

Volume 8, Issue 1 (Continuously Updated 2025)
Func Disabil J 2025, 8(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Obaigwa E O, Govender P. Rehabilitation of Individuals With Spinal Cord Injuries in Kenya: Occupational Therapists’ Perspectives on Community (Re)Integration. Func Disabil J 2025; 8 (1)
URL: http://fdj.iums.ac.ir/article-1-321-en.html
URL: http://fdj.iums.ac.ir/article-1-321-en.html



1- Department of Occupational Therapy, Kenyatta National Hospital, Nairobi, Kenya.
2- Department of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. ,naidoopg@ukzn.ac.za
2- Department of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. ,
Keywords: Spinal cord injuries (SCI), Occupational therapist, Service delivery, Community integration, Rehabilitation
Full-Text [PDF 851 kb]
(54 Downloads)
| Abstract (HTML) (166 Views)
Full-Text: (44 Views)
Introduction
The World Health Organization (WHO) identifies participation in community and social life as a fundamental human right. According to the international classification of functioning, disability and health, participation is defined as an individual’s involvement in life situations [1]. The rehabilitation literature increasingly emphasizes social and community participation because of its strong association with quality of life, health outcomes, and psychological well-being. In addition, evidence from studies on individuals with spinal cord injuries (SCIs) demonstrates that participation in community activities fosters motivation, competence, and self-efficacy while also reducing depressive symptoms [1-3]. Despite these proven benefits, individuals with SCIs continue to experience reduced levels of participation. On the other hand, the prescribed assistive devices to support mobility and access alone do not guarantee optimal community reintegration (CR). The CR process dictates restoring or enhancing an individual’s ability to resume meaningful roles and fully participate in social, cultural, and community life following SCIs. It further includes overcoming environmental and social barriers to enable autonomy, inclusion, and improved quality of life [1-3].
In Kenya, people with SCIs constitute 3.5% of those with disabilities who face unique challenges to CR, including limited rehabilitation resources, environmental barriers, and societal attitudes toward disability. Though occupational therapists (OTs) play a critical role in supporting this process by facilitating participation, addressing barriers, and promoting independence in community contexts, their numbers are below the WHO threshold for each given population [4-7]. However, little is known about the lived experiences of OTs working in this area. Accordingly, understanding their perspectives is essential to inform policies, practices, and training aimed at improving CR outcomes for individuals with SCIs in Kenya.
Materials and Methods
Research team and reflexivity
The principal investigator was the first author, an OT with experience in SCI rehabilitation. The interviewer’s professional background and interest in SCI rehabilitation were disclosed to participants to establish rapport and credibility. It should be noted that the interviewer had no prior professional relationships with the participants. Participants were recruited through professional networks and institutional contacts, ensuring a lack of power dynamics that could influence responses. The research team received formal training on qualitative research methods. In addition, the first author served as the primary interviewer and maintained reflexivity throughout the data collection process through bracketing [8].
Study design and sampling
This study employed an explorative qualitative approach [8], allowing participants to share their lived experiences with individuals with SCIs and their concerns about service delivery [8].
Purposive sampling was utilized to recruit participants with specific experience in SCI rehabilitation. Potential participants were approached through professional occupational therapy networks and institutional contacts in Nairobi. A total of 14 Nairobi-based OTs were recruited who met the criteria of being practising OTs with over two years of experience working with patients with SCIs.
Setting and data collection
This study was performed in Nairobi, Kenya, targeting OTs working in hospital and community settings with experience in SCI rehabilitation. The interviews were conducted in neutral environments to promote confidentiality and participant comfort. Only the principal author was present during data collection sessions. Two focus group discussions (FGDs) with six OTs, each representing a different institution, and two individual in-depth interviews were conducted to gather comprehensive insights into the research topic. A semi-structured interview and focus group discussion (FGD) guide, which covered perceptions on SCIs, prevalence, OT roles, barriers, facilitators, improvement strategies, and participants’ final additional contributions, was developed, including predetermined short, open-ended, and non-threatening questions [8]. The questions elicited responses reflecting participants’ insights and experiences working with individuals with SCIs [8]. Additional probes examined institutional support for the CR of individuals with SCIs [8, 9]. No repeat interviews were conducted, as data redundancy was achieved within the planned data collection sessions. It is noteworthy that all sessions were audio-recorded with the participant’s consent. Strategies to obtain approval for recording included establishing rapport and assuring complete confidentiality [8, 9]. In addition, handwritten notes were taken during sessions, capturing participants’ nonverbal expressions and contextual information. Each individual and focus group session lasted approximately 90 minutes. Transcripts were not returned to participants for comments or corrections due to logistical constraints, but member checking was employed during the analysis phase.
Data Analysis
Two researchers were involved in the coding process to enhance reliability while reducing bias. The initial codes represented key emerging themes related to study objectives. The codes were expanded after reading all transcripts, with conceptual and substantive categories generated using NVivo’s “tree nodes” structure. Themes were inductively derived from the data through content analysis [8]. The framework included coding criteria, key findings, quotes, definitions, and other interview outcomes. QSR NVivo software, version 10 was used to systematically organize and process qualitative data. Furthermore, member checking was conducted to control researcher bias and ensure data authenticity. Study participants were involved in testing the reality of collected data and study processes [8].
Trustworthiness and rigour
Multiple strategies were employed, including rigorous data collection, peer debriefing with supervisors, and member checking with participants [8]. A detailed description of the research context, participant characteristics, and findings enables readers to assess transferability to similar settings. Consistency and traceability were ensured through detailed audit trails, comprehensive record-keeping, and collaborative data analysis [8]. Moreover, the principle of bracketing was maintained throughout data collection and analysis to distinguish between participants’ perspectives and the researcher’s assumptions. Eventually, methodological triangulation was achieved through multiple data collection methods (focus groups and individual interviews) to enhance the validity of findings [8].
Results
Table 1 presents a profile of the 14 participants who contributed to the study.
