

Volume 7, Issue 1 (Continuously Updated 2024)
Func Disabil J 2024, 7(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Eshghi M, Akbarfahimi M, Taghizadeh Hajlouee G, Hojati Abed E. The Face and Content Validity of the Persian Version of Occupational Identity Questionnaire in People With Multiple Sclerosis. Func Disabil J 2024; 7 (1)
URL: http://fdj.iums.ac.ir/article-1-291-en.html
URL: http://fdj.iums.ac.ir/article-1-291-en.html



1- Department of Occupational Therapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran.
2- Rehabilitation Research Center, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Occupational Therapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran. ,hojatiabed.e@iums.ac.ir
2- Rehabilitation Research Center, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Occupational Therapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 632 kb]
(574 Downloads)
| Abstract (HTML) (1448 Views)
Full-Text: (394 Views)
Introduction
Multiple sclerosis (MS) is a common neurological condition among young adults that has a chronic, degenerative, and disabling nature [1]. People with multiple sclerosis (PwMS) often face a variety of symptoms, such as visual impairments, tremors, ataxia, fatigue, imbalance, bowel/bladder problems, cognitive decline, and psychological disorders [2]. These symptoms can prevent them from engaging in their typical occupations and changes in occupational abilities may change their understanding of how they perform in their occupations [3]. The effect of this inability on their sense of occupational identity is not fairly understood.
Occupational identity is shaped by a sense that we are as an occupational being and it depends on our past, current, and future occupations [4]. This definition shows that occupation and identity are separate but connected concepts [5]. When an illness or condition leads to reduced engagement in occupations, it may have detrimental impacts on one’s occupational identity; as a result, individuals consistently try to restore their occupational performance and regain their occupational identity [6]. Furthermore, occupational identity can influence clients’ motivation and adherence to therapy. A well-defined occupational identity enhances patients’ perceptions of their occupational roles and helps them set meaningful goals for their therapy [7, 8].
The occupational identity questionnaire (OIQ) is a new tool exclusively intended to assess occupational identity (OI); Shikata developed this questionnaire in Japan to assess OI in the elderly [9]. OIQ has 14 items and is divided into three sections, individuals’ feelings about themselves in present and future expectations, individuals’ feelings about their past, and satisfaction with the present condition. This questionnaire is self-reported, allowing clients to respond on a 4-point Likert scale [9]. Since this questionnaire was originally designed for the elderly, it was predicted that it may need some adaptations to be suitable for PwMS. As a result, the study was conducted to assess the face and content validity of the OIQ and make necessary changes according to patients’ and experts’ opinions.
Materials and Methods
In this study, the Persian version of OIQ was used after permission was obtained from the developer. The study used a methodological design and was completed in May 2024. In this study, we evaluated the content and face validity of OIQ. The Research Ethics Committee of the Iran University of Medical Science assessed and approved the study design. The authors informed all participants about the study’s objectives, and informed consent forms were signed by the participants.
Face validity
A total of 15 Iranian patients diagnosed with MS participated in the face validity study. The inclusion criteria included being diagnosed with MS by 2 neurologists according to the revised McDonald criteria [10], diagnosis duration ≥ 6 months, education level ≥5 years, Montreal cognitive assessment scores (MoCA) ≥26 [11], Beck depression inventory scores (BDI-II) ≤29 [12], not having other neurological disorders or visual impairment according to the patient’s statement.
Content validity
A total of 12 PhDs in occupational therapy and PhD candidates participated in the study of the content validity ratio (CVR) and content validity index (CVI). The inclusion criteria included having ≥5 years of experience in the field of neurology especially MS, being familiar with the concepts of occupational therapy and occupational identity, or having published articles in these fields.
Measures
Dr. Shikata created OIQ in Japan. Initially, its purpose was to evaluate the occupational identity among the elderly population. The questionnaire is composed of 14 items, divided into three sections, individuals’ feelings about themselves in present and future expectations, individuals’ feelings about their past and satisfaction with present condition. Respondents answer the items on a Likert scale from ‘strongly agree’ to ‘strongly disagree’. Scores are assigned on a scale from 4 (strongly agree) to 1 (strongly disagree). Scores range from 14 to 56; higher scores indicate a stronger sense of OI and lower scores indicate a weaker sense of OI [9].
Face validity
The face validity was first assessed qualitatively through in-person interviews. Each participant evaluated every item about its comprehensibility, clarity, and potential ambiguity. Second, a quantitative assessment was conducted by measuring each item’s importance with the item impact method (IIM). The measurement was performed using a 5-point Likert scale which ranged from 1 (not important at all) to 5 (quite important). Items IIM was calculated according to Equation 1:
1. Impact Score: Importance×Frequency (%).
Items which receive a score >1.5 are suitable for subsequent analysis.
Content validity
CVR and CVI were employed to evaluate the validity of the content [13, 14]. To calculate the CVR, the necessity and essentiality of each item were evaluated using a 3-point Likert scale [15]. The assessment involved 12 occupational therapists but one was excluded due to filling the form incompletely and not responding to our emails. The formula of the CVR is (Equation 2):
2. CVR=(Ne–N/2)/(N/2);
Ne represents the number of experts indicating an item as “essential” and N represents the number of experts participating in the evaluation. According to Lawshe’s Table, a critical value of CVR >0.59 is acceptable for 11 experts [14]. CVI is a widely used method to examine content validity [14]. In this research, item-level-CVI (I-CVI) and scale-level-CVI (S-CVI) were employed. I-CVI assesses the relevance of each item according to the Likert scale. For each category, we calculate the proportion of experts who selected ratings 3 and 4 on the Likert scale, relative to the total number of experts [16]. The result of this calculation varies between 0 to 1. An item is considered eligible if its I-CVI exceeds 0.79. If the value falls between 0.7 to 0.79, it indicates that the item requires revisions. Items with values below 0.7 are considered for elimination [16]. In addition, the overall CVI of the scale was calculated by methods of scale CVI/universal agreement (S-CVI/UA) and scale CVI/average proportion (S-CVI)/Ave. S-CVI/UA indicates the proportion of items that receive a relevancy score of 1 by all the respondents and it shows agreement among experts on each item’s relevancy. S-CVI/Ave is an average of I-CVI scores for all the items [17].
Results
Face validity
