

Volume 9, Issue 1 (Continuously Updated- In press 2026)
Func Disabil J 2026, 9(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jarollahi F, Hosseini A, Ghaharri S, Jalaie S, Validabadi Z, DesJardin J L, et al . Psychometric Evaluation of the Persian Version of the Scale of Parental Involvement and Self-efficacy-revised. Func Disabil J 2026; 9 (1)
URL: http://fdj.iums.ac.ir/article-1-329-en.html
URL: http://fdj.iums.ac.ir/article-1-329-en.html
Farnoush Jarollahi1 

 , Anis Hosseini1 , Shahrbanoo Ghaharri2 , Shohreh Jalaie *3 , Zahra Validabadi2 , Jean L. DesJardin4 , Samin Moradi1 , Sahand Rahimipour1 , Mahsa Morsali1 , Maedeh Radayi1 , Samaneh Tourani1
, Anis Hosseini1 , Shahrbanoo Ghaharri2 , Shohreh Jalaie *3 , Zahra Validabadi2 , Jean L. DesJardin4 , Samin Moradi1 , Sahand Rahimipour1 , Mahsa Morsali1 , Maedeh Radayi1 , Samaneh Tourani1
, Anis Hosseini1 , Shahrbanoo Ghaharri2 , Shohreh Jalaie *3 , Zahra Validabadi2 , Jean L. DesJardin4 , Samin Moradi1 , Sahand Rahimipour1 , Mahsa Morsali1 , Maedeh Radayi1 , Samaneh Tourani1
1- Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Mental Health, School of Behavioral Sciences and Mental Health, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. ,jalaeish@tums.ac.ir
4- Department of Education, Moravian University, Bethlehem, United States.
2- Department of Mental Health, School of Behavioral Sciences and Mental Health, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Physiotherapy, School of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran. ,
4- Department of Education, Moravian University, Bethlehem, United States.
Keywords: Self-efficacy, Hard-of-hearing children, Deafness, Early intervention, SPISE-R, Persian language
Full-Text [PDF 773 kb]
(79 Downloads)
| Abstract (HTML) (284 Views)
دستورالعمل: در پاسخ به هر سوال دور شماره مورد نظرتان (از یک تا هفت را که احتمال بیشتر میدهید)، دایره بکشید.
الف) باورها
سوالات زیر مواردی هستندکه برخی از والدین کودکان کمشنوا ممکن است به آن اعتقاد، یا نگرانیهایی درباره آن داشته باشند. لطفاً مشخص کنید که چقدر به این موارد اعتقاد و باور دارید.

ب) اطلاعات:
هنگامی که والدین، دارای فرزند کمشنوا میشوند؛ باید اطلاعات و مهارتهای جدید بسیاری را بیاموزند و این فرایندی زمان بر است. میخواهیم بدانیم که شما در حال حاضر درباره هر یک از موضوعات زیر چقدر آگاه هستید و اطلاعات دارید.

ج) اطمینان:
داشتن اطلاعات به تنهایی همیشه ما را در انجام کاری مطمئن و آسوده نمیکند. ممکن است برای ایجاد اطمینان و اعتماد به خود، به زمان یا تمرین بیشتری نیاز داشته باشیم. لطفاً مشخص کنید که چقدر نسبت به توانایی خود در انجام هر یک از کارهای زیر اطمینان دارید.


د) اقدامات :
میدانیم که در طی روز مشغلههای زیادی داریم. والدین مسئولیتهای بسیاری دارند. از این رو ممکن است نتوانیم همه کارهایی را که دوست داریم، هرروز انجام دهیم. می خواهیم بدانیم با در نظر گرفتن همه مسئولیت های دیگری که دارید، شما چه میزان قادر به انجام فعالیت های زیر هستید؟


ه) استفاده از "سمعک یا کاشت حلزون":
میخواهیم بدانیم فرزند شما روزانه در هنگام بیداری به طور معمول چقدر از «سمعک یا کاشت حلزون" خود استفاده میکند. اگر کودک شما در یک گوش سمعک و در گوش دیگر کاشت حلزون دارد و در میزان استفاده از آنها تفاوتی وجود دارد، لطفاً برای هر دستگاه به طور جداگانه پاسخ دهید. (در صورت نیاز در جدول از کلمه های «کاشت حلزون» و»سمعک» استفاده کنید.)
1. فرزندتان در طی شبانهروز معمولا چند ساعت بیدار است ؟ ---------------
2. فرزندتان هنگامی که بیدار است، معمولا چند ساعت از سمعک یا کاشت حلزون خود استفاده میکند؟ ---------------
3. اگر فرزندتان تا به حال با سمعک یا کاشت حلزون روشن روی گوشش خوابیده است، لطفا مشخص کنید به طور معمول چند ساعت در شبانه روز این اتفاق میافتد؟ ---------------
4. هنگامی که فرزندتان در موقعیتهای زیر بیدار است، چقدر از سمعک یا کاشت حلزون خود استفاده میکند؟
مشخصات پاسخ دهنده به سوالات پرسشنامه
والدین: پدر مادر
سن والد: ..........
وضعیت شنوایی والد: شنوا کم شنوا ناشنوا
سطح تحصیلات والد: ابتدایی دیپلم لیسانس فوق لیسانس دکترا
وضعیت شغلی والد: شاغل غیرشاغل
تعداد فرزند کم شنوا در خانواده: یکی دو تا سه تا
سن کودک (به سال): ..........
جنسیت کودک: دختر پسر
سن تشخیص کم شنوایی: 12 ماهگی یا قبل بعد از 12 ماهگی
میزان کم شنوایی گوش بهتر (براساس آزمایش شنوایی بدون وسیله تقویت کننده):
ملایم تا متوسط (مسطح یا با شیب ملایم در فرکانسهای بالا)
متوسط تا شدید
شدید
عمیق
میزان کم شنوایی گوش بهتر (براساس آزمایش شنوایی با استفاده از وسیله تقویت کننده):
جزئی (نزدیک به محدوده طبیعی) ملایم متوسط متوسط شدید شدید عمیق
نوع روش ارتباطی: شنیداری-کلامی شفاهی (گفتاری و لبخوانی)
ارتباط کلی (گفتاری، لبخوانی و زبان اشاره) زبان اشاره و لبخوانی
وجود مشکلات دیگر علاوه بر کم شنوایی (درصورت پاسخ بلی، نوع آن نوشته شود): بلی خیر
توضیح: ..........
نوع وسیله کمک شنوایی (در حال حاضر): سمعک دو گوشی سمعک یک گوشی (گوش بهتر یا بدتر)
کاشت حلزون یکطرفه کاشت حلزون دوطرفه
در چه سنی (برحسب ماه)، کم شنوایی توسط متخصصین تایید شد؟ ..........
در چه سنی (برحسب ماه)، سمعک دریافت و استفاده شد؟ ..........
در چه سنی (برحسب ماه)، دستگاه کاشت حلزون دریافت و استفاده شد؟ ..........
Full-Text: (42 Views)
Introduction
Language development in children is shaped by a dynamic interplay of biological and environmental factors, with hearing status playing a central role. For children with typical development, language acquisition predominantly occurs through auditory-verbal communication. In contrast, deaf and hard-of-hearing (D/HH) children often rely on additional modalities, such as sign language and lip reading, to learn language [1]. Beyond internal factors, like hearing status, the environment plays a critical role in shaping language development. Early exposure to rich and diverse linguistic input is vital for fostering language growth [2]. Research has demonstrated that D/HH children receiving sufficient and high-quality linguistic input in their early years exhibit better language outcomes than those with limited exposure [3].
As primary caregivers, parents provide essential linguistic input that shapes their D/HH child’s language trajectory. Parental self-efficacy—the belief in one’s ability to effectively fulfil parenting responsibilities—has shown to positively influence parents’ involvement and resourcefulness in addressing challenges [4]. In the context of D/HH children, higher parental self-efficacy beliefs are associated with greater engagement in activities that promote language development, while lower self-efficacy may hinder involvement, potentially contributing to language deprivation [5].
Early intervention programs for D/HH children increasingly focus on empowering parents with the knowledge and confidence needed to support their child’s development. These programs aim to enhance parental involvement through family-centered approaches that provide language and communication support, emotional and psychosocial guidance, and education on communication modalities and other D/HH-related topics. Given the critical role of parental beliefs in influencing child outcomes, accurately measuring parental self-efficacy during early intervention is crucial for tailoring interventions and evaluating program effectiveness.
