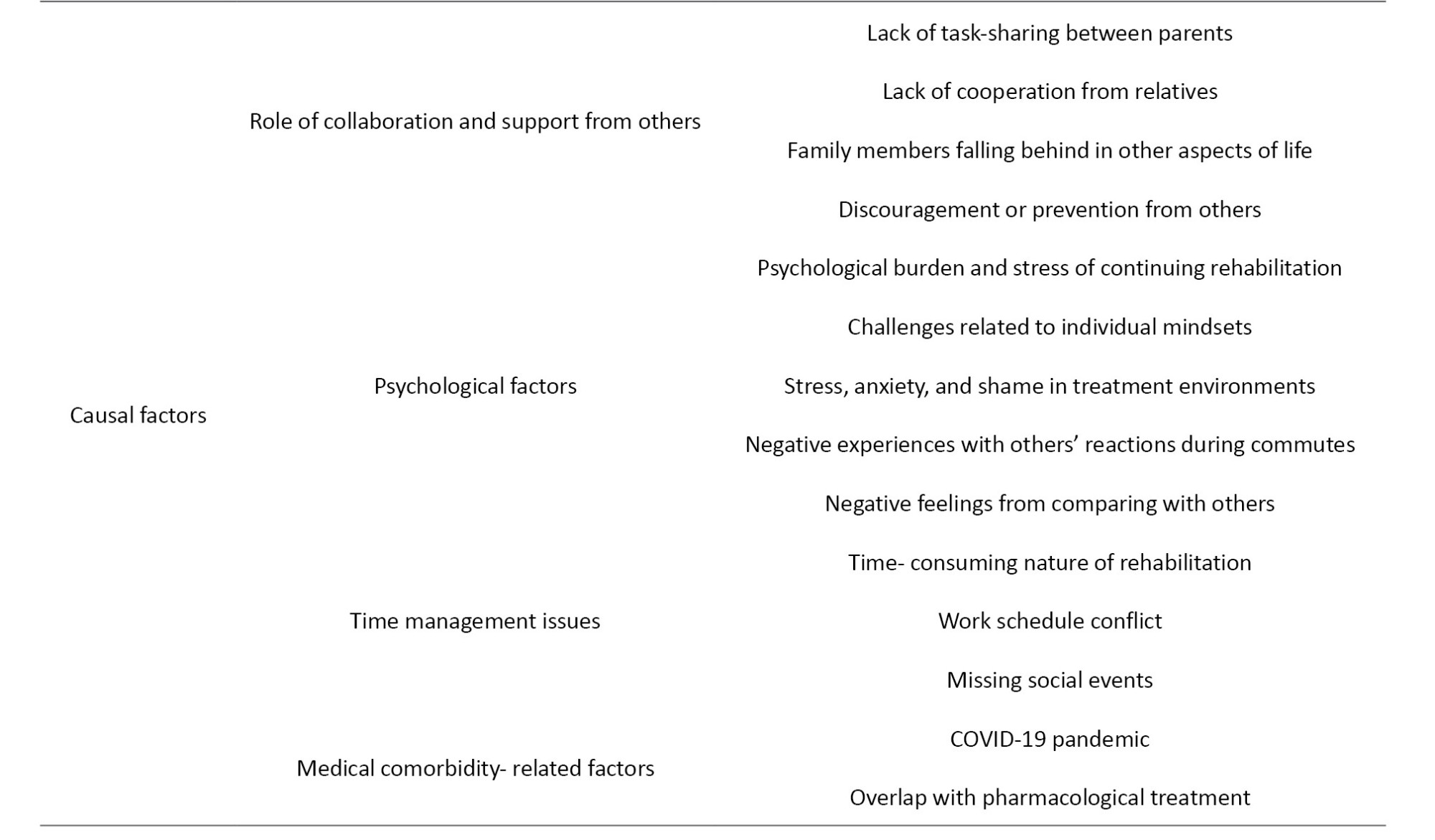
The interviewees shared their perspectives on the causal factors behind discontinuation of rehabilitation. Based on their views and experiences, 43 codes were extracted, which were organized into eight subthemes: “Expectations and attitudes toward rehabilitation,” “Accessibility issues,” “financial barriers,” “therapist and center related issues,” “role of collaboration and support from others,” “psychological factors,” “time management issues,” and “factors related to medical comorbidities.” from the integration of these subthemes, the overarching theme of “causal factors” emerged. The main theme, subthemes, and representative codes are summarized in Table 4, and each subtheme is described in detail in the following sections.