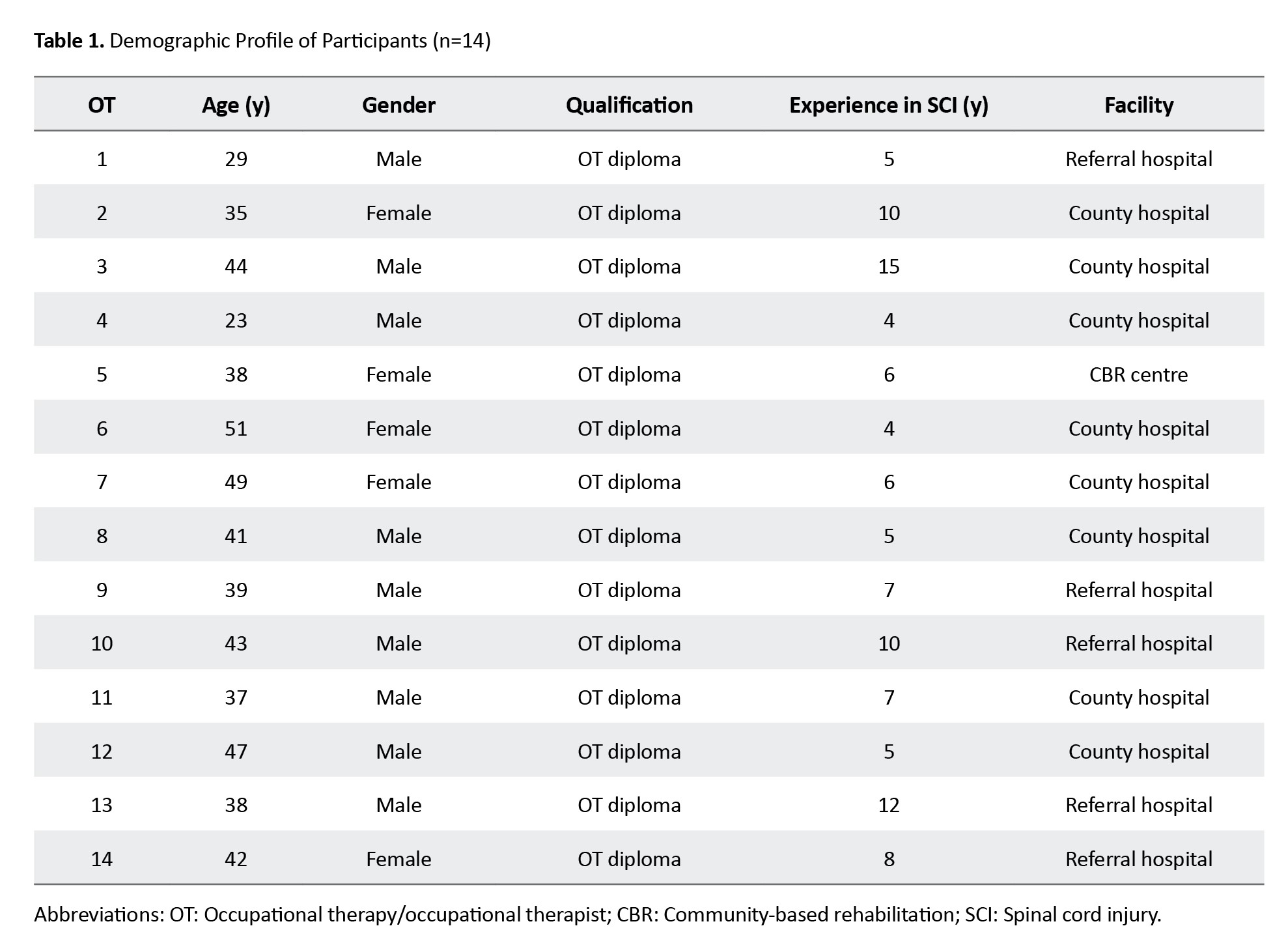
Of this number, 11 held a diploma qualification, and three held a degree qualification. The overall theme encompassed the lived experiences of OTs in addressing the needs of individuals with SCIs. The information was organized into three subthemes (Figure 1) and described with a narrative augmented by verbatim quotes.

Theme 1: The typical delivery of CR interventions for SCIs
The findings demonstrated that discrepancies and a lack of structure in occupational therapy service delivery in SCIs resulted in inconsistent interventions. Even with these discrepancies, participants noted their commitment to collaborative interventions, including a comprehensive ward program, helping them return to the highest possible level of function and independence.
“We share our intervention process with the other multidisciplinary team.” (OT2, focus group 2)
“We have days for ward rounds that we have to attend and share our intervention process with the other multidisciplinary team; there are those days we receive outpatients’ clients to continue therapy, and those for outdoor activities. There are other days that I have students” (OT3, focus group 1).
Theme 2: Challenges in spinal cord injury service delivery
The results revealed several barriers to facilitating CR. The participants identified that enabling CR was difficult, particularly for individuals from poor households.
“Some of these individuals used to be hustlers…who will accept them, so it is difficult...” (OT4. focus group 1).
“Our community is poor; now adding the burden of an individual, they are adding another burden. You find it difficult to support. We have experience where you find that because of prolonged stays in the hospital, people with SCI properties get lost, and you fail to get to where to take these individuals. Some of these individuals used to be hustlers; now imagine who this landlord is to accept them; therefore, it is difficult...” (OT6, focus group 2).
Societal attitudes: Society believes they should help and “feel they have a duty to help,” rather than encouraging independent living, complicating the CR processes.
Insurance coverage: The discrepancies in medical insurance coverage that “do not cover most services” affect efforts to provide services. For instance, some insurance companies decline to provide outpatient services and mobility aids (e.g. wheelchairs), hindering CR after SCIs.
Training and Knowledge Gaps: Lack of knowledge and skills from college training and inadequate orientation hinder goal achievement. For example, a specialization in areas of SCIs
OT11 indicated
“If it is training, this is where it should start; our hospitals should embark on the frequent updating of skills in this area. The knowledge we receive in college is fundamental, and yet, this is a specialized area.”