Several valid tools have been developed in English to systematically assess parental self-efficacy and involvement in early intervention, including the scale of parental involvement and self-efficacy-revised (SPISE-R) [5-7]. However, a few Persian tools are available to check the language and communication skills of Persian hearing-impaired children [8-11] and no proper instrument exists to examine parents’ beliefs and self-efficacy. Although the old version of the SPISE was translated into Persian [12], its psychometric characteristics have not been examined. The SPISE-R is newer and more comprehensive than the others; therefore, it was selected for translation. This questionnaire, originally developed in English, systematically has five subscales, including beliefs (7 questions), knowledge subscale (10 questions), confidence subscale (10 questions), and actions subscale (15 questions) related to supporting their children’s auditory access and language development. The final section of the questionnaire asks parents to report the amount of time their child uses hearing assistive devices during the day [5]. Thus, this study aimed to translate and adapt a valid and reliable Persian tool for assessing parental self-efficacy in the context of childhood hearing loss by translating the SPISE-R and examining its psychometric properties.
Materials and Methods
This cross-sectional study aimed to translate and validate a Persian version of the SPISE-R through translation and psychometric evaluation.
Phase I: Translation process
First, permission to translate the questionnaire in Persian was obtained from its authors. Then the international quality of life assessment (IQOLA) protocol [13] was followed and involved two main phases: forward and backward translations.
Forward translation
Two native Persian-speaking translators with sufficient English proficiency (Translators 1 and 2) independently translated the questionnaire into Persian. They provided alternative translations for specific terms when necessary. Each translator rated the translation difficulty for each item on a scale from 0 (easy) to 100 (difficult). Items with an average score above 50 were flagged as difficult to translate. The translators collaboratively developed a consensus Persian version of the questionnaire. The consensus Persian version was reviewed by two additional translators (Translators 3 and 4) who evaluated its quality compared to the original English version. They rated each item’s clarity, conceptual equivalence (similarity in meaning), and appropriateness of language on a scale from 1 (very low) to 5 (very high). This process ensured the production of an acceptable Persian version.
Backward translation
Two other native Persian-speaking translators fluent in English (translators 5 and 6) independently translated the Persian version back into English. Their translations were compared with the original English questionnaire to assess alignment and accuracy and were approved by the developers of the original English version.
This rigorous process ensured that the Persian version of the SPISE-R maintained linguistic, cultural, and conceptual equivalence to the original questionnaire (Appendix 1).
Phase II: Psychometric evaluation
Parents were asked to complete the questionnaire if their child met the following criteria: a) 48 months of age or younger, b) using at least one hearing aid or cochlear implant, c) learning spoken language, and d) no known conditions other than hearing loss. To evaluate the psychometric characteristics of the Persian version of the SPISE-R, several measures were assessed, including cultural adaptation, face validity, concurrent validity, and reliability.
Cultural adaptation: The cultural adaptation of the questionnaire was assessed using the content validity ratio (CVR) and content validity index (CVI). A panel of 9 experts, including audiologists and psychologists, rated the appropriateness of each item on a 3-point Likert scale (1=suitable, 2=moderate, and 3=unsuitable). The CVR was then calculated [4].
Face validity index (FVI): To assess face validity, 10 experts and 34 parents (mothers and fathers) rated the clarity and fluency of the translated questionnaire. They used a 6-point Likert scale: very weak, weak, moderate, good, very good, and best. This evaluation focused on whether the items used meaningful, easy-to-understand language appropriate for the target population.
Concurrent and discriminant validity: As no existing questionnaire served as a standard for comparison, we developed a researcher-made questionnaire with items similar to those in the SPISE-R (Appendix 1). Two audiologists independently scored this new questionnaire. We then compared their scores with the responses from 25 mothers and fathers who completed the translated SPISE-R. The comparison focused on the beliefs, confidence, and action subscales, which were rated using the 7-point Likert scale.
For concurrent validity, three scores were calculated for each subscale. In the beliefs section, responses were categorized as “negative”, “intermediate”, or “positive”: values of 1-2 were classified as “negative”, 3-4 as “intermediate”, and 5-7 as “positive” (with questions 5, 6, and 7 scored in reverse). In the confidence section, responses were categorized into “ineffective”, “intermediate”, and “effective” levels, similar to the beliefs section. For the action subscale, responses were classified as “weak”, “moderate”, or “excellent”, based on the levels of parent responses. These categories were then compared across the subscales for consistency and validity.
For discriminant validity, we collected responses from the audiologist to the researcher-made questionnaire in the confidence and action subscales. Based on these responses, parents were divided into two groups, including average and high, and the mean scores of their self-efficacy and action subscales were compared with the scores of the main questionnaire using an independent t-test and the non-parametric Mann-Whitney U test.
Test re-test reliability: A total of 78 mothers and fathers were initially asked to complete the questionnaire. Of these, 37 participants completed the questionnaire again after a one-month interval. This test re-test procedure helped to assess the reliability of the translated SPISE-R, providing information on its consistency over time. The sample size was estimated based on prior studies. All parents first filled out the informed consent form, then if they were willing to cooperate, entered the study.
Statistical analysis
SPSS software, version 26 was employed for data analysis. CVR, CVI, FVIs, and impact scores were used to evaluate cultural adaptation and face validity. Test re-test reliability and internal consistency were examined using intra-class correlation coefficient (ICC) and Cronbach’s α. Pearson correlation coefficients and ICCs were used to assess the link between each item’s test re-test score. The degree of agreement between clinical scores from audiologists and the new questionnaire for each item was calculated as concurrent validity. P<0.5 were considered significant for all analyses.
Results
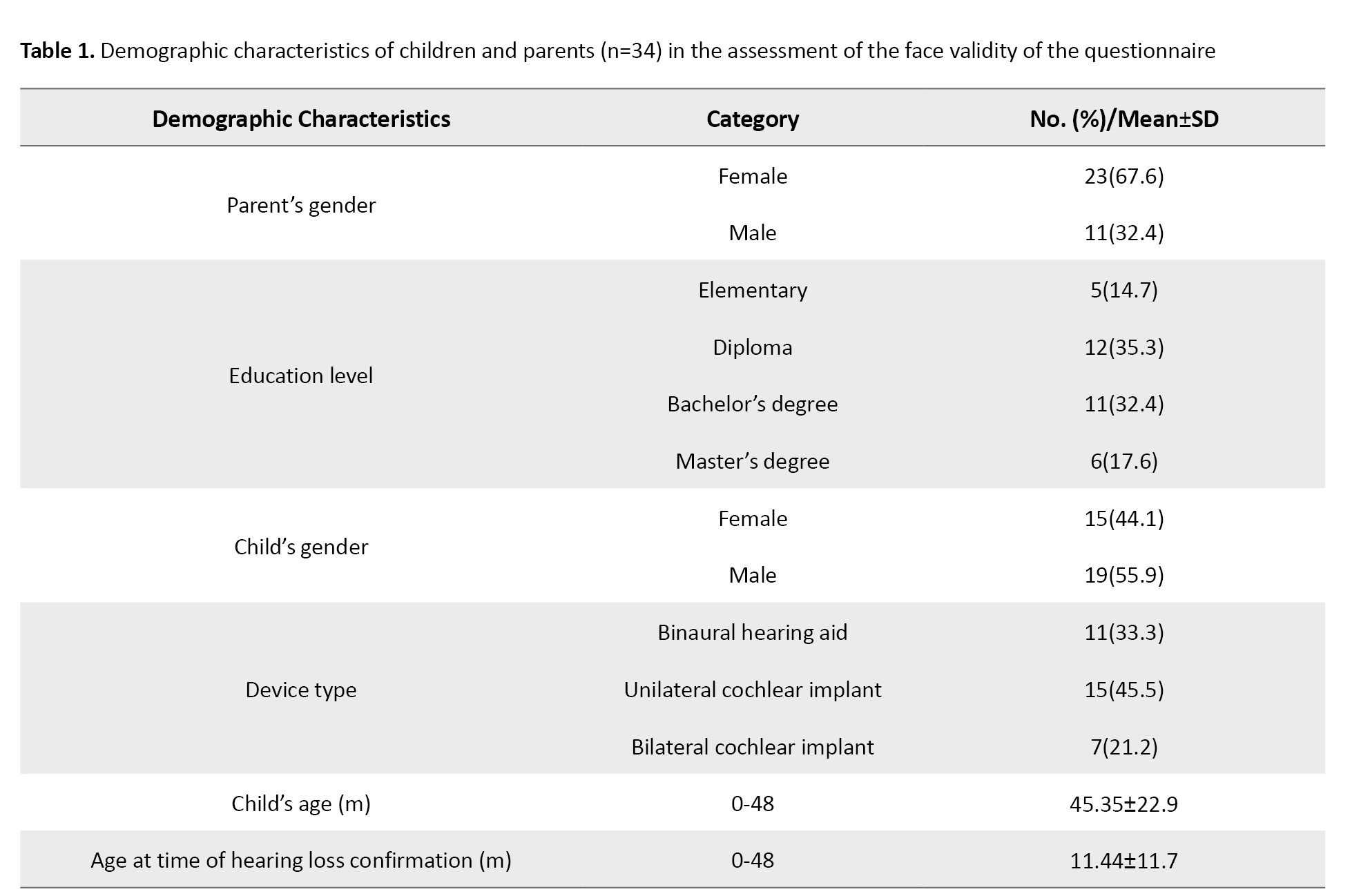
Demographic characteristics of the patients involved in the face validity assessment were gathered from 34 individuals. The majority were mothers, 23(67.6%), compared with fathers, 11(32.4%). The mean age of the children was 45.35(22.9) months, while the mean age at confirmation of hearing loss was 11.44(11.7) months. Eleven children (33.3%) reported using binaural hearing aids, 15 children (45.4%) had unilateral cochlear implants, and 7 children (21.2%) reported wearing bilateral cochlear implants (Table 1).