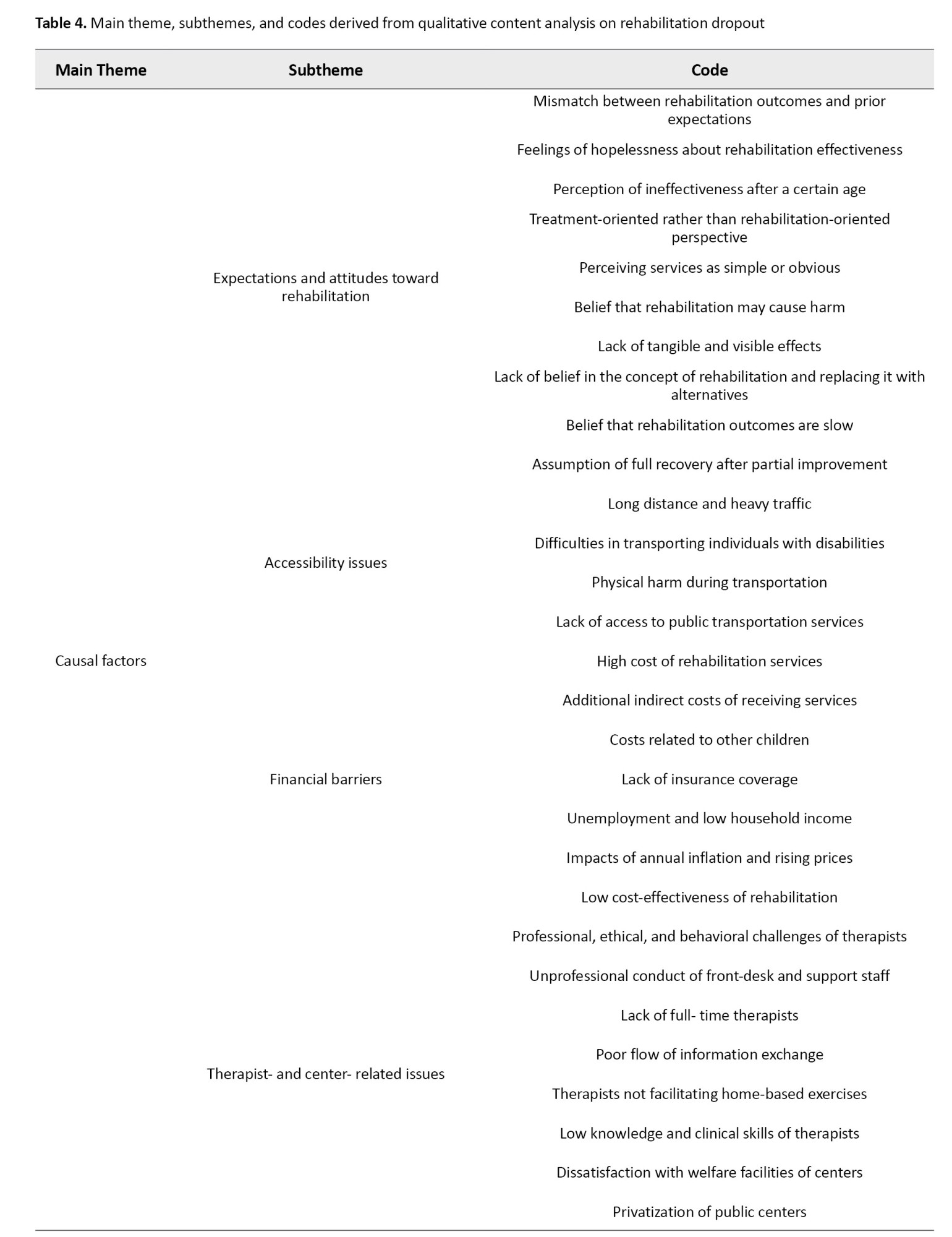
Expectations and attitudes toward rehabilitation
Clients’ expectations from rehabilitation services often did not align with reality, and this mismatch was one of the main reasons for discontinuation. Families usually expected a full recovery within a short period, whereas meaningful changes required time and continuity. For example, one parent stated:
“At first, I thought that after four months of occupational therapy, my child would be on track and progressing well. I assumed that after these four months, the process would end, and I would have a healthy child back” (Participant 7 [P.7]).
Hopelessness regarding effectiveness, the belief that rehabilitation becomes useless after a certain age, and perceiving rehabilitation as merely a form of medical treatment were among other deterrents. Some participants considered services to be simple and non-specialized, or even harmful. One participant noted:
“I reached a point where I felt rehabilitation no longer benefited me, and I was at the end of the road” (P.3).
Lack of observable progress, skepticism toward the concept of rehabilitation, a tendency to seek alternatives such as traditional medicine, and the belief that rehabilitation outcomes are slow or progress would be incomplete were all reported as significant reasons for dropping out.
Accessibility issues
This subtheme referred to geographical and physical limitations in accessing rehabilitation centers. Participants identified long distances, heavy traffic in metropolitan areas, and the lack of suitable public transportation as major barriers to continuity. One participant explained:
“One of the reasons for discontinuation was that in Tehran, the long distances and heavy traffic were really exhausting” (P.10).
In addition, difficulties in transporting individuals with disabilities, the absence of standard ramps and elevators, and behavioral challenges in social environments made attending sessions more difficult. In some cases, even caregivers experienced physical problems due to repeated transportation. One mother shared:
“On the other hand, as he grew older, we could no longer carry him back and forth… I myself developed arthritis and a herniated disc because of the constant lifting and moving” (P.16).
Financial Barriers
This subtheme referred to the economic pressures associated with receiving rehabilitation services. The identified codes included the high cost of sessions, additional transportation expenses, financial responsibilities for other children, lack of insurance coverage, unemployment or low family income, annual inflation, and the perception of low cost-effectiveness of rehabilitation.
Participants stated that the repetition of multiple sessions and high service fees restricted the continuation of therapy. One parent noted:
“At that time, when it was twice a week, the costs really put pressure on me. I stopped and decided not to take my child anymore” (P.20).
In addition to session fees, transportation costs were also a major obstacle:
“The center’s fees are not that high, maybe one or two million per month; but if I need to arrange transportation, it costs three or four million monthly, which is too much for me” (P.6).
The lack of insurance coverage for occupational and speech therapy, and the insufficient coverage for physiotherapy, further complicated service continuity:
“[The costs] are calculated as out-of-pocket expenses for me, and financial issues had a huge impact and caused a lot of stress” (P.23).
Economic challenges, such as unemployment and inflation exacerbated these financial burdens. One participant explained:
“The main reason for discontinuing rehabilitation was definitely the costs. The increasing rate of expenses made it impossible for us to continue” (P.3).
Finally, some families believed that the benefits of rehabilitation were not proportional to its costs:
“Overall, the family’s conclusion was that rehabilitation is not cost-effective” (therapists (T.4).
Therapist- and center-related issues
This subtheme referred to problems associated with the quality of services, therapists’ behaviors, and the conditions of rehabilitation centers. The main codes included communication difficulties with therapists, professional and ethical shortcomings, unprofessional conduct of front-desk and support staff, lack of full-time therapists, insufficient information exchange, failure to facilitate home-based exercises, low clinical competence, dissatisfaction with facilities, and the privatization of public centers.
Some participants highlighted weak communication between their child and the therapist:
“My son couldn’t connect with his doctors there; I knew that when he entered the therapy room, he wasn’t able to build any rapport” (P.21).
Unethical behavior by staff was also strongly emphasized:
“Unfortunately, many rehabilitation staff lack conscience. They just come for the money, and when they see a quiet, less able child, they don’t work properly with them to save their energy for other clients. I wish there were real accountability for such behavior” (P.11).
Similarly, inappropriate attitudes of center managers caused additional stress for families:
“…The managers of that center were so unethical and disrespectful to families that my husband only accompanied us to the entrance. He had to wait outside in the heat or cold because of their behavior and the way they supervised” (P.11).