Organizational barriers: The commitment of concerned organizations, including the need to address inadequate space, lack of supplies, late referrals, poor discharge protocols, and insufficient resources to perform home assessment and modification before discharge, hinders the facilitation of CR of people with SCIs.
“Lack of supplies prevents me from using my intervention of choice as per my assessment” (OT 2, focus group 2).
Professional recognition: Though OTs’ role in the rehabilitation process is significant, the lack of support undermines their contributions. In addition, their roles are poorly understood; most people, including fellow healthcare workers, suppose that OT is physiotherapy, resulting in incorrect referrals.
“The OT role in rehabilitation is vital; there are few. I wish the governments could do something” (OT12, focus group 2).
Infrastructure limitations: There are few SCI-specialized hospitals, while other general health facilities lack resources and have no special wards or spaces for SCIs. In addition, there is a lack of simplified manuals or guidelines for the handling or management of SCIs, and OTs’ reluctance to work in the community impedes efforts to facilitate the CR of people with SCIs.
“These patients need to be handled as special, which is never guaranteed; they are considered ordinary patients. The toilets and washrooms were the same. There are no adjustable beds, and you cannot train for transfers. The wards are congested with very little space for the therapists to properly handle these clients without straining their backs” (OT3 focus group 1).
Theme 3: Enhancing the community reintegration of individuals with SCI
The participants in this study considered applicable processes to facilitate the CR of people with SCIs. They included using the Internet to access information and self-training through reading to compensate for the lack of skills and training in SCIs.
“This is self-taught experience; I have learned through the Internet how to handle intimate matters because, based on my experience, this is a pertinent issue to handle before patients are released to the community” (OT9, focus group 2).
Therapeutic Relationships: Establishing or creating an acceptable therapist-client relationship during intervention enables the CR process to be successful.
Peer Support: Remarkably, the use of individuals who have already adjusted to the community and trained motivational speakers strategically facilitates CR among those individuals. This can also be reinforced by working as a team, in addition to “sharing progress on specific clients” and sharing experiences on handling complex issues of their clients with SCIs.
“Through support groups and post-SCI individuals are trained as counsellors, we have specific days we allow them to interact and answer their questions; we have seen that this way works” (OT13, individual interview).
Support groups and education: SCI support groups and education encourage these individuals to attend short counselling courses, where unique and sensitive issues can be adequately addressed. In addition, education can be provided to family members on SCI care at home.
“Education has to involve family members to prevent future complications related to incontinence. Involving family members is very helpful” (OT7, focus group 2).
Stakeholder Collaboration: Prioritizing the transition process from key stakeholders, such as relevant government divisions, non-governmental organizations (NGOs), and local groups, can reduce delays in the discharge process, which, in turn, will make the CR process easier to achieve.
“Minimal support is provided; managing SCIs requires collaborative efforts. Despite the help of the government, even if they were to offer comprehensive support, NGOs and religious organizations should collaborate in this regard” (OT5, focus group 1).
Institutional support: Institutions should ensure the availability of specialized SCI units, well-trained OTs supported by mentorship programs, and well-equipped OT departments. It was further established that raising awareness in the community on SCIs to alleviate negative attitudes in the community is crucial because such attitudes “demotivate these patients,” affecting the CR process.
Financial and Policy Support: Increasing funding for people with disabilities, including individuals with SCIs, while making this funding easily accessible, will enable CR. Likewise, our findings indicated that it would be prudent for the government to make it possible and mandatory for employers to support their employees returning to work after SCIs, including by making their working environment conducive and ensuring comprehensive medical cover to support them in continuing their rehabilitation.
Advocacy and Benchmarking: Most importantly, advocacy initiatives, benchmarking with developed or neighbouring countries on managing SCIs, and collaboration among all relevant institutions, in addition to exchange programs, research, and scholarships for SCI students or staff, enable OTs to successfully participate in CR.
Discussion
The results of this study revealed that while OTs are committed to multidisciplinary collaboration, service delivery remains inconsistent and is hindered by socioeconomic, organizational, infrastructural, and training challenges. Limited insurance coverage, poor recognition of OT roles, and negative societal attitudes restrict reintegration. Strengthening peer support, family education, stakeholder collaboration, institutional capacity, and policy advocacy were identified as key strategies to enhance successful CR.
Baradaran-Seyed et al. reported the complexities of CR for individuals with SCIs, where systemic barriers (e.g. lack of structured guidelines, limited resources, and weak institutional frameworks) undermine the development and implementation of best practices in developing countries [10]. Similarly, OTs in this study described inconsistent service delivery, poor discharge protocols, and inadequate infrastructure, reflecting how health system gaps directly hinder effective CR.
While other studies have demonstrated that collaborative, multi-site quality improvement initiatives can strengthen SCI care [11], Kenyan OTs emphasized their commitment to multidisciplinary collaboration. However, they also noted challenges, including under-recognition of their roles, limited insurance coverage, and limited organizational support, constraining the impact of collaborative practices in low-resource settings.
Finally, Barclay et al. found that both facilitators (e.g. peer support and community engagement) and barriers (e.g. social attitudes and lack of resources) strongly influence participation after SCIs [12], which aligns with Kenyan OTs’ accounts of society’s dual role. On the one hand, negative attitudes and poverty impede reintegration; on the other hand, peer support, family education, and community awareness emerge as powerful enablers.
Overall, these studies reinforce that a combination of systemic, organizational, and social factors shapes OTs’ experiences when facilitating CR. Addressing these barriers while strengthening collaborative networks, policy frameworks, and community-based supports is essential to improve reintegration outcomes for individuals with SCIs [11-15].