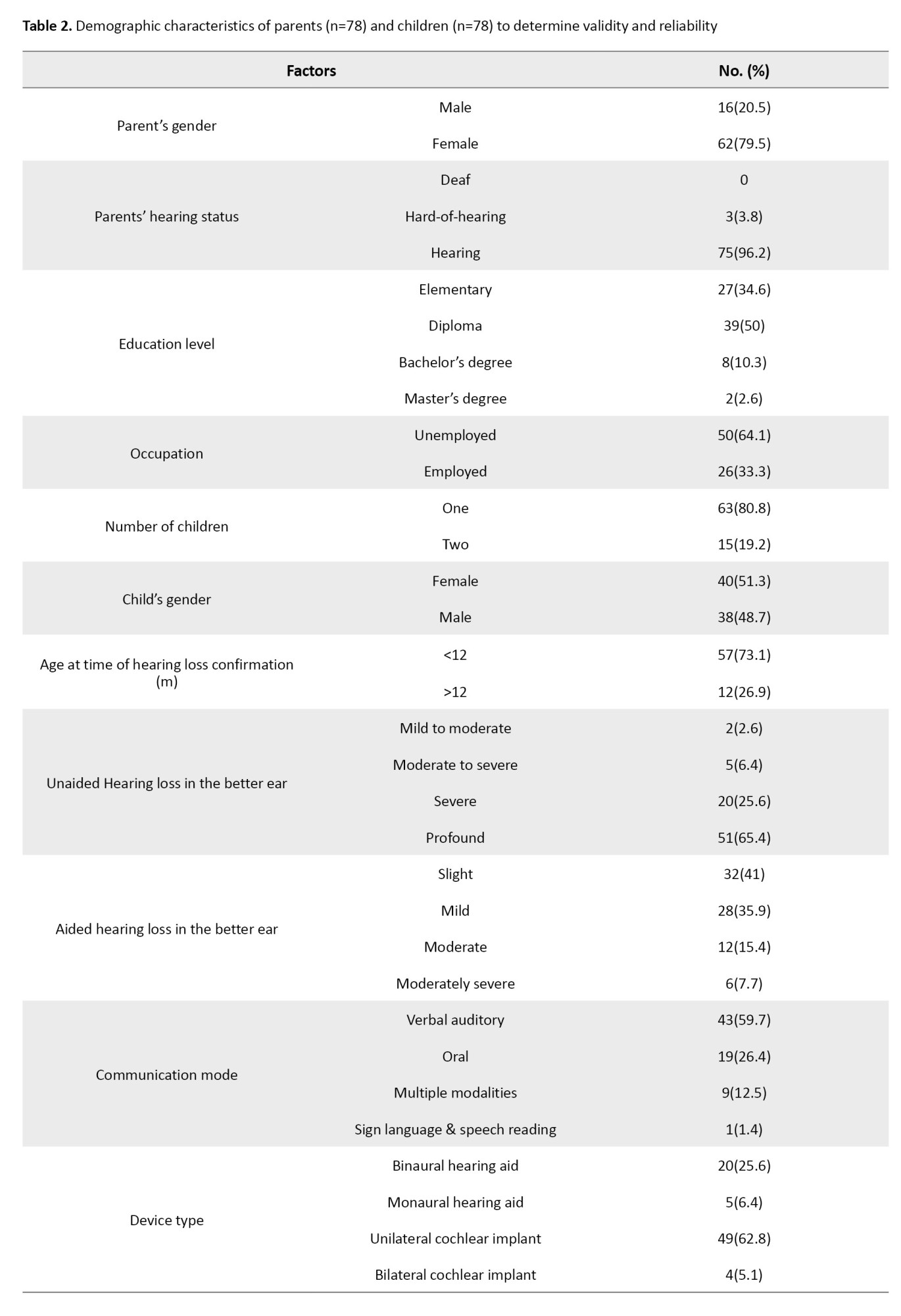
A reliability and descriptive study was conducted, including 78 children, with 62 (79.5%) being mothers and 16 (20.5%) being fathers: 25 children reported using hearing aids (25.6% binaural and 6.4% monaural), and 53 children reported wearing cochlear implants (62.8% unilateral and 5.1% bilateral). Confirmation of hearing loss was obtained in 57 cases (73.1%) before 12 months, while hearing loss was detected after 12 months in 12 cases (26.9%). Participant demographics, including parental age, education level, and child hearing status, are summarized in Tables 1 and 2.
Based on the 9 experts’ reviews, the minimum acceptable CVR and item-level CVI (I-CVI) for this analysis were set at 0.77 and 0.70, respectively. The results showed that the CVRs for all items in the questionnaire were above the acceptable threshold, indicating that each item had an appropriate validity score (Table 3).


The item-face validity indices (I-FVIs) for item appropriateness and fluency ranged from 0.72 to 1.0. For the cultural appropriateness specific to Iranian culture, the I-FVIs ranged from 0.79 to 1.0. The S-FVIs were 0.94 and 0.95, respectively. A threshold greater than 0.70 was considered acceptable for FVI. However, further assessments are needed for FVI values between 0.7 and 0.8.
Regarding impact scores, all items had acceptable ratings. An impact score greater than 1.5 was considered satisfactory (Table 3).