Another major concern was the irregular presence of therapists in welfare-affiliated centers:
“This center didn’t have occupational and speech therapists every day, sometimes just once a week. They didn’t have also enough time to work properly with the children” (P.9).
Families also complained about the lack of clear information regarding therapy goals and required duration:
“Even the occupational therapist himself didn’t know how much my child needed services…” (P.13).
Another issue was the lack of practical and feasible home exercises:
“One of the exercises was sound recording, but because of stress I couldn’t do it. These exercises were exhausting and drained my energy, and eventually I had to stop” (P.28).
Some participants reported dissatisfaction with the low clinical skills of staff:
“I once went to centers under the Welfare Organization with lower fees, but I wasn’t satisfied at all. I felt like they were inexperienced people or students who had just studied superficially and gotten a certificate” (P.12).
Additional barriers included inadequate facilities, such as the absence of playrooms for siblings and the privatization of public centers, which increased costs and reduced service quality:
“I realized that the costs had gone up because the center became privatized, while the therapy hours decreased from three hours to less. It just wasn’t worth it” (P.9)
Role of collaboration and support from others
This subtheme highlighted the impact of family members, relatives, and others on whether rehabilitation was continued or abandoned. The main codes included lack of task-sharing between parents, absence of support from relatives and friends, disruption of other family members’ personal lives, and even obstruction of treatment by some individuals.
When the responsibility of follow-up fell solely on one parent, it often led to psychological exhaustion and treatment discontinuation:
“My husband was not supportive and didn’t back me up” (P.25).
The absence of support from extended family or friends further compounded the pressure. As one therapist emphasized:
“…Having a supportive figure such as a strong father, mother, sister, or brother, who can not only handle the problems but also solve issues is critical” (T.1).
In some cases, parents had to abandon work or education to follow up with treatment:
“I left my job because of the rehabilitation sessions, and I barely managed to finish my university studies with so much struggle” (P.4).
There were also reports of relatives actively discouraging therapy:
“Her husband completely disagreed with these programs. He kept saying, ‘Just leave it; these efforts are pointless’” (P.14).
Psychological factors
This subtheme referred to the psychological influences on individuals, both from prior personal predispositions and from the emotional impact of attending rehabilitation centers. Identified codes included psychological distress from rehabilitation follow-up, personal mindset challenges, stress, anxiety, and shame related to therapy attendance, negative encounters during commuting, and feelings of inadequacy when comparing with others.
One core concept was the psychological burden of rehabilitation itself. A participant shared:
“When I see other people, my mood is disturbed and I get anxious, and this makes me not want to be here” (P.18).
Another theme involved individual mindset-related barriers. Some participants attributed discontinuation to personal traits:
“More than anything, it was my personality, I just can’t do things consistently, so, I quit” (P.2).
“The reason I didn’t continue was my own messiness” (P.13).
Stress, anxiety, and shame associated with attending rehabilitation were also reported:
“At that time, I was worried the issue of urinary and fecal incontinence during sessions. After I quit rehab for five years, I finally felt relief from this concern” (P.3).
Negative experiences during commuting also emerged, particularly due to social stigma toward individuals with disabilities:
“Until he was 10, he was calm; I could take him by bus. But afterward, it was impossible to go by metro; he would hit me or mock others. We had several arguments with strangers who even tried to fight with him” (P.15).
Another significant factor was the emotional distress of comparing one’s child to others, both to peers with disabilities and to typically developing children:
“…My children are triplets, and only one of them has this condition. For me, disability means that he is not like the other two. This has been the worst thing in my life, overshadowing everything else” (P.12)
Time management issues
This subtheme referred to time-related constraints associated with attending rehabilitation sessions. The main codes included the time-consuming nature of the rehabilitation process, work schedule conflict, and deprivation from social activities.
The lengthy process of attending sessions consumed a considerable portion of daily life:
“Altogether, the classes take at least five hours a day” (P.8).
For employed individuals, the overlap between work schedules and rehabilitation center hours was a significant barrier:
“Since I am employed, this issue constantly conflicted with my job…” (P.13).
Moreover, the continuation of sessions often deprived participants of leisure activities and social events:
“A lot of time was wasted; considering the loss of personal life, work, etc.; it wasn’t worth it” (P.4).
Medical comorbidity-related factors
This subtheme emphasized the impact of co-occurring or successive medical conditions on the discontinuation of rehabilitation services. Two primary emerged codes were the COVID-19 pandemic and interference with pharmacological treatment.
During the COVID-19 pandemic, many families discontinued rehabilitation due to fear of infection:
“We couldn’t go for two years because of COVID. Out of fear of illness and infection, I didn’t take him. Even though some centers were open, I kept him home. I didn’t let him attend school either; he stayed at home completely” (P.17).
Additionally, chronic conditions, such as epilepsy and the burden of heavy medication regimens also disrupted rehabilitation:
“At one stage, they said speech and occupational therapy should be stopped because the medications he was taking were too strong” (P.8).
Discussion
This study aimed to explore the factors influencing the discontinuation of rehabilitation services from the perspectives of people with disabilities and service providers. The findings revealed that multiple factors contributed to non -adherence, which could be categorized into perceptual–attitudinal, economic, geographical, individual, social, and psychological dimensions. Unrealistic expectations and patients’ disappointment were among the most significant barriers, as the gap between patients’ perceptions of the rehabilitation process and its actual realities increased the likelihood of treatment withdrawal, as Sloots et al. and Windle et al. emphasized [14, 15]. Furthermore, disbelief in rehabilitation and a tendency toward alternative treatments, such as traditional medicine were also noted in the present study, consistent with the findings of Oshomoji et al. [16].
Economic barriers, including high service costs, lack of insurance coverage, and the impact of inflation, were identified as key reasons for discontinuation. These results are in line with the findings of Bamer et al. [17], Pishkhani et al. [18], and Aliabadi et al. [19]. Geographical challenges, such as long distances and transportation difficulties for people with disabilities, also played an important role in discontinuation, a finding that was also confirmed in studies by Borg et al. and Aliabadi et al. [19, 20].