Culture is a collection of beliefs, attitudes, and value systems that are internalized throughout life and influence an individual’s behaviour. Consequently, OTs find it challenging to address intimacy, sexuality, and bowel and bladder management in people with SCIs as a result of cultural sensitivity [14, 15]. Although sexual needs are a right for individuals with SCIs, this study found that addressing intimacy and sexuality is viewed as culturally sensitive, likely due to inadequate training and skills, compounded by internalized cultural beliefs. However, OTs must adapt their practice and enhance competency in addressing these needs despite cultural sensitivities [16-18].
The treatment and rehabilitation of SCI are expensive and exhausting. Early access to specialized care and rehabilitation should address the prevention of joint contractures, loss of muscle strength, maintenance of bone density, optimal functioning of the respiratory and digestive systems, and improvement of CR [19, 20]. Although it was found that the rehabilitation process is essential, few OTs whose role is not well understood, thus delaying referrals. Consequently, Obaigwa et al. suggested that professional bodies and the Ministry should promote OTs’ value, knowledge, and skills, and encourage collaborative multidisciplinary practices [21].
Complex barriers (e.g. inadequate workspace, insufficient supplies, inadequate guidelines for managing persons with SCI, and/or poor discharge protocols) complicate optimal rehabilitation. Conversely, Upton et al. demonstrated that OTs hold positive attitudes toward evidence-based practice. However, these attitudes do not translate into practice due to several barriers, such as limited time, the availability and accessibility of research, and limited research skills [22]. Therefore, educational and training initiatives must provide therapists with the tools and support they need to fully engage with research evidence and its application in clinical care. Emerich et al. also reported that enhancing therapists’ skills and developing expertise greatly improve the treatment of individuals with SCI and enhance competency in preparing patients for discharge to home, teaching them to become advocates, and preparing them for social participation [23].
The participants further complained that only one SCI-specialized hospital serves the whole country. This hospital is overwhelmed by vast numbers of clients, resulting in premature discharge before SCI clients gain optimal independence to survive in the community. The findings of this study also revealed that support to facilitate the transition from hospital to the community was limited, particularly from the government and NGOs, implying that their clients lack support systems. Undeniably, WHO applauds the need for specialized rehabilitation for individuals suffering from SCI, but inadequate vocational rehabilitation, financial support, physical rehabilitation, and problems of access in the workplace hinder the integration of individuals with SCI into mainstream society [6, 24-27].
The participants suggested that the involvement of the government, religious organizations, learning institutions, and other support groups is necessary to comprehensively address the needs of people with SCI. The WHO adopted the Alma-Ata Declaration in 1978 to strengthen community-based rehabilitation and involve all stakeholders to ensure successful community participation. The government institution is supposed to be the steering leader. The participants further recommended that the government not only involve OTs and individuals with SCI in decision-making but also establish mechanisms to ensure fund accessibility and employers’ facilitation of a successful return to work, thereby making the working environment conducive for people with SCI. Other initiatives recommended in this regard include benchmarking, exchange programs, research, and scholarships for SCI students or staff, and the establishment of SCI-specialized hospitals by regional governments nationwide. Similarly, other studies reported that collective decision-making strengthens the community [25-30].
Strengths and limitations
The participants’ views in this study did not reflect the perceptions of OTs nationwide. However, the findings provide a strong foundation in addressing the professions’ discrepancies, enabling people with SCIs to achieve CR.
Conclusion
This study provides strong evidence that collaborative efforts among training institutions, local and national governments, professional bodies, and individual OTs are needed to enhance skills and create an environment that supports holistic approaches to fully integrate individuals with SCI into their communities. However, further research is recommended to merge the experience of OTs in developing interventional tools meant for facilitating CR for people with SCIs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Nairobi, Nairobi, Kenya and the University of KwaZulu-Natal Biomedical, Durban, South Africa (Code: BE070/18). Moreover, written informed consent was obtained from all participants prior to data collection. Additionally, all the principles of research ethics were strictly observed, including confidentiality, anonymity, and voluntary participation.
Funding
This paper was extracted from doctoral thesis of Evans Obara Obaigwa, approved by University of KwaZulu-Natal Biomedical, Durban, South Africa.
Authors' contributions
Data collection, investigation, project administration, resources, validation and software: Evans Obara Obaigwa; Supervision: Pragashnie Govender; Conceptualization, writing the original draft, review, editing, formal analysis, funding acquisition, methodology and visualization: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors acknowledge the support and assistance of the Kenyan OTs who participated in this study and Kitty Uys for her mentorship on this project.
References
The World Health Organization (WHO) identifies participation in community and social life as a fundamental human right. According to the international classification of functioning, disability and health, participation is defined as an individual’s involvement in life situations [1]. The rehabilitation literature increasingly emphasizes social and community participation because of its strong association with quality of life, health outcomes, and psychological well-being. In addition, evidence from studies on individuals with spinal cord injuries (SCIs) demonstrates that participation in community activities fosters motivation, competence, and self-efficacy while also reducing depressive symptoms [1-3]. Despite these proven benefits, individuals with SCIs continue to experience reduced levels of participation. On the other hand, the prescribed assistive devices to support mobility and access alone do not guarantee optimal community reintegration (CR). The CR process dictates restoring or enhancing an individual’s ability to resume meaningful roles and fully participate in social, cultural, and community life following SCIs. It further includes overcoming environmental and social barriers to enable autonomy, inclusion, and improved quality of life [1-3].
In Kenya, people with SCIs constitute 3.5% of those with disabilities who face unique challenges to CR, including limited rehabilitation resources, environmental barriers, and societal attitudes toward disability. Though occupational therapists (OTs) play a critical role in supporting this process by facilitating participation, addressing barriers, and promoting independence in community contexts, their numbers are below the WHO threshold for each given population [4-7]. However, little is known about the lived experiences of OTs working in this area. Accordingly, understanding their perspectives is essential to inform policies, practices, and training aimed at improving CR outcomes for individuals with SCIs in Kenya.