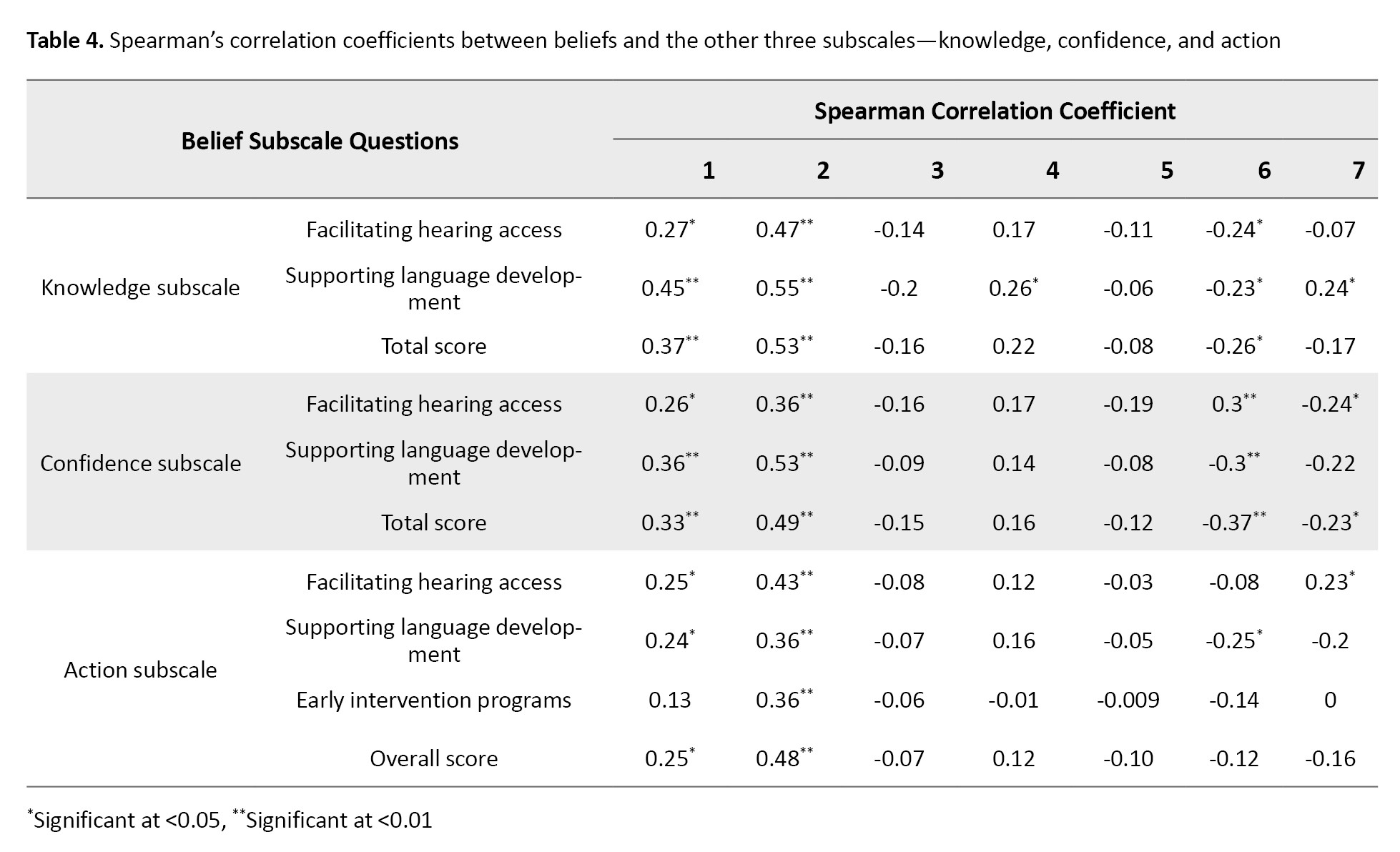
Table 3 represents Spearman’s correlation coefficients between the seven questions of beliefs and the knowledge subscale (facilitating hearing access and supporting language development), confidence subscale (facilitating hearing access and supporting language development), and action subscale (facilitating hearing access, supporting language development, and early intervention programs).
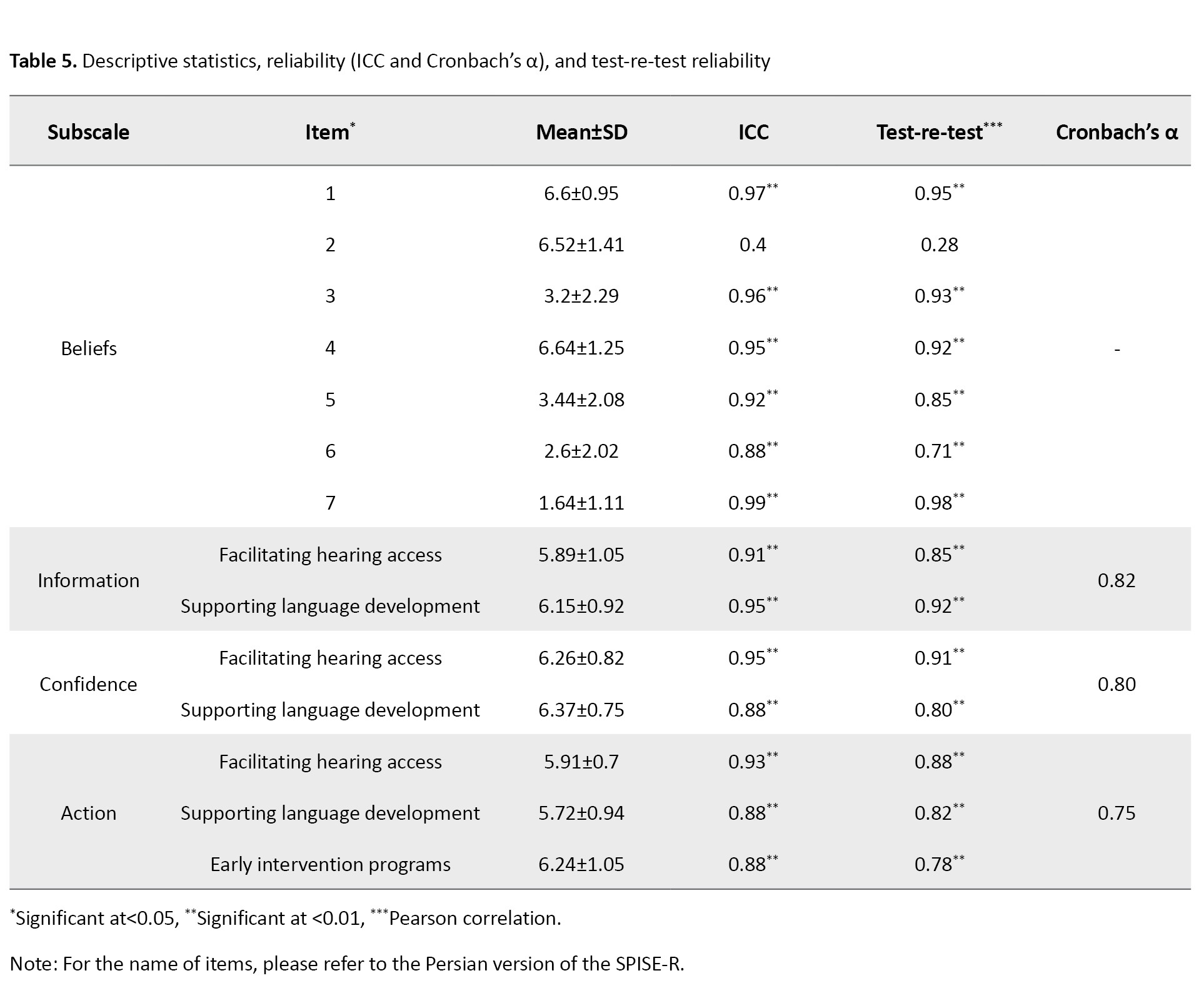
The results showed that in the beliefs section, question 2 had the most significant positive relationship with other sections, followed by question 1, which exhibited the second strongest positive relationship. Although questions 3-5 demonstrated a positive relationship with the support of language development in the knowledge section, these relationships were not statistically significant. Conversely, questions 6 and 7 revealed a negative relationship in some situations, with several instances showing a significant negative relationship. The total score of knowledge and questions 3, 4, 5, and 7 showed no significant differences. The total confidence score showed no significant difference with questions 3, 4, 5, and 7 of the beliefs section. The total score of action subscale showed a positive significant difference only relative to questions 1 and 2 of the beliefs section, and the rest of the questions did not show any statistically significant (P<0.05). However, there was a significant positive relationship between the total knowledge subscale score and the total confidence score (r=0.73, P<0.001), as well as between the total knowledge subscale score and action subscale (r=0.61, P<0.001), and between the total confidence subscale score and action subscale (r=0.70, P<0.001). This indicates a strong positive relationship between parental knowledge and confidence. The Mean±SD, ICC, Cronbach’s α coefficient, and Pearson’s correlation coefficient of all questions related to the beliefs section, total scores, and subscale scores of the domains were analyzed. The knowledge, confidence, and action subscales had a sufficient level of consistency, with Cronbach’s α values ranging from 0.75 to 0.82 for beliefs-related items. The consistency of the knowledge, confidence, and action subscales was confirmed through test re-test Pearson correlations, with values ranging from 0.71 to 0.98, except for the second item in the beliefs section. Additionally, the ICCs demonstrated strong relevance for individuals and factors, as summarized in Table 5.