The quality of services and effective therapist–patient communication emerged as other critical factors, where dissatisfaction with staff interactions or weaknesses in the rehabilitation team contributed to non-adherence. This finding was consistent with the results of Pishkhani et al. [18] and Razjouyan et al. [21]. Similarly, family and social support were shown to be vital in ensuring the continuity of care, aligning with the findings of Ezzati and Grover et al. regarding the importance of emotional–psychological support [22, 23].
From a psychological perspective, mental distress, stress, and negative attitudes of others were among the major factors leading to treatment discontinuation. Ezzati identified stress as a key reason [22], while Resurrección et al. emphasized the role of intrapersonal factors, such as health beliefs [10]. However, Pedersen et al. found that high anxiety could, in some cases, increase participation [24]. Additionally, time constraints and conflicts with work or family responsibilities were other barriers, consistent with the studies by Hosseini et al. [25], Gibson et al. [26], and Worcester et al. [27]. Finally, comorbid conditions, such as COVID-19 or the need for intensive pharmacological treatment also led to discontinuation, in line with the findings of Borg et al. regarding cardiac patients [20] and Ezzati concerning obesity [22].
Taken together, these findings indicate that the discontinuation of rehabilitation results from the complex interplay of individual, social, economic, and structural factors. Therefore, policy-level and practice-level interventions should comprehensively address these dimensions.
Based on these findings, it can be concluded that designing effective interventions to increase treatment adherence requires a holistic and integrated approach. Such interventions should operate at the macro-policy level (e.g. expanding insurance coverage, decentralizing and localizing services), as well as at the operational level (e.g. better patient education, empowering therapists, modifying public attitudes, and strengthening family and social support). Addressing each of these dimensions can serve as an effective step toward improving the quality of life of people with disabilities and enhancing the overall efficiency of rehabilitation services. While the results are not intended for statistical generalization, they offer transferable insights that may be applicable to similar social and rehabilitation contexts.
Conclusion
The findings of this qualitative study clearly demonstrated that dropout of rehabilitation programs among people with disabilities is a complex and multidimensional phenomenon rooted in diverse and intertwined factors. These include unrealistic attitudes and expectations toward rehabilitation, financial difficulties, physical and geographical access barriers, shortcomings in service delivery models and professional interactions, individual psychological issues, time- and family-related challenges, and the lack of social and interpersonal support. This interconnection highlights that treatment discontinuation is not the result of a single factor but rather the outcome of the interaction of multiple factors across individual, interpersonal, social, and structural levels.
Limitations
This study was conducted qualitatively in Tehran, which may restrict the generalizability of the findings to other regions or cultural contexts. Therefore, the findings reflect the specific social and cultural context of the participants. Moreover, as data were based on participants’ self-reported experiences, some degree of recall bias may exist.
Suggestions
Future research could expand on these findings by including participants from different regions and rehabilitation contexts to explore similarities and differences across settings. Mixed-method or longitudinal approaches may help deepen understanding and identify potential causal relationships. Moreover, including perspectives from policymakers, insurance providers, and rehabilitation administrators could enrich the systemic view and support evidence-informed policy development.
Declaration
The authors declare that there were no financial, personal, or academic conflicts of interest during the design, implementation, data analysis, or writing of this study. The research was conducted independently and responsibly, in full compliance with relevant ethical principles.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1403.746).
Funding
The paper was extracted from the master's thesis of Mohammad Najafpour, approved by the Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Authors' contributions
Conceptualization: Mohammad Najafpour and Samaneh Heidari; Methodology: Mohammad Najafpour and Reza Salehi; Investigation: All authors; Writing the original draft: Mohammad Najafpour; Review and editing: Samaneh Heidari, Reza Salehi; Supervision: Samaneh Heidari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
This study would not have been possible without the support, collaboration, and kind assistance of many individuals and institutions, particularly the Yara Comprehensive Rehabilitation Center. The authors extend their sincere gratitude to all participants in this research, including people with disabilities, their families, and rehabilitation service providers, who generously shared their valuable experiences with the research team.
References
Rehabilitation, as an essential component of the health system and a fundamental human right, plays a key role in improving the quality of life for individuals with disabilities. The World Health Organization (WHO) identifies disability not only as a health issue but also as a development priority and part of human rights [1]. The global initiative “rehabilitation 2030” also emphasizes raising awareness, expanding access to rehabilitation services, and reducing costs [2]. With the increasing prevalence of disability, particularly in developing countries, equitable access to rehabilitation services has become more critical than ever [3].
In general, the treatment and rehabilitation of any disease or disability involve several main stages. These include raising awareness about the disease process and related risk factors, screening for the disease, associated risks or comorbidities, diagnosis, treatment, adherence to prescribed treatment, and control or improvement [4]. In this regard, adherence and continuation of treatment are crucial for achieving effective outcomes. Studies have shown that regular and uninterrupted participation in rehabilitation sessions is one of the most important factors in improving the condition of individuals with various disabilities [5, 6]. Furthermore, consistent participation in rehabilitation contributes to greater independence, reduced dependency, and has a cost-effective impact from an economic perspective [5, 6]. Timely interventions significantly increase their effectiveness [7]. In addition to direct and obvious costs, discontinuing treatment is also a risk factor for a range of adverse and secondary health outcomes [8, 9].
Despite the clear need for persistence and adherence in rehabilitation, some individuals with disabilities [10], or parents and caregivers of children with disabilities, may express dissatisfaction with rehabilitation for various reasons and in some cases withdraw their children from ongoing rehabilitation programs [11]. This issue becomes particularly problematic when early intervention is required, for instance, in children with developmental delays or similar conditions, where the window of opportunity for intervention is limited.
Health plays a crucial role in development, and for individuals with disabilities, achieving the highest possible level of health and quality of life depends on adherence to rehabilitation programs. Regular attendance at rehabilitation sessions enhances treatment effectiveness, reduces economic costs, and improves individual functioning. This is especially important for children and individuals with cognitive disabilities. Given the lack of comprehensive studies on the reasons behind dropout of rehabilitation treatments, the present study aimed to examine the factors influencing this issue from the perspective of individuals with disabilities and rehabilitation service providers.
Materials and Methods
This qualitative study, conducted using conventional content analysis with an inductive approach, explored the experiences and perspectives of individuals with disabilities and rehabilitation service providers regarding the reasons for discontinuation of treatment programs in Tehran.