Materials and Methods
Research team and reflexivity
The principal investigator was the first author, an OT with experience in SCI rehabilitation. The interviewer’s professional background and interest in SCI rehabilitation were disclosed to participants to establish rapport and credibility. It should be noted that the interviewer had no prior professional relationships with the participants. Participants were recruited through professional networks and institutional contacts, ensuring a lack of power dynamics that could influence responses. The research team received formal training on qualitative research methods. In addition, the first author served as the primary interviewer and maintained reflexivity throughout the data collection process through bracketing [8].
Study design and sampling
This study employed an explorative qualitative approach [8], allowing participants to share their lived experiences with individuals with SCIs and their concerns about service delivery [8].
Purposive sampling was utilized to recruit participants with specific experience in SCI rehabilitation. Potential participants were approached through professional occupational therapy networks and institutional contacts in Nairobi. A total of 14 Nairobi-based OTs were recruited who met the criteria of being practising OTs with over two years of experience working with patients with SCIs.
Setting and data collection
This study was performed in Nairobi, Kenya, targeting OTs working in hospital and community settings with experience in SCI rehabilitation. The interviews were conducted in neutral environments to promote confidentiality and participant comfort. Only the principal author was present during data collection sessions. Two focus group discussions (FGDs) with six OTs, each representing a different institution, and two individual in-depth interviews were conducted to gather comprehensive insights into the research topic. A semi-structured interview and focus group discussion (FGD) guide, which covered perceptions on SCIs, prevalence, OT roles, barriers, facilitators, improvement strategies, and participants’ final additional contributions, was developed, including predetermined short, open-ended, and non-threatening questions [8]. The questions elicited responses reflecting participants’ insights and experiences working with individuals with SCIs [8]. Additional probes examined institutional support for the CR of individuals with SCIs [8, 9]. No repeat interviews were conducted, as data redundancy was achieved within the planned data collection sessions. It is noteworthy that all sessions were audio-recorded with the participant’s consent. Strategies to obtain approval for recording included establishing rapport and assuring complete confidentiality [8, 9]. In addition, handwritten notes were taken during sessions, capturing participants’ nonverbal expressions and contextual information. Each individual and focus group session lasted approximately 90 minutes. Transcripts were not returned to participants for comments or corrections due to logistical constraints, but member checking was employed during the analysis phase.
Data Analysis
Two researchers were involved in the coding process to enhance reliability while reducing bias. The initial codes represented key emerging themes related to study objectives. The codes were expanded after reading all transcripts, with conceptual and substantive categories generated using NVivo’s “tree nodes” structure. Themes were inductively derived from the data through content analysis [8]. The framework included coding criteria, key findings, quotes, definitions, and other interview outcomes. QSR NVivo software, version 10 was used to systematically organize and process qualitative data. Furthermore, member checking was conducted to control researcher bias and ensure data authenticity. Study participants were involved in testing the reality of collected data and study processes [8].
Trustworthiness and rigour
Multiple strategies were employed, including rigorous data collection, peer debriefing with supervisors, and member checking with participants [8]. A detailed description of the research context, participant characteristics, and findings enables readers to assess transferability to similar settings. Consistency and traceability were ensured through detailed audit trails, comprehensive record-keeping, and collaborative data analysis [8]. Moreover, the principle of bracketing was maintained throughout data collection and analysis to distinguish between participants’ perspectives and the researcher’s assumptions. Eventually, methodological triangulation was achieved through multiple data collection methods (focus groups and individual interviews) to enhance the validity of findings [8].
Results
Table 1 presents a profile of the 14 participants who contributed to the study.
Of this number, 11 held a diploma qualification, and three held a degree qualification. The overall theme encompassed the lived experiences of OTs in addressing the needs of individuals with SCIs. The information was organized into three subthemes (Figure 1) and described with a narrative augmented by verbatim quotes.
Theme 1: The typical delivery of CR interventions for SCIs
The findings demonstrated that discrepancies and a lack of structure in occupational therapy service delivery in SCIs resulted in inconsistent interventions. Even with these discrepancies, participants noted their commitment to collaborative interventions, including a comprehensive ward program, helping them return to the highest possible level of function and independence.
“We share our intervention process with the other multidisciplinary team.” (OT2, focus group 2)
“We have days for ward rounds that we have to attend and share our intervention process with the other multidisciplinary team; there are those days we receive outpatients’ clients to continue therapy, and those for outdoor activities. There are other days that I have students” (OT3, focus group 1).
Theme 2: Challenges in spinal cord injury service delivery
The results revealed several barriers to facilitating CR. The participants identified that enabling CR was difficult, particularly for individuals from poor households.
“Some of these individuals used to be hustlers…who will accept them, so it is difficult...” (OT4. focus group 1).
“Our community is poor; now adding the burden of an individual, they are adding another burden. You find it difficult to support. We have experience where you find that because of prolonged stays in the hospital, people with SCI properties get lost, and you fail to get to where to take these individuals. Some of these individuals used to be hustlers; now imagine who this landlord is to accept them; therefore, it is difficult...” (OT6, focus group 2).
Societal attitudes: Society believes they should help and “feel they have a duty to help,” rather than encouraging independent living, complicating the CR processes.
Insurance coverage: The discrepancies in medical insurance coverage that “do not cover most services” affect efforts to provide services. For instance, some insurance companies decline to provide outpatient services and mobility aids (e.g. wheelchairs), hindering CR after SCIs.
Training and Knowledge Gaps: Lack of knowledge and skills from college training and inadequate orientation hinder goal achievement. For example, a specialization in areas of SCIs
OT11 indicated
“If it is training, this is where it should start; our hospitals should embark on the frequent updating of skills in this area. The knowledge we receive in college is fundamental, and yet, this is a specialized area.”
Organizational barriers: The commitment of concerned organizations, including the need to address inadequate space, lack of supplies, late referrals, poor discharge protocols, and insufficient resources to perform home assessment and modification before discharge, hinders the facilitation of CR of people with SCIs.
“Lack of supplies prevents me from using my intervention of choice as per my assessment” (OT 2, focus group 2).