The concurrent validity of the questionnaire was assessed by examining the association and agreement between audiologists’ clinical judgments and parents’ self-efficacy and participation scores on the confidence and action subscales. Audiologists used a 7-point Likert scale to categorize self-efficacy into three levels: “Inefficient” (scores 1–2), “intermediate” (scores 3–4), and “efficient” (scores 5–7). Scores of “1–2” were categorized as “inefficient,” “3–4” as “intermediate,” and “5–7” as “effective” for calculating the confidence subscale. Expert evaluations categorized as “weak,” “moderate,” and “excellent” were included in the participation section. These evaluations were aligned with the action subscale responses, where scores of “1–2” represented “weak,” “3–4” represented “moderate,” and “5–7” represented “excellent.” The results of the specialists’ evaluations for self-efficacy in the confidence subscale showed a correlation coefficient of 0.55, an ICC of 0.65, and an agreement rate of 0.76 (13 out of 17 items). For the action subscale, the correlation coefficient was 0.31, the ICC was 0.47, and the agreement rate was 0.82 (14 out of 17 items). These values suggest moderate agreement between audiologists’ evaluations and parent-reported scores. Both parents completed the questionnaire, and the results showed no significant difference in their knowledge levels for the subgroups of facilitating hearing access (Z=-0.83, P=0.40) and language development (Z=-1.24, P=0.21). However, mothers scored significantly higher than fathers in both the confidence and action subscales. Statistically significant differences were observed in the following areas: the confidence subscale for facilitating hearing access (Z=-2.33, P=0.02), the confidence subscale for supporting language development (Z=-3.40, P=0.001), and the action subscale for facilitating hearing access (Z=-1.88, P=0.05). The gender-based findings are compelling and suggest that mothers may perceive themselves as more confident and engaged in supporting their child’s auditory and language development.
Discussion
The coaching model, which fosters collaboration between professionals and parents, is central to early intervention for D/HH children from birth to age three. The ultimate aim is to empower parents and caregivers with the knowledge and confidence to independently implement their children’s individualized program goals without ongoing professional involvement. Parents participating in early intervention exhibit varying levels of beliefs and self-efficacy concerning their children’s hearing loss [5]. By thoroughly understanding parents’ strengths and identifying areas where they seek guidance, professionals can better support parents in achieving these goals.
The SPISE-R serves as a valuable tool for identifying parents’ capacities in terms of their beliefs, knowledge, and confidence in supporting a child with hearing loss. It provides insights that allow for tailored counseling, training, and guidance during early intervention. Given its usefulness, translating the SPISE-R into Persian was imperative to extend its applicability to Persian-speaking populations.
The Persian version demonstrated strong cultural compatibility across all five sections (CVR=0.77–1) and was highly comprehensible to families (S-FVI=0.94). Unlike the English [5] and Korean [14] versions, which have not published their content and face validity metrics, the Persian version provides these values, enhancing transparency and replicability. Additionally, the Persian version exhibited acceptable reliability, with no significant differences between test and re-test results, consistent with findings from the original and Korean versions.
Grounded in social learning theory, parental self-efficacy refers to parents’ beliefs in their ability to fulfil parenting tasks [15, 4]. Previous research demonstrates a strong association between parents’ task-specific self-efficacy and child language outcomes in children with hearing loss [3]. Higher confidence levels are linked to greater engagement in actions [5]. Consequently, parents play a pivotal role in enabling their child’s hearing access and fostering language development.
In terms of gender effects, we found no significant differences based on whether the father or mother completed the questionnaire. However, mothers scored higher than fathers in the confidence and action subscales. These differences were statistically significant for the confidence subscale in facilitating hearing access (Z=-2.33, P=0.02) and language development (Z=-3.40, P=0.001), as well as for the action subscale in facilitating hearing access (Z=-1.88, P=0.05). These findings may reflect greater maternal involvement, as mothers were predominantly unemployed and had more available time compared with fathers, and intervention programs may benefit from actively engaging fathers and addressing potential barriers to their involvement. Another study reported higher self-efficacy among mothers in managing their child’s hearing loss [16]. These results underscore the need to assess the unique strengths and needs of both parents when designing early intervention programs.
Parents’ beliefs about hearing loss significantly influence their self-efficacy and engagement in early intervention programs. Several factors, including gender, education level, and occupation, can shape these beliefs and their participation [4]. Additionally, child-specific factors, such as the age of hearing loss diagnosis, the timing of early intervention, the type of hearing devices, and the presence of comorbidities, may impact parents’ self-efficacy and involvement. Future research should explore how the SPISE-R can be utilized to assess these variables, thereby further refining early intervention strategies. The Persian version of the SPISE-R, like its English [5] and Korean [14] counterparts, is a valid and reliable tool.
Insights derived from the questionnaire can effectively highlight both parents’ resources and areas requiring additional support. The SPISE-R will be valuable in identifying families of children with hearing loss who may benefit from further counselling, education, and training to better support their child’s development. To enhance its clinical utility, future studies should focus on developing detailed implementation guidelines for its use in practice.
Conclusion
The validated Persian SPISE-R offers clinicians and researchers a culturally appropriate tool (CVR=0.77–1, S-FVI=0.94) to assess and support parental engagement in early intervention. Future work should focus on implementation protocols and longitudinal studies to evaluate its impact on child outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.REC.1400.492) on 29 August 2021. The participants received written and oral information about the study and provided consent to participate.
Funding
This study is part of a research plan accepted by the School of Rehabilitation Sciences at Iran University of Medical Sciences (Grant No.: 19626).
Authors' contributions
Methodology, formal analysis, and supervision: Shohreh Jalaie; Literature review: Zahra Validabadi, Maedeh Radayi; Investigation and data collection: Samaneh Tourani; Data curation, validation, and conceptual equivalence assessment: Shahrbanoo Ghaharri; Instrument validation and English questionnaire editing: Jean L. DesJardin; Writing: Anis Hosseini, Shohreh Jalaie and Mahsa Morsali; Translation: Anis Hosseini, Zahra Validabadi, Samin Moradi, and Sahand Rahimipour.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the participants in the study. Special thanks to Zhila Afsharmanesh, Majid Karimi, Soheila Shayanmehr and Afsaneh Alinejad. They would also like to show their gratitude toward the Cochlear Implant Center in Kerman City and the Cochlear Implant Center in Ahvaz City for their referrals.
References
Language development in children is shaped by a dynamic interplay of biological and environmental factors, with hearing status playing a central role. For children with typical development, language acquisition predominantly occurs through auditory-verbal communication. In contrast, deaf and hard-of-hearing (D/HH) children often rely on additional modalities, such as sign language and lip reading, to learn language [1]. Beyond internal factors, like hearing status, the environment plays a critical role in shaping language development. Early exposure to rich and diverse linguistic input is vital for fostering language growth [2]. Research has demonstrated that D/HH children receiving sufficient and high-quality linguistic input in their early years exhibit better language outcomes than those with limited exposure [3].
As primary caregivers, parents provide essential linguistic input that shapes their D/HH child’s language trajectory. Parental self-efficacy—the belief in one’s ability to effectively fulfil parenting responsibilities—has shown to positively influence parents’ involvement and resourcefulness in addressing challenges [4]. In the context of D/HH children, higher parental self-efficacy beliefs are associated with greater engagement in activities that promote language development, while lower self-efficacy may hinder involvement, potentially contributing to language deprivation [5].
Early intervention programs for D/HH children increasingly focus on empowering parents with the knowledge and confidence needed to support their child’s development. These programs aim to enhance parental involvement through family-centered approaches that provide language and communication support, emotional and psychosocial guidance, and education on communication modalities and other D/HH-related topics. Given the critical role of parental beliefs in influencing child outcomes, accurately measuring parental self-efficacy during early intervention is crucial for tailoring interventions and evaluating program effectiveness.