Participants were selected purposefully, with maximum variation in variables, such as type of disability, age, gender, and level of education, to gather a comprehensive range of views and experiences. Inclusion criteria for individuals with disabilities were having attended at least three rehabilitation sessions, discontinuation of services for a period of three months or more after starting rehabilitation, and willingness to participate in interviews. For service providers, inclusion criteria were possession of a valid medical license in one of the three mentioned fields and at least two years of professional experience. Ineffective cooperation during interviews or voluntary withdrawal were considered exclusion criteria.
Data were collected through in-depth, semi-structured interviews. The interview guide consisted of open-ended, exploratory questions focusing on barriers to continuing rehabilitation services (for example, “What made you stop attending rehabilitation sessions? Please explain.”). The duration of the interviews ranged from 10 to 48 minutes. Prior to participation, written informed consent was obtained from all participants. The time and location of the sessions were mutually agreed upon and conducted in a quiet, calm environment. Participants were free to withdraw from the study at any stage and could contact the interviewer for clarification of any questions. Audio files were securely stored in protected folders with password access. The sampling process lasted for approximately 6 months.
All interviews were audio-recorded and transcribed verbatim. They were then analyzed using conventional content analysis based on the method of Graneheim and Lundman [12]. Initial coding, categorization, and theme extraction were carried out by Mohammad Najafpour. The process included repeated reading of the transcripts to gain an overall understanding, identifying meaning units, condensing and abstracting them, and assigning codes. Subsequently, the codes were compared for similarities and differences, grouped into subcategories, and finally organized into broader categories.
To ensure trustworthiness of the data, Lincoln and Guba’s four criteria were applied: Transferability (through the selection of diverse participants), dependability (rechecking the codes with other researchers), confirmability (review of the results by several research team members), and credibility (through field notes and in-depth analysis of interview transcripts) [13].
Results
Participants included 28 individuals with various physical motor, developmental, or cognitive disabilities (or their caregivers, in cases where the individual was too young or had insufficient cognitive ability to respond independently), as well as 10 service providers in the fields of physiotherapy, speech therapy, and occupational therapy. The demographic characteristics of individuals with disabilities and caregivers are summarized in Tables 1 and 2.
The characteristics of rehabilitation service providers are shown in Table 3.
The interviewees shared their perspectives on the causal factors behind discontinuation of rehabilitation. Based on their views and experiences, 43 codes were extracted, which were organized into eight subthemes: “Expectations and attitudes toward rehabilitation,” “Accessibility issues,” “financial barriers,” “therapist and center related issues,” “role of collaboration and support from others,” “psychological factors,” “time management issues,” and “factors related to medical comorbidities.” from the integration of these subthemes, the overarching theme of “causal factors” emerged. The main theme, subthemes, and representative codes are summarized in Table 4, and each subtheme is described in detail in the following sections.
Expectations and attitudes toward rehabilitation
Clients’ expectations from rehabilitation services often did not align with reality, and this mismatch was one of the main reasons for discontinuation. Families usually expected a full recovery within a short period, whereas meaningful changes required time and continuity. For example, one parent stated:
“At first, I thought that after four months of occupational therapy, my child would be on track and progressing well. I assumed that after these four months, the process would end, and I would have a healthy child back” (Participant 7 [P.7]).
Hopelessness regarding effectiveness, the belief that rehabilitation becomes useless after a certain age, and perceiving rehabilitation as merely a form of medical treatment were among other deterrents. Some participants considered services to be simple and non-specialized, or even harmful. One participant noted:
“I reached a point where I felt rehabilitation no longer benefited me, and I was at the end of the road” (P.3).
Lack of observable progress, skepticism toward the concept of rehabilitation, a tendency to seek alternatives such as traditional medicine, and the belief that rehabilitation outcomes are slow or progress would be incomplete were all reported as significant reasons for dropping out.
Accessibility issues
This subtheme referred to geographical and physical limitations in accessing rehabilitation centers. Participants identified long distances, heavy traffic in metropolitan areas, and the lack of suitable public transportation as major barriers to continuity. One participant explained:
“One of the reasons for discontinuation was that in Tehran, the long distances and heavy traffic were really exhausting” (P.10).
In addition, difficulties in transporting individuals with disabilities, the absence of standard ramps and elevators, and behavioral challenges in social environments made attending sessions more difficult. In some cases, even caregivers experienced physical problems due to repeated transportation. One mother shared:
“On the other hand, as he grew older, we could no longer carry him back and forth… I myself developed arthritis and a herniated disc because of the constant lifting and moving” (P.16).
Financial Barriers
This subtheme referred to the economic pressures associated with receiving rehabilitation services. The identified codes included the high cost of sessions, additional transportation expenses, financial responsibilities for other children, lack of insurance coverage, unemployment or low family income, annual inflation, and the perception of low cost-effectiveness of rehabilitation.
Participants stated that the repetition of multiple sessions and high service fees restricted the continuation of therapy. One parent noted:
“At that time, when it was twice a week, the costs really put pressure on me. I stopped and decided not to take my child anymore” (P.20).
In addition to session fees, transportation costs were also a major obstacle:
“The center’s fees are not that high, maybe one or two million per month; but if I need to arrange transportation, it costs three or four million monthly, which is too much for me” (P.6).
The lack of insurance coverage for occupational and speech therapy, and the insufficient coverage for physiotherapy, further complicated service continuity:
“[The costs] are calculated as out-of-pocket expenses for me, and financial issues had a huge impact and caused a lot of stress” (P.23).
Economic challenges, such as unemployment and inflation exacerbated these financial burdens. One participant explained:
“The main reason for discontinuing rehabilitation was definitely the costs. The increasing rate of expenses made it impossible for us to continue” (P.3).
Finally, some families believed that the benefits of rehabilitation were not proportional to its costs:
“Overall, the family’s conclusion was that rehabilitation is not cost-effective” (therapists (T.4).
Therapist- and center-related issues
This subtheme referred to problems associated with the quality of services, therapists’ behaviors, and the conditions of rehabilitation centers. The main codes included communication difficulties with therapists, professional and ethical shortcomings, unprofessional conduct of front-desk and support staff, lack of full-time therapists, insufficient information exchange, failure to facilitate home-based exercises, low clinical competence, dissatisfaction with facilities, and the privatization of public centers.