Professional recognition: Though OTs’ role in the rehabilitation process is significant, the lack of support undermines their contributions. In addition, their roles are poorly understood; most people, including fellow healthcare workers, suppose that OT is physiotherapy, resulting in incorrect referrals.
“The OT role in rehabilitation is vital; there are few. I wish the governments could do something” (OT12, focus group 2).
Infrastructure limitations: There are few SCI-specialized hospitals, while other general health facilities lack resources and have no special wards or spaces for SCIs. In addition, there is a lack of simplified manuals or guidelines for the handling or management of SCIs, and OTs’ reluctance to work in the community impedes efforts to facilitate the CR of people with SCIs.
“These patients need to be handled as special, which is never guaranteed; they are considered ordinary patients. The toilets and washrooms were the same. There are no adjustable beds, and you cannot train for transfers. The wards are congested with very little space for the therapists to properly handle these clients without straining their backs” (OT3 focus group 1).
Theme 3: Enhancing the community reintegration of individuals with SCI
The participants in this study considered applicable processes to facilitate the CR of people with SCIs. They included using the Internet to access information and self-training through reading to compensate for the lack of skills and training in SCIs.
“This is self-taught experience; I have learned through the Internet how to handle intimate matters because, based on my experience, this is a pertinent issue to handle before patients are released to the community” (OT9, focus group 2).
Therapeutic Relationships: Establishing or creating an acceptable therapist-client relationship during intervention enables the CR process to be successful.
Peer Support: Remarkably, the use of individuals who have already adjusted to the community and trained motivational speakers strategically facilitates CR among those individuals. This can also be reinforced by working as a team, in addition to “sharing progress on specific clients” and sharing experiences on handling complex issues of their clients with SCIs.
“Through support groups and post-SCI individuals are trained as counsellors, we have specific days we allow them to interact and answer their questions; we have seen that this way works” (OT13, individual interview).
Support groups and education: SCI support groups and education encourage these individuals to attend short counselling courses, where unique and sensitive issues can be adequately addressed. In addition, education can be provided to family members on SCI care at home.
“Education has to involve family members to prevent future complications related to incontinence. Involving family members is very helpful” (OT7, focus group 2).
Stakeholder Collaboration: Prioritizing the transition process from key stakeholders, such as relevant government divisions, non-governmental organizations (NGOs), and local groups, can reduce delays in the discharge process, which, in turn, will make the CR process easier to achieve.
“Minimal support is provided; managing SCIs requires collaborative efforts. Despite the help of the government, even if they were to offer comprehensive support, NGOs and religious organizations should collaborate in this regard” (OT5, focus group 1).
Institutional support: Institutions should ensure the availability of specialized SCI units, well-trained OTs supported by mentorship programs, and well-equipped OT departments. It was further established that raising awareness in the community on SCIs to alleviate negative attitudes in the community is crucial because such attitudes “demotivate these patients,” affecting the CR process.
Financial and Policy Support: Increasing funding for people with disabilities, including individuals with SCIs, while making this funding easily accessible, will enable CR. Likewise, our findings indicated that it would be prudent for the government to make it possible and mandatory for employers to support their employees returning to work after SCIs, including by making their working environment conducive and ensuring comprehensive medical cover to support them in continuing their rehabilitation.
Advocacy and Benchmarking: Most importantly, advocacy initiatives, benchmarking with developed or neighbouring countries on managing SCIs, and collaboration among all relevant institutions, in addition to exchange programs, research, and scholarships for SCI students or staff, enable OTs to successfully participate in CR.
Discussion
The results of this study revealed that while OTs are committed to multidisciplinary collaboration, service delivery remains inconsistent and is hindered by socioeconomic, organizational, infrastructural, and training challenges. Limited insurance coverage, poor recognition of OT roles, and negative societal attitudes restrict reintegration. Strengthening peer support, family education, stakeholder collaboration, institutional capacity, and policy advocacy were identified as key strategies to enhance successful CR.
Baradaran-Seyed et al. reported the complexities of CR for individuals with SCIs, where systemic barriers (e.g. lack of structured guidelines, limited resources, and weak institutional frameworks) undermine the development and implementation of best practices in developing countries [10]. Similarly, OTs in this study described inconsistent service delivery, poor discharge protocols, and inadequate infrastructure, reflecting how health system gaps directly hinder effective CR.
While other studies have demonstrated that collaborative, multi-site quality improvement initiatives can strengthen SCI care [11], Kenyan OTs emphasized their commitment to multidisciplinary collaboration. However, they also noted challenges, including under-recognition of their roles, limited insurance coverage, and limited organizational support, constraining the impact of collaborative practices in low-resource settings.
Finally, Barclay et al. found that both facilitators (e.g. peer support and community engagement) and barriers (e.g. social attitudes and lack of resources) strongly influence participation after SCIs [12], which aligns with Kenyan OTs’ accounts of society’s dual role. On the one hand, negative attitudes and poverty impede reintegration; on the other hand, peer support, family education, and community awareness emerge as powerful enablers.
Overall, these studies reinforce that a combination of systemic, organizational, and social factors shapes OTs’ experiences when facilitating CR. Addressing these barriers while strengthening collaborative networks, policy frameworks, and community-based supports is essential to improve reintegration outcomes for individuals with SCIs [11-15].
Culture is a collection of beliefs, attitudes, and value systems that are internalized throughout life and influence an individual’s behaviour. Consequently, OTs find it challenging to address intimacy, sexuality, and bowel and bladder management in people with SCIs as a result of cultural sensitivity [14, 15]. Although sexual needs are a right for individuals with SCIs, this study found that addressing intimacy and sexuality is viewed as culturally sensitive, likely due to inadequate training and skills, compounded by internalized cultural beliefs. However, OTs must adapt their practice and enhance competency in addressing these needs despite cultural sensitivities [16-18].