Several valid tools have been developed in English to systematically assess parental self-efficacy and involvement in early intervention, including the scale of parental involvement and self-efficacy-revised (SPISE-R) [5-7]. However, a few Persian tools are available to check the language and communication skills of Persian hearing-impaired children [8-11] and no proper instrument exists to examine parents’ beliefs and self-efficacy. Although the old version of the SPISE was translated into Persian [12], its psychometric characteristics have not been examined. The SPISE-R is newer and more comprehensive than the others; therefore, it was selected for translation. This questionnaire, originally developed in English, systematically has five subscales, including beliefs (7 questions), knowledge subscale (10 questions), confidence subscale (10 questions), and actions subscale (15 questions) related to supporting their children’s auditory access and language development. The final section of the questionnaire asks parents to report the amount of time their child uses hearing assistive devices during the day [5]. Thus, this study aimed to translate and adapt a valid and reliable Persian tool for assessing parental self-efficacy in the context of childhood hearing loss by translating the SPISE-R and examining its psychometric properties.
Materials and Methods
This cross-sectional study aimed to translate and validate a Persian version of the SPISE-R through translation and psychometric evaluation.
Phase I: Translation process
First, permission to translate the questionnaire in Persian was obtained from its authors. Then the international quality of life assessment (IQOLA) protocol [13] was followed and involved two main phases: forward and backward translations.
Forward translation
Two native Persian-speaking translators with sufficient English proficiency (Translators 1 and 2) independently translated the questionnaire into Persian. They provided alternative translations for specific terms when necessary. Each translator rated the translation difficulty for each item on a scale from 0 (easy) to 100 (difficult). Items with an average score above 50 were flagged as difficult to translate. The translators collaboratively developed a consensus Persian version of the questionnaire. The consensus Persian version was reviewed by two additional translators (Translators 3 and 4) who evaluated its quality compared to the original English version. They rated each item’s clarity, conceptual equivalence (similarity in meaning), and appropriateness of language on a scale from 1 (very low) to 5 (very high). This process ensured the production of an acceptable Persian version.
Backward translation
Two other native Persian-speaking translators fluent in English (translators 5 and 6) independently translated the Persian version back into English. Their translations were compared with the original English questionnaire to assess alignment and accuracy and were approved by the developers of the original English version.
This rigorous process ensured that the Persian version of the SPISE-R maintained linguistic, cultural, and conceptual equivalence to the original questionnaire (Appendix 1).
Phase II: Psychometric evaluation
Parents were asked to complete the questionnaire if their child met the following criteria: a) 48 months of age or younger, b) using at least one hearing aid or cochlear implant, c) learning spoken language, and d) no known conditions other than hearing loss. To evaluate the psychometric characteristics of the Persian version of the SPISE-R, several measures were assessed, including cultural adaptation, face validity, concurrent validity, and reliability.
Cultural adaptation: The cultural adaptation of the questionnaire was assessed using the content validity ratio (CVR) and content validity index (CVI). A panel of 9 experts, including audiologists and psychologists, rated the appropriateness of each item on a 3-point Likert scale (1=suitable, 2=moderate, and 3=unsuitable). The CVR was then calculated [4].
Face validity index (FVI): To assess face validity, 10 experts and 34 parents (mothers and fathers) rated the clarity and fluency of the translated questionnaire. They used a 6-point Likert scale: very weak, weak, moderate, good, very good, and best. This evaluation focused on whether the items used meaningful, easy-to-understand language appropriate for the target population.
Concurrent and discriminant validity: As no existing questionnaire served as a standard for comparison, we developed a researcher-made questionnaire with items similar to those in the SPISE-R (Appendix 1). Two audiologists independently scored this new questionnaire. We then compared their scores with the responses from 25 mothers and fathers who completed the translated SPISE-R. The comparison focused on the beliefs, confidence, and action subscales, which were rated using the 7-point Likert scale.
For concurrent validity, three scores were calculated for each subscale. In the beliefs section, responses were categorized as “negative”, “intermediate”, or “positive”: values of 1-2 were classified as “negative”, 3-4 as “intermediate”, and 5-7 as “positive” (with questions 5, 6, and 7 scored in reverse). In the confidence section, responses were categorized into “ineffective”, “intermediate”, and “effective” levels, similar to the beliefs section. For the action subscale, responses were classified as “weak”, “moderate”, or “excellent”, based on the levels of parent responses. These categories were then compared across the subscales for consistency and validity.
For discriminant validity, we collected responses from the audiologist to the researcher-made questionnaire in the confidence and action subscales. Based on these responses, parents were divided into two groups, including average and high, and the mean scores of their self-efficacy and action subscales were compared with the scores of the main questionnaire using an independent t-test and the non-parametric Mann-Whitney U test.
Test re-test reliability: A total of 78 mothers and fathers were initially asked to complete the questionnaire. Of these, 37 participants completed the questionnaire again after a one-month interval. This test re-test procedure helped to assess the reliability of the translated SPISE-R, providing information on its consistency over time. The sample size was estimated based on prior studies. All parents first filled out the informed consent form, then if they were willing to cooperate, entered the study.
Statistical analysis
SPSS software, version 26 was employed for data analysis. CVR, CVI, FVIs, and impact scores were used to evaluate cultural adaptation and face validity. Test re-test reliability and internal consistency were examined using intra-class correlation coefficient (ICC) and Cronbach’s α. Pearson correlation coefficients and ICCs were used to assess the link between each item’s test re-test score. The degree of agreement between clinical scores from audiologists and the new questionnaire for each item was calculated as concurrent validity. P<0.5 were considered significant for all analyses.
Results
Demographic characteristics of the patients involved in the face validity assessment were gathered from 34 individuals. The majority were mothers, 23(67.6%), compared with fathers, 11(32.4%). The mean age of the children was 45.35(22.9) months, while the mean age at confirmation of hearing loss was 11.44(11.7) months. Eleven children (33.3%) reported using binaural hearing aids, 15 children (45.4%) had unilateral cochlear implants, and 7 children (21.2%) reported wearing bilateral cochlear implants (Table 1).
A reliability and descriptive study was conducted, including 78 children, with 62 (79.5%) being mothers and 16 (20.5%) being fathers: 25 children reported using hearing aids (25.6% binaural and 6.4% monaural), and 53 children reported wearing cochlear implants (62.8% unilateral and 5.1% bilateral). Confirmation of hearing loss was obtained in 57 cases (73.1%) before 12 months, while hearing loss was detected after 12 months in 12 cases (26.9%). Participant demographics, including parental age, education level, and child hearing status, are summarized in Tables 1 and 2.
Based on the 9 experts’ reviews, the minimum acceptable CVR and item-level CVI (I-CVI) for this analysis were set at 0.77 and 0.70, respectively. The results showed that the CVRs for all items in the questionnaire were above the acceptable threshold, indicating that each item had an appropriate validity score (Table 3).
The item-face validity indices (I-FVIs) for item appropriateness and fluency ranged from 0.72 to 1.0. For the cultural appropriateness specific to Iranian culture, the I-FVIs ranged from 0.79 to 1.0. The S-FVIs were 0.94 and 0.95, respectively. A threshold greater than 0.70 was considered acceptable for FVI. However, further assessments are needed for FVI values between 0.7 and 0.8.
Regarding impact scores, all items had acceptable ratings. An impact score greater than 1.5 was considered satisfactory (Table 3).
Table 3 represents Spearman’s correlation coefficients between the seven questions of beliefs and the knowledge subscale (facilitating hearing access and supporting language development), confidence subscale (facilitating hearing access and supporting language development), and action subscale (facilitating hearing access, supporting language development, and early intervention programs).
The results showed that in the beliefs section, question 2 had the most significant positive relationship with other sections, followed by question 1, which exhibited the second strongest positive relationship. Although questions 3-5 demonstrated a positive relationship with the support of language development in the knowledge section, these relationships were not statistically significant. Conversely, questions 6 and 7 revealed a negative relationship in some situations, with several instances showing a significant negative relationship. The total score of knowledge and questions 3, 4, 5, and 7 showed no significant differences. The total confidence score showed no significant difference with questions 3, 4, 5, and 7 of the beliefs section. The total score of action subscale showed a positive significant difference only relative to questions 1 and 2 of the beliefs section, and the rest of the questions did not show any statistically significant (P<0.05). However, there was a significant positive relationship between the total knowledge subscale score and the total confidence score (r=0.73, P<0.001), as well as between the total knowledge subscale score and action subscale (r=0.61, P<0.001), and between the total confidence subscale score and action subscale (r=0.70, P<0.001). This indicates a strong positive relationship between parental knowledge and confidence. The Mean±SD, ICC, Cronbach’s α coefficient, and Pearson’s correlation coefficient of all questions related to the beliefs section, total scores, and subscale scores of the domains were analyzed. The knowledge, confidence, and action subscales had a sufficient level of consistency, with Cronbach’s α values ranging from 0.75 to 0.82 for beliefs-related items. The consistency of the knowledge, confidence, and action subscales was confirmed through test re-test Pearson correlations, with values ranging from 0.71 to 0.98, except for the second item in the beliefs section. Additionally, the ICCs demonstrated strong relevance for individuals and factors, as summarized in Table 5.