Some participants highlighted weak communication between their child and the therapist:
“My son couldn’t connect with his doctors there; I knew that when he entered the therapy room, he wasn’t able to build any rapport” (P.21).
Unethical behavior by staff was also strongly emphasized:
“Unfortunately, many rehabilitation staff lack conscience. They just come for the money, and when they see a quiet, less able child, they don’t work properly with them to save their energy for other clients. I wish there were real accountability for such behavior” (P.11).
Similarly, inappropriate attitudes of center managers caused additional stress for families:
“…The managers of that center were so unethical and disrespectful to families that my husband only accompanied us to the entrance. He had to wait outside in the heat or cold because of their behavior and the way they supervised” (P.11).
Another major concern was the irregular presence of therapists in welfare-affiliated centers:
“This center didn’t have occupational and speech therapists every day, sometimes just once a week. They didn’t have also enough time to work properly with the children” (P.9).
Families also complained about the lack of clear information regarding therapy goals and required duration:
“Even the occupational therapist himself didn’t know how much my child needed services…” (P.13).
Another issue was the lack of practical and feasible home exercises:
“One of the exercises was sound recording, but because of stress I couldn’t do it. These exercises were exhausting and drained my energy, and eventually I had to stop” (P.28).
Some participants reported dissatisfaction with the low clinical skills of staff:
“I once went to centers under the Welfare Organization with lower fees, but I wasn’t satisfied at all. I felt like they were inexperienced people or students who had just studied superficially and gotten a certificate” (P.12).
Additional barriers included inadequate facilities, such as the absence of playrooms for siblings and the privatization of public centers, which increased costs and reduced service quality:
“I realized that the costs had gone up because the center became privatized, while the therapy hours decreased from three hours to less. It just wasn’t worth it” (P.9)
Role of collaboration and support from others
This subtheme highlighted the impact of family members, relatives, and others on whether rehabilitation was continued or abandoned. The main codes included lack of task-sharing between parents, absence of support from relatives and friends, disruption of other family members’ personal lives, and even obstruction of treatment by some individuals.
When the responsibility of follow-up fell solely on one parent, it often led to psychological exhaustion and treatment discontinuation:
“My husband was not supportive and didn’t back me up” (P.25).
The absence of support from extended family or friends further compounded the pressure. As one therapist emphasized:
“…Having a supportive figure such as a strong father, mother, sister, or brother, who can not only handle the problems but also solve issues is critical” (T.1).
In some cases, parents had to abandon work or education to follow up with treatment:
“I left my job because of the rehabilitation sessions, and I barely managed to finish my university studies with so much struggle” (P.4).
There were also reports of relatives actively discouraging therapy:
“Her husband completely disagreed with these programs. He kept saying, ‘Just leave it; these efforts are pointless’” (P.14).
Psychological factors
This subtheme referred to the psychological influences on individuals, both from prior personal predispositions and from the emotional impact of attending rehabilitation centers. Identified codes included psychological distress from rehabilitation follow-up, personal mindset challenges, stress, anxiety, and shame related to therapy attendance, negative encounters during commuting, and feelings of inadequacy when comparing with others.
One core concept was the psychological burden of rehabilitation itself. A participant shared:
“When I see other people, my mood is disturbed and I get anxious, and this makes me not want to be here” (P.18).
Another theme involved individual mindset-related barriers. Some participants attributed discontinuation to personal traits:
“More than anything, it was my personality, I just can’t do things consistently, so, I quit” (P.2).
“The reason I didn’t continue was my own messiness” (P.13).
Stress, anxiety, and shame associated with attending rehabilitation were also reported:
“At that time, I was worried the issue of urinary and fecal incontinence during sessions. After I quit rehab for five years, I finally felt relief from this concern” (P.3).
Negative experiences during commuting also emerged, particularly due to social stigma toward individuals with disabilities:
“Until he was 10, he was calm; I could take him by bus. But afterward, it was impossible to go by metro; he would hit me or mock others. We had several arguments with strangers who even tried to fight with him” (P.15).
Another significant factor was the emotional distress of comparing one’s child to others, both to peers with disabilities and to typically developing children:
“…My children are triplets, and only one of them has this condition. For me, disability means that he is not like the other two. This has been the worst thing in my life, overshadowing everything else” (P.12)
Time management issues
This subtheme referred to time-related constraints associated with attending rehabilitation sessions. The main codes included the time-consuming nature of the rehabilitation process, work schedule conflict, and deprivation from social activities.
The lengthy process of attending sessions consumed a considerable portion of daily life:
“Altogether, the classes take at least five hours a day” (P.8).
For employed individuals, the overlap between work schedules and rehabilitation center hours was a significant barrier:
“Since I am employed, this issue constantly conflicted with my job…” (P.13).
Moreover, the continuation of sessions often deprived participants of leisure activities and social events:
“A lot of time was wasted; considering the loss of personal life, work, etc.; it wasn’t worth it” (P.4).
Medical comorbidity-related factors
This subtheme emphasized the impact of co-occurring or successive medical conditions on the discontinuation of rehabilitation services. Two primary emerged codes were the COVID-19 pandemic and interference with pharmacological treatment.
During the COVID-19 pandemic, many families discontinued rehabilitation due to fear of infection:
“We couldn’t go for two years because of COVID. Out of fear of illness and infection, I didn’t take him. Even though some centers were open, I kept him home. I didn’t let him attend school either; he stayed at home completely” (P.17).
Additionally, chronic conditions, such as epilepsy and the burden of heavy medication regimens also disrupted rehabilitation:
“At one stage, they said speech and occupational therapy should be stopped because the medications he was taking were too strong” (P.8).
Discussion
This study aimed to explore the factors influencing the discontinuation of rehabilitation services from the perspectives of people with disabilities and service providers. The findings revealed that multiple factors contributed to non -adherence, which could be categorized into perceptual–attitudinal, economic, geographical, individual, social, and psychological dimensions. Unrealistic expectations and patients’ disappointment were among the most significant barriers, as the gap between patients’ perceptions of the rehabilitation process and its actual realities increased the likelihood of treatment withdrawal, as Sloots et al. and Windle et al. emphasized [14, 15]. Furthermore, disbelief in rehabilitation and a tendency toward alternative treatments, such as traditional medicine were also noted in the present study, consistent with the findings of Oshomoji et al. [16].