The treatment and rehabilitation of SCI are expensive and exhausting. Early access to specialized care and rehabilitation should address the prevention of joint contractures, loss of muscle strength, maintenance of bone density, optimal functioning of the respiratory and digestive systems, and improvement of CR [19, 20]. Although it was found that the rehabilitation process is essential, few OTs whose role is not well understood, thus delaying referrals. Consequently, Obaigwa et al. suggested that professional bodies and the Ministry should promote OTs’ value, knowledge, and skills, and encourage collaborative multidisciplinary practices [21].
Complex barriers (e.g. inadequate workspace, insufficient supplies, inadequate guidelines for managing persons with SCI, and/or poor discharge protocols) complicate optimal rehabilitation. Conversely, Upton et al. demonstrated that OTs hold positive attitudes toward evidence-based practice. However, these attitudes do not translate into practice due to several barriers, such as limited time, the availability and accessibility of research, and limited research skills [22]. Therefore, educational and training initiatives must provide therapists with the tools and support they need to fully engage with research evidence and its application in clinical care. Emerich et al. also reported that enhancing therapists’ skills and developing expertise greatly improve the treatment of individuals with SCI and enhance competency in preparing patients for discharge to home, teaching them to become advocates, and preparing them for social participation [23].
The participants further complained that only one SCI-specialized hospital serves the whole country. This hospital is overwhelmed by vast numbers of clients, resulting in premature discharge before SCI clients gain optimal independence to survive in the community. The findings of this study also revealed that support to facilitate the transition from hospital to the community was limited, particularly from the government and NGOs, implying that their clients lack support systems. Undeniably, WHO applauds the need for specialized rehabilitation for individuals suffering from SCI, but inadequate vocational rehabilitation, financial support, physical rehabilitation, and problems of access in the workplace hinder the integration of individuals with SCI into mainstream society [6, 24-27].
The participants suggested that the involvement of the government, religious organizations, learning institutions, and other support groups is necessary to comprehensively address the needs of people with SCI. The WHO adopted the Alma-Ata Declaration in 1978 to strengthen community-based rehabilitation and involve all stakeholders to ensure successful community participation. The government institution is supposed to be the steering leader. The participants further recommended that the government not only involve OTs and individuals with SCI in decision-making but also establish mechanisms to ensure fund accessibility and employers’ facilitation of a successful return to work, thereby making the working environment conducive for people with SCI. Other initiatives recommended in this regard include benchmarking, exchange programs, research, and scholarships for SCI students or staff, and the establishment of SCI-specialized hospitals by regional governments nationwide. Similarly, other studies reported that collective decision-making strengthens the community [25-30].
Strengths and limitations
The participants’ views in this study did not reflect the perceptions of OTs nationwide. However, the findings provide a strong foundation in addressing the professions’ discrepancies, enabling people with SCIs to achieve CR.
Conclusion
This study provides strong evidence that collaborative efforts among training institutions, local and national governments, professional bodies, and individual OTs are needed to enhance skills and create an environment that supports holistic approaches to fully integrate individuals with SCI into their communities. However, further research is recommended to merge the experience of OTs in developing interventional tools meant for facilitating CR for people with SCIs.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Nairobi, Nairobi, Kenya and the University of KwaZulu-Natal Biomedical, Durban, South Africa (Code: BE070/18). Moreover, written informed consent was obtained from all participants prior to data collection. Additionally, all the principles of research ethics were strictly observed, including confidentiality, anonymity, and voluntary participation.
Funding
This paper was extracted from doctoral thesis of Evans Obara Obaigwa, approved by University of KwaZulu-Natal Biomedical, Durban, South Africa.
Authors' contributions
Data collection, investigation, project administration, resources, validation and software: Evans Obara Obaigwa; Supervision: Pragashnie Govender; Conceptualization, writing the original draft, review, editing, formal analysis, funding acquisition, methodology and visualization: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors acknowledge the support and assistance of the Kenyan OTs who participated in this study and Kitty Uys for her mentorship on this project.
References
- Smith EM, Sakakibara BM, Miller WC. A review of factors influencing participation in social and community activities for wheelchair users. Disabil Rehabil Assist Technol. 2016; 11(5):361-74. [DOI:10.3109/17483107.2014.989420] [PMID]
- Gutterman AS. Addressing the human rights challenges of older persons with disabilities. SSRN. 2023; 4504570. [DOI:10.2139/ssrn.4504570]
- Chhabra HS, Sharma S, Arora M. Challenges in comprehensive management of spinal cord injury in India and in the Asian Spinal Cord Network region: Findings of a survey of experts, patients and consumers. Spinal Cord. 2018; 56(1):71-7. [DOI:10.1038/sc.2017.102] [PMID]
- Obaigwa EO, Cloete G. Challenges to accessing crucial services in the management of children having autism spectrum disorders: caregivers’ perspective in Kenya. Open J Pediatr Child Health. 2019; 4(1):31-9. [DOI:10.17352/ojpch.000018]