The concurrent validity of the questionnaire was assessed by examining the association and agreement between audiologists’ clinical judgments and parents’ self-efficacy and participation scores on the confidence and action subscales. Audiologists used a 7-point Likert scale to categorize self-efficacy into three levels: “Inefficient” (scores 1–2), “intermediate” (scores 3–4), and “efficient” (scores 5–7). Scores of “1–2” were categorized as “inefficient,” “3–4” as “intermediate,” and “5–7” as “effective” for calculating the confidence subscale. Expert evaluations categorized as “weak,” “moderate,” and “excellent” were included in the participation section. These evaluations were aligned with the action subscale responses, where scores of “1–2” represented “weak,” “3–4” represented “moderate,” and “5–7” represented “excellent.” The results of the specialists’ evaluations for self-efficacy in the confidence subscale showed a correlation coefficient of 0.55, an ICC of 0.65, and an agreement rate of 0.76 (13 out of 17 items). For the action subscale, the correlation coefficient was 0.31, the ICC was 0.47, and the agreement rate was 0.82 (14 out of 17 items). These values suggest moderate agreement between audiologists’ evaluations and parent-reported scores. Both parents completed the questionnaire, and the results showed no significant difference in their knowledge levels for the subgroups of facilitating hearing access (Z=-0.83, P=0.40) and language development (Z=-1.24, P=0.21). However, mothers scored significantly higher than fathers in both the confidence and action subscales. Statistically significant differences were observed in the following areas: the confidence subscale for facilitating hearing access (Z=-2.33, P=0.02), the confidence subscale for supporting language development (Z=-3.40, P=0.001), and the action subscale for facilitating hearing access (Z=-1.88, P=0.05). The gender-based findings are compelling and suggest that mothers may perceive themselves as more confident and engaged in supporting their child’s auditory and language development.
Discussion
The coaching model, which fosters collaboration between professionals and parents, is central to early intervention for D/HH children from birth to age three. The ultimate aim is to empower parents and caregivers with the knowledge and confidence to independently implement their children’s individualized program goals without ongoing professional involvement. Parents participating in early intervention exhibit varying levels of beliefs and self-efficacy concerning their children’s hearing loss [5]. By thoroughly understanding parents’ strengths and identifying areas where they seek guidance, professionals can better support parents in achieving these goals.
The SPISE-R serves as a valuable tool for identifying parents’ capacities in terms of their beliefs, knowledge, and confidence in supporting a child with hearing loss. It provides insights that allow for tailored counseling, training, and guidance during early intervention. Given its usefulness, translating the SPISE-R into Persian was imperative to extend its applicability to Persian-speaking populations.
The Persian version demonstrated strong cultural compatibility across all five sections (CVR=0.77–1) and was highly comprehensible to families (S-FVI=0.94). Unlike the English [5] and Korean [14] versions, which have not published their content and face validity metrics, the Persian version provides these values, enhancing transparency and replicability. Additionally, the Persian version exhibited acceptable reliability, with no significant differences between test and re-test results, consistent with findings from the original and Korean versions.
Grounded in social learning theory, parental self-efficacy refers to parents’ beliefs in their ability to fulfil parenting tasks [15, 4]. Previous research demonstrates a strong association between parents’ task-specific self-efficacy and child language outcomes in children with hearing loss [3]. Higher confidence levels are linked to greater engagement in actions [5]. Consequently, parents play a pivotal role in enabling their child’s hearing access and fostering language development.
In terms of gender effects, we found no significant differences based on whether the father or mother completed the questionnaire. However, mothers scored higher than fathers in the confidence and action subscales. These differences were statistically significant for the confidence subscale in facilitating hearing access (Z=-2.33, P=0.02) and language development (Z=-3.40, P=0.001), as well as for the action subscale in facilitating hearing access (Z=-1.88, P=0.05). These findings may reflect greater maternal involvement, as mothers were predominantly unemployed and had more available time compared with fathers, and intervention programs may benefit from actively engaging fathers and addressing potential barriers to their involvement. Another study reported higher self-efficacy among mothers in managing their child’s hearing loss [16]. These results underscore the need to assess the unique strengths and needs of both parents when designing early intervention programs.
Parents’ beliefs about hearing loss significantly influence their self-efficacy and engagement in early intervention programs. Several factors, including gender, education level, and occupation, can shape these beliefs and their participation [4]. Additionally, child-specific factors, such as the age of hearing loss diagnosis, the timing of early intervention, the type of hearing devices, and the presence of comorbidities, may impact parents’ self-efficacy and involvement. Future research should explore how the SPISE-R can be utilized to assess these variables, thereby further refining early intervention strategies. The Persian version of the SPISE-R, like its English [5] and Korean [14] counterparts, is a valid and reliable tool.
Insights derived from the questionnaire can effectively highlight both parents’ resources and areas requiring additional support. The SPISE-R will be valuable in identifying families of children with hearing loss who may benefit from further counselling, education, and training to better support their child’s development. To enhance its clinical utility, future studies should focus on developing detailed implementation guidelines for its use in practice.
Conclusion
The validated Persian SPISE-R offers clinicians and researchers a culturally appropriate tool (CVR=0.77–1, S-FVI=0.94) to assess and support parental engagement in early intervention. Future work should focus on implementation protocols and longitudinal studies to evaluate its impact on child outcomes.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Research Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.REC.1400.492) on 29 August 2021. The participants received written and oral information about the study and provided consent to participate.
Funding
This study is part of a research plan accepted by the School of Rehabilitation Sciences at Iran University of Medical Sciences (Grant No.: 19626).
Authors' contributions
Methodology, formal analysis, and supervision: Shohreh Jalaie; Literature review: Zahra Validabadi, Maedeh Radayi; Investigation and data collection: Samaneh Tourani; Data curation, validation, and conceptual equivalence assessment: Shahrbanoo Ghaharri; Instrument validation and English questionnaire editing: Jean L. DesJardin; Writing: Anis Hosseini, Shohreh Jalaie and Mahsa Morsali; Translation: Anis Hosseini, Zahra Validabadi, Samin Moradi, and Sahand Rahimipour.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank all the participants in the study. Special thanks to Zhila Afsharmanesh, Majid Karimi, Soheila Shayanmehr and Afsaneh Alinejad. They would also like to show their gratitude toward the Cochlear Implant Center in Kerman City and the Cochlear Implant Center in Ahvaz City for their referrals.