Economic barriers, including high service costs, lack of insurance coverage, and the impact of inflation, were identified as key reasons for discontinuation. These results are in line with the findings of Bamer et al. [17], Pishkhani et al. [18], and Aliabadi et al. [19]. Geographical challenges, such as long distances and transportation difficulties for people with disabilities, also played an important role in discontinuation, a finding that was also confirmed in studies by Borg et al. and Aliabadi et al. [19, 20].
The quality of services and effective therapist–patient communication emerged as other critical factors, where dissatisfaction with staff interactions or weaknesses in the rehabilitation team contributed to non-adherence. This finding was consistent with the results of Pishkhani et al. [18] and Razjouyan et al. [21]. Similarly, family and social support were shown to be vital in ensuring the continuity of care, aligning with the findings of Ezzati and Grover et al. regarding the importance of emotional–psychological support [22, 23].
From a psychological perspective, mental distress, stress, and negative attitudes of others were among the major factors leading to treatment discontinuation. Ezzati identified stress as a key reason [22], while Resurrección et al. emphasized the role of intrapersonal factors, such as health beliefs [10]. However, Pedersen et al. found that high anxiety could, in some cases, increase participation [24]. Additionally, time constraints and conflicts with work or family responsibilities were other barriers, consistent with the studies by Hosseini et al. [25], Gibson et al. [26], and Worcester et al. [27]. Finally, comorbid conditions, such as COVID-19 or the need for intensive pharmacological treatment also led to discontinuation, in line with the findings of Borg et al. regarding cardiac patients [20] and Ezzati concerning obesity [22].
Taken together, these findings indicate that the discontinuation of rehabilitation results from the complex interplay of individual, social, economic, and structural factors. Therefore, policy-level and practice-level interventions should comprehensively address these dimensions.
Based on these findings, it can be concluded that designing effective interventions to increase treatment adherence requires a holistic and integrated approach. Such interventions should operate at the macro-policy level (e.g. expanding insurance coverage, decentralizing and localizing services), as well as at the operational level (e.g. better patient education, empowering therapists, modifying public attitudes, and strengthening family and social support). Addressing each of these dimensions can serve as an effective step toward improving the quality of life of people with disabilities and enhancing the overall efficiency of rehabilitation services. While the results are not intended for statistical generalization, they offer transferable insights that may be applicable to similar social and rehabilitation contexts.
Conclusion
The findings of this qualitative study clearly demonstrated that dropout of rehabilitation programs among people with disabilities is a complex and multidimensional phenomenon rooted in diverse and intertwined factors. These include unrealistic attitudes and expectations toward rehabilitation, financial difficulties, physical and geographical access barriers, shortcomings in service delivery models and professional interactions, individual psychological issues, time- and family-related challenges, and the lack of social and interpersonal support. This interconnection highlights that treatment discontinuation is not the result of a single factor but rather the outcome of the interaction of multiple factors across individual, interpersonal, social, and structural levels.
Limitations
This study was conducted qualitatively in Tehran, which may restrict the generalizability of the findings to other regions or cultural contexts. Therefore, the findings reflect the specific social and cultural context of the participants. Moreover, as data were based on participants’ self-reported experiences, some degree of recall bias may exist.
Suggestions
Future research could expand on these findings by including participants from different regions and rehabilitation contexts to explore similarities and differences across settings. Mixed-method or longitudinal approaches may help deepen understanding and identify potential causal relationships. Moreover, including perspectives from policymakers, insurance providers, and rehabilitation administrators could enrich the systemic view and support evidence-informed policy development.
Declaration
The authors declare that there were no financial, personal, or academic conflicts of interest during the design, implementation, data analysis, or writing of this study. The research was conducted independently and responsibly, in full compliance with relevant ethical principles.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (Code: IR.IUMS.REC.1403.746).
Funding
The paper was extracted from the master's thesis of Mohammad Najafpour, approved by the Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Authors' contributions
Conceptualization: Mohammad Najafpour and Samaneh Heidari; Methodology: Mohammad Najafpour and Reza Salehi; Investigation: All authors; Writing the original draft: Mohammad Najafpour; Review and editing: Samaneh Heidari, Reza Salehi; Supervision: Samaneh Heidari.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
This study would not have been possible without the support, collaboration, and kind assistance of many individuals and institutions, particularly the Yara Comprehensive Rehabilitation Center. The authors extend their sincere gratitude to all participants in this research, including people with disabilities, their families, and rehabilitation service providers, who generously shared their valuable experiences with the research team.