- Burns AS, O’Connell C. The challenge of spinal cord injury care in the developing world. J Spinal Cord Med. 2012; 35(1):3-8. [DOI:10.1179/2045772311Y.0000000043] [PMID]
- World Health Organization (WHO), International spinal cord society. International perspectives on spinal cord injury. Geneva: WHO; 2013. [Link]
- Cloete LG, Obaigwa EO. Lived experiences of caregivers of children with autism spectrum disorder in Kenya. Afr J Disabil. 2019; 8:435. [DOI:10.4102/ajod.v8i0.435] [PMID]
- Ritchie J, Ormston R, McNaughton Nicholls C, Lewis J. Qualitative research practice: A guide for social science students and researchers. London: SAGE Publications; 2013. [Link]
- Morrow R, Rodriguez A, King N. Colaizzi’s descriptive phenomenological method. Psychologist. 2015; 28(8):643-4. [Link]
- Baradaran-Seyed Z, Nedjat S, Yazdizadeh B, Nedjat S, Majdzadeh R. Barriers of clinical practice guidelines development and implementation in developing countries: A case study in iran. Int J Prev Med. 2013; 4(3):340-8. [PMID]
- Bateman EA, Sreenivasan VA, Farahani F, Casemore S, Chase AD, Duley J, et al. Improving practice through collaboration: early experiences from the multi-site spinal cord injury implementation and evaluation quality care consortium. J Spinal Cord Med. 2021; 44(Suppl 1):S147-58. [DOI:10.1080/10790268.2021.1936946] [PMID]
- Barclay L, McDonald R, Lentin P, Bourke-Taylor H. Facilitators and barriers to social and community participation following spinal cord injury. Aust Occup Ther J. 2016; 63(1):19-28. [DOI:10.1111/1440-1630.12241] [PMID]
- Pernambuco AP, Lana RD, Polese JC. Knowledge and use of the ICF in clinical practice by physiotherapists and occupational therapists of Minas Gerais. Fisioter Pesqui. 2018; 25(2):134-42. [DOI:10.1590/1809-2950/16765225022018]
- Lottes IL. Sexual rights: meanings, controversies, and sexual health promotion. J Sex Res. 2013; 50(3-4):367-91. [DOI:10.1080/00224499.2013.764380] [PMID]
- McGrath M, Sakellariou D. Why has so little progress been made in the practice of occupational therapy in relation to sexuality? Am J Occup Ther. 2016; 70(1):7001360010p1-5. [DOI:10.5014/ajot.2016.017707] [PMID]
- Helland Y, Garratt A, Kjeken I, Kvien TK, Dagfinrud H. Current practice and barriers to the management of sexual issues in rheumatology: Results of a survey of health professionals. Scand J Rheumatol. 2013; 42(1):20-6. [DOI:10.3109/03009742.2012.709274] [PMID]
- Browne C, Kehoe M, Salmon N. How beliefs about bladder dysfunction among health-care professionals influence clinical practice development: perspectives of allied health professionals, nurses, and managers. Int J MS Care. 2017; 19(4):191-8. [DOI:10.7224/1537-2073.2016-006] [PMID]
- Wang C, Li J, Wan X, Wang X, Kane RL, Wang K. Effects of stigma on Chinese women’s attitudes towards seeking treatment for urinary incontinence. J Clin Nurs. 2015; 24(7-8):1112-21. [DOI:10.1111/jocn.12729] [PMID]
- Parent S, Barchi S, LeBreton M, Casha S, Fehlings MG. The impact of specialized centers of care for spinal cord injury on length of stay, complications, and mortality: A systematic review of the literature. J Neurotrauma. 2011; 28(8):1363-70. [DOI:10.1089/neu.2009.1151] [PMID]
- Middleton PM, Davies SR, Anand S, Reinten-Reynolds T, Marial O, Middleton JW. The pre-hospital epidemiology and management of spinal cord injuries in New South Wales: 2004-2008. Injury. 2012; 43(4):480-5. [DOI:10.1016/j.injury.2011.12.010] [PMID]
- Obaigwa EO, Uys CJ, Governder P. Occupational therapy rehabilitation managers’ perspectives on community integration of persons with spinal cord injuries in Nairobi, Kenya. S Afr J Occup Ther. 2023; 53(1):101-9. [DOI:10.17159/2310-3833/2023/vol53n1a11]
- Upton D, Stephens D, Williams B, Scurlock-Evans L. Occupational therapists’ attitudes, knowledge, and implementation of evidence-based practice: A systematic review of published research. Br J Occup Ther. 2014; 77(1):24-38. [DOI:10.4276/030802214X13887685335544]
- Emerich L, Parsons KC, Stein A. Competent care for persons with spinal cord injury and dysfunction in acute inpatient rehabilitation. Top Spinal Cord Inj Rehabil. 2012; 18(2):149-66. [DOI:10.1310/sci1802-149] [PMID]
- Arango-Lasprilla JC, da Silva Cardoso E, Wilson LM, Romero MG, Chan F, Sung C. Vocational rehabilitation service patterns and employment outcomes for Hispanics with spinal cord injuries. Rehabil Res Policy Educ. 2011; 25(4):149-62. [DOI:10.1891/2168-6653.25.4.149]
- Kitzman PH, Hunter EG. Developing a community-based rehabilitation network for people with spinal cord injury: A case study in Appalachian Kentucky. J Rural Community Dev. 2011; 6(1):95-104. [Link]
- Hoekstra F, Roberts L, van Lindert C, Martin Ginis KA, van der Woude LH, McColl MA. National approaches to promote sports and physical activity in adults with disabilities: Examples from the Netherlands and Canada. Disabil Rehabil. 2019; 41(10):1217-26. [DOI:10.1080/09638288.2017.1423402] [PMID]
- McVeigh J, MacLachlan M, Gilmore B, McClean C, Eide AH, Mannan H, et al. Promoting good policy for leadership and governance of health-related rehabilitation: A realist synthesis. Global Health. 2016; 12(1):49. [DOI:10.1186/s12992-016-0182-8] [PMID]
- Gosney JE, Reinhardt JD, von Groote PM, Rathore FA, Melvin JL. Medical rehabilitation of spinal cord injury following earthquakes in rehabilitation resource-scarce settings: Implications for disaster research. Spinal Cord. 2013; 51(8):603-9. [DOI:10.1038/sc.2013.50] [PMID]
- Pighills AC, Plummer D, Harvey D, Pain T. Positioning occupational therapy as a discipline on the research continuum: Results of a cross-sectional survey of research experience. Aust Occup Ther J. 2013; 60(4):241-51. [DOI:10.1111/1440-1630.12057] [PMID]
- Buckland N, Mackenzie L. Exploring the role of occupational therapy in caring for cancer survivors in Australia: A cross sectional study. Aust Occup Ther J. 2017; 64(5):358-68. [DOI:10.1111/1440-1630.12386] [PMID]
Type of Study: Research |
Subject:
Occupational Therapy
Received: 2025/06/5 | Accepted: 2025/09/16 | Published: 2025/03/2
Received: 2025/06/5 | Accepted: 2025/09/16 | Published: 2025/03/2
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.