References
- Fitzpatrick EM, Durieux-Smith A, Gaboury I, Coyle D, Whittingham J. Communication Development in Early-Identified Children With Mild Bilateral and Unilateral Hearing Loss. Am J Audiol. 2015; 24(3):349-53. [DOI:10.1044/2015_aja-15-0003] [PMID]
- Nazzi T, Nishibayashi LL, Berdasco-Muñoz E, Baud O, Biran V, Gonzalez-Gomez N. [Language acquisition in preterm infants during the first year of life (French)]. Arch Pediatr. 2015; 22(10):1072-7. [DOI:10.1016/j.arcped.2015.07.002] [PMID]
- Desjardin JL. Empowering families of children with cochlear implants: Implications for early intervention and language development. In: Eisenberg LS, editor. Clinical management of children with cochlear implants. San Diego: Plural Publishing Inc; 2009. [Link]
- Wittkowski A, Garrett C, Calam R, Weisberg D. Self-report measures of parental self-efficacy: A systematic review of the current literature. J Child Fam Stud. 2017; 26(11):2960-78. [DOI:10.1007/s10826-017-0830-5] [PMID]
- Ambrose SE, Appenzeller M, Mai A, DesJardin JL. Beliefs and self-efficacy of parents of young children with hearing loss. J Early Hear Detect Interv. 2020; 5(1):73. [DOI:10.26077/kkkh-vj55]
- Guimond AB, Wilcox MJ, Lamorey SG. The early intervention parenting self-efficacy scale (EIPSES) scale construction and initial psychometric evidence. J Early Interve. 2008; 30(4):295-320. [DOI:10.1177/1053815108320814]
- Desjardin JL. Maternal perceptions of self-efficacy and involvement in the auditory development of young children with prelingual deafness. J Early Interv. 2005; 27(3):193-209. [DOI:10.1177/105381510502700306]
- Salmani M, Asadi M, Tohidast SA, Shekariyan T, Shah Hoseyni F. A new Persian version of language assessment, remediation, and screening procedure (P-LARSP). Iran Rehab J. 2023; 20(4):517-28. [Link]
- Oryadi-Zanjani MM, Vahab M. Lexical effects on spoken word recognition in children with hearing impairment: Test-retest reliability of the Persian lexical neighborhood tests. JRSR. 2021;8(4):169-175. [DOI: 10.30476/jrsr.2021.92117.1201]
- Noori F, Ameri H, Noorian S, Aghagolzadeh F, Dabir Moghaddam M. [Story grammar assessment in Persian narrative discourse test (Persian)]. Adv Cogn Sci 2023; 25 (1) :123-136. [DOI: 10.30514/icss.25.1.123]
- Mohamadi R, Ahmadi A, Kazemi MD, Minaei A, Damarchi Z. Development of the Persian syntax comprehension test. Int J Pediatr Otorhinolaryngol. 2019; 124:22-29. [DOI:10.1016/j.ijporl.2019.05.032] [PMID]
- Joulaie M, Zamiri Abdollahi F, Darouie A, Ahmadi T, Desjardin J. Maternal perception of self-efficacy and involvement in young children with prelingual hearing loss. Indian J Otolaryngol Head Neck Surg. 2019; 71(1):48-53. [DOI:10.1007/s12070-018-1520-3] [PMID]
- Aaronson NK, Acquadro C, Alonso J, Apolone G, Bucquet D, Bullinger M, et al. International quality of life assessment (IQOLA) Project. Qual Life Res. 1992; 1(5):349-51. [DOI:10.1007/BF00434949] [PMID]
- Jung J, Jeon EK, Kim-Lee Y, Pae S. Parental self-efficacy and involvement in early intervention for young children with hearing loss. Commun Sci Dis. 2023; 28(2):354-71. [DOI:10.12963/csd.23955]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Advances in Behaviour Research and Therapy. 1978;1(4):139-161. https://doi.org/10.1016/0146-6402(78)90002-4
- Zaidman-Zait A, Most T, Tarrasch R, Haddad-eid E, Brand D. The impact of childhood hearing loss on the family: Mothers' and fathers' stress and coping resources. J Deaf Stud Deaf Educ. 2016; 21(1):23-33. [DOI:10.1093/deafed/env038] [PMID]
دانشکده علوم توانبخشی
گروه شنواییشناسی
مقیاس میزان مشارکت و خودکارآمدی والدین-1401
(SPISE-R)-2020
گروه شنواییشناسی
مقیاس میزان مشارکت و خودکارآمدی والدین-1401
(SPISE-R)-2020
دستورالعمل: در پاسخ به هر سوال دور شماره مورد نظرتان (از یک تا هفت را که احتمال بیشتر میدهید)، دایره بکشید.
الف) باورها
سوالات زیر مواردی هستندکه برخی از والدین کودکان کمشنوا ممکن است به آن اعتقاد، یا نگرانیهایی درباره آن داشته باشند. لطفاً مشخص کنید که چقدر به این موارد اعتقاد و باور دارید.
ب) اطلاعات:
هنگامی که والدین، دارای فرزند کمشنوا میشوند؛ باید اطلاعات و مهارتهای جدید بسیاری را بیاموزند و این فرایندی زمان بر است. میخواهیم بدانیم که شما در حال حاضر درباره هر یک از موضوعات زیر چقدر آگاه هستید و اطلاعات دارید.
ج) اطمینان:
داشتن اطلاعات به تنهایی همیشه ما را در انجام کاری مطمئن و آسوده نمیکند. ممکن است برای ایجاد اطمینان و اعتماد به خود، به زمان یا تمرین بیشتری نیاز داشته باشیم. لطفاً مشخص کنید که چقدر نسبت به توانایی خود در انجام هر یک از کارهای زیر اطمینان دارید.
د) اقدامات :
میدانیم که در طی روز مشغلههای زیادی داریم. والدین مسئولیتهای بسیاری دارند. از این رو ممکن است نتوانیم همه کارهایی را که دوست داریم، هرروز انجام دهیم. می خواهیم بدانیم با در نظر گرفتن همه مسئولیت های دیگری که دارید، شما چه میزان قادر به انجام فعالیت های زیر هستید؟
ه) استفاده از "سمعک یا کاشت حلزون":
میخواهیم بدانیم فرزند شما روزانه در هنگام بیداری به طور معمول چقدر از «سمعک یا کاشت حلزون" خود استفاده میکند. اگر کودک شما در یک گوش سمعک و در گوش دیگر کاشت حلزون دارد و در میزان استفاده از آنها تفاوتی وجود دارد، لطفاً برای هر دستگاه به طور جداگانه پاسخ دهید. (در صورت نیاز در جدول از کلمه های «کاشت حلزون» و»سمعک» استفاده کنید.)
1. فرزندتان در طی شبانهروز معمولا چند ساعت بیدار است ؟ ---------------
2. فرزندتان هنگامی که بیدار است، معمولا چند ساعت از سمعک یا کاشت حلزون خود استفاده میکند؟ ---------------
3. اگر فرزندتان تا به حال با سمعک یا کاشت حلزون روشن روی گوشش خوابیده است، لطفا مشخص کنید به طور معمول چند ساعت در شبانه روز این اتفاق میافتد؟ ---------------
4. هنگامی که فرزندتان در موقعیتهای زیر بیدار است، چقدر از سمعک یا کاشت حلزون خود استفاده میکند؟
مشخصات پاسخ دهنده به سوالات پرسشنامه
والدین: پدر مادر
سن والد: ..........
وضعیت شنوایی والد: شنوا کم شنوا ناشنوا
سطح تحصیلات والد: ابتدایی دیپلم لیسانس فوق لیسانس دکترا
وضعیت شغلی والد: شاغل غیرشاغل
تعداد فرزند کم شنوا در خانواده: یکی دو تا سه تا
سن کودک (به سال): ..........
جنسیت کودک: دختر پسر
سن تشخیص کم شنوایی: 12 ماهگی یا قبل بعد از 12 ماهگی
میزان کم شنوایی گوش بهتر (براساس آزمایش شنوایی بدون وسیله تقویت کننده):
ملایم تا متوسط (مسطح یا با شیب ملایم در فرکانسهای بالا)
متوسط تا شدید
شدید
عمیق
میزان کم شنوایی گوش بهتر (براساس آزمایش شنوایی با استفاده از وسیله تقویت کننده):
جزئی (نزدیک به محدوده طبیعی) ملایم متوسط متوسط شدید شدید عمیق
نوع روش ارتباطی: شنیداری-کلامی شفاهی (گفتاری و لبخوانی)
ارتباط کلی (گفتاری، لبخوانی و زبان اشاره) زبان اشاره و لبخوانی
وجود مشکلات دیگر علاوه بر کم شنوایی (درصورت پاسخ بلی، نوع آن نوشته شود): بلی خیر
توضیح: ..........
نوع وسیله کمک شنوایی (در حال حاضر): سمعک دو گوشی سمعک یک گوشی (گوش بهتر یا بدتر)
کاشت حلزون یکطرفه کاشت حلزون دوطرفه
در چه سنی (برحسب ماه)، کم شنوایی توسط متخصصین تایید شد؟ ..........
در چه سنی (برحسب ماه)، سمعک دریافت و استفاده شد؟ ..........
در چه سنی (برحسب ماه)، دستگاه کاشت حلزون دریافت و استفاده شد؟ ..........
Type of Study: Research |
Subject:
Audiology
Received: 2025/08/1 | Accepted: 2025/12/22 | Published: 2026/03/11
Received: 2025/08/1 | Accepted: 2025/12/22 | Published: 2026/03/11
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.