References
- World Health Organization (WHO). WHO global disability action plan 2014-2021: Better health for all people with disability. Geneva: World Health Organization; 2015. [Link]
- Gimigliano F, Negrini S. The World Health Organization "rehabilitation 2030: A call for action". Eur J Phys Rehabil Med. 2017; 53(2):155-68. [DOI:10.23736/S1973-9087.17.04746-3] [PMID]
- World Health Organization (WHO). World report on disability. World report on disability. 2011 [Updated 2026 February 18]. Available from: [Link]
- Devi R, Kanitkar K, Narendhar R, Sehmi K, Subramaniam K. A narrative review of the patient journey through the lens of non-communicable diseases in low-and middle-income countries. Adv Ther. 2020; 37(12):4808-30. [DOI:10.1007/s12325-020-01519-3] [PMID]
- House CM, Anstadt MA, Stuck LH, Nelson WB. The association between cardiac rehabilitation attendance and hospital readmission. Am J Lifestyle Med. 2018; 12(6):513-20. [DOI:10.1177/1559827616670118] [PMID]
- Nelson MB, Gilbert ON, Duncan PW, Kitzman DW, Reeves GR, Whellan DJ, et al. Intervention adherence in REHAB‐HF: predictors and relationship with physical function, quality of life, and clinical events. J Am Heart Assoc. 2022;11(11):e024246. [DOI:10.1161/JAHA.121.024246] [PMID]
- Lobo MA, Harbourne RT, Dusing SC, McCoy SW. Grounding early intervention: Physical therapy cannot just be about motor skills anymore. Phys Ther. 2013; 93(1):94-103. [DOI:10.2522/ptj.20120158] [PMID]
- Kane S, Huo D, Aikens J, Hanauer S. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis. Am J Medicine. 2003; 114(1):39-43. [DOI:10.1016/S0002-9343(02)01383-9] [PMID]
- Burman WJ, Cohn DL, Rietmeijer CA, Judson FN, Reves RR, Sbarbaro JA. Noncompliance with directly observed therapy for tuberculosis: epidemiology and effect on the outcome of treatment. Chest. 1997; 111(5):1168-73. [DOI:10.1378/chest.111.5.1168] [PMID]
- Resurrección DM, Moreno-Peral P, Gomez-Herranz M, Rubio-Valera M, Pastor L, Caldas de Almeida JM, et al. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: A systematic review of prospective cohort studies. Eur J Cardiovasc Nurs. 2019; 18(1):38-47. [DOI:10.1177/1474515118783157] [PMID]
- Valentine K. A consideration of medicalisation: Choice, engagement and other responsibilities of parents of children with autism spectrum disorder. Soc Sci Med. 2010;71(5):950-7. [DOI:10.1016/j.socscimed.2010.06.010] [PMID]
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004; 24(2):105-12. [DOI:10.1016/j.nedt.2003.10.001] [PMID]
- Lincoln YS, Guba EG. Naturalistic inquiry. Los Angeles: Sage; 1985. [DOI:10.1016/0147-1767(85)90062-8]
- Sloots M, Dekker JH, Bartels E, Pont M, Geertzen JH, Dekker J. Reasons for drop-out from rehabilitation in patients of Turkish and Moroccan origin with chronic low back pain in The Netherlands: A qualitative study. J Rehabil Med. 2010; 42(6):566-73. [DOI:10.2340/16501977-0536] [PMID]
- Windle E, Tee H, Sabitova A, Jovanovic N, Priebe S, Carr C. Association of patient treatment preference with dropout and clinical outcomes in adult psychosocial mental health interventions: A systematic review and meta-analysis. JAMA Psychiatry. 2020; 77(3):294-302. [DOI:10.1001/jamapsychiatry.2019.3750] [PMID]
- Oshomoji OI, Ajiroba JO, Semudara SO, Olayemi MA, Adeoye SO, Ugwu OC, et al. Cultural influences on physiotherapy engagement and outcomes in Guillain-Barré syndrome rehabilitation: A systematic review. Discov Public Health. 2025; 22(1):302. [DOI:10.1186/s12982-025-00682-8]
- Bamer AM, McMullen K, Gibran N, Holavanahalli R, Schneider JC, Carrougher GJ, et al. Factors associated with attrition of adult participants in a longitudinal database: A national institute on disability, independent living, and rehabilitation research burn model system study. J Burn Care Res. 2020; 41(2):270-9. [DOI:10.1093/jbcr/irz186] [PMID]
- Pishkhani MK, Dalvandi A, Ebadi A, Hosseini M. Factors affecting adherence to rehabilitation in Iranian stroke patients: A qualitative study. J Vasc Nurs. 2019; 37(4):264-71. [DOI:10.1016/j.jvn.2019.07.001] [PMID]
- Aliabadi S, Hatamizadeh N, Vamghi R, Kazemnejad A. [Children with disability: barriers to regular attendance in rehabilitation sessions (Persian)]. J Res Rehabil Sci. 2013; 8(5):959-69. [DOI:10.22122/jrrs.v8i5.474]
- Borg S, Öberg B, Leosdottir M, Lindolm D, Nilsson L, Bäck M. Factors associated with non-attendance at exercise-based cardiac rehabilitation. BMC Sports Sci Med Rehabil. 2019; 11:13. [DOI:10.1186/s13102-019-0135-7] [PMID]
- Razjouyan K, Yasamy MT, Rezaei A, Davari-Ashtiani R, Khademi M, Sohrabi MR. Dropout from rehabilitation and its associated factors in children with developmental disabilities in Tehran Rehabilitation centers. Iran J Psychiatry Behav Sci. 2021; 15:e113655. [DOI:10.5812/ijpbs.113655]
- Ezzati P. [Investigating the role of life with stressful events and demographic and clinical factors in the follow-up of cardiac rehabilitation after retraction coronary artery surgery in patients referred to the rehabilitation department of Imam Ali Hospital (AS) in Kermanshah city in 2014 (Persian)] [MSc. Thesis]. Tehran: University of Welfare and Rehabilitation Sciences; 2016. [Link]
- Grover S, Dua D, Chakrabarti S, Avasthi A. Dropout rates and factors associated with dropout from treatment among elderly patients attending the outpatient services of a tertiary care hospital. Ind J Psychiatry. 2018; 60(1):49-55. [DOI:10.4103/0019-5545.174373] [PMID]
- Pedersen M, Egerod I, Overgaard D, Baastrup M, Andersen I. Social inequality in phase II cardiac rehabilitation attendance: The impact of potential mediators. Eur Cardiovasc Nurs. 2018; 17(4):345-55. [DOI:10.1177/1474515117746011] [PMID]
- Hosseini Z, Ghaffari M, Rakhshanderou S, Jafari Y, Shoraka HR. Investigating the reasons for not referring men to health centers to receive health services. J North Khorasan Univ Med Sci. 2022; 14(1):29-37. [DOI:10.52547/nkums.14.1.29]
- Gibson I, Carvalho M, Byrne M, Dunne D, Kenny E, Mcsharry J, et al. What am I doing here? Enablers and barriers to community-based cardiac rehabilitation attendance: A qualitative study utilising a behavioural science approach. Eur J Cardiovasc Nurs. 2021; 20(Supplement_1):zvab060. [DOI:10.1093/eurjcn/zvab060.065]
- Worcester MU, Murphy BM, Mee VK, Roberts SB, Goble AJ. Cardiac rehabilitation programmes: Predictors of non-attendance and drop-out. Eur J Prevent Cardiol. 2004;11(4):328-35. [DOI:10.1097/01.hjr.0000137083.20844.54] [PMID]
Type of Study: Research |
Subject:
Rehabilitation management
Received: 2025/09/2 | Accepted: 2025/12/17 | Published: 2026/03/11
Received: 2025/09/2 | Accepted: 2025/12/17 | Published: 2026/03/11
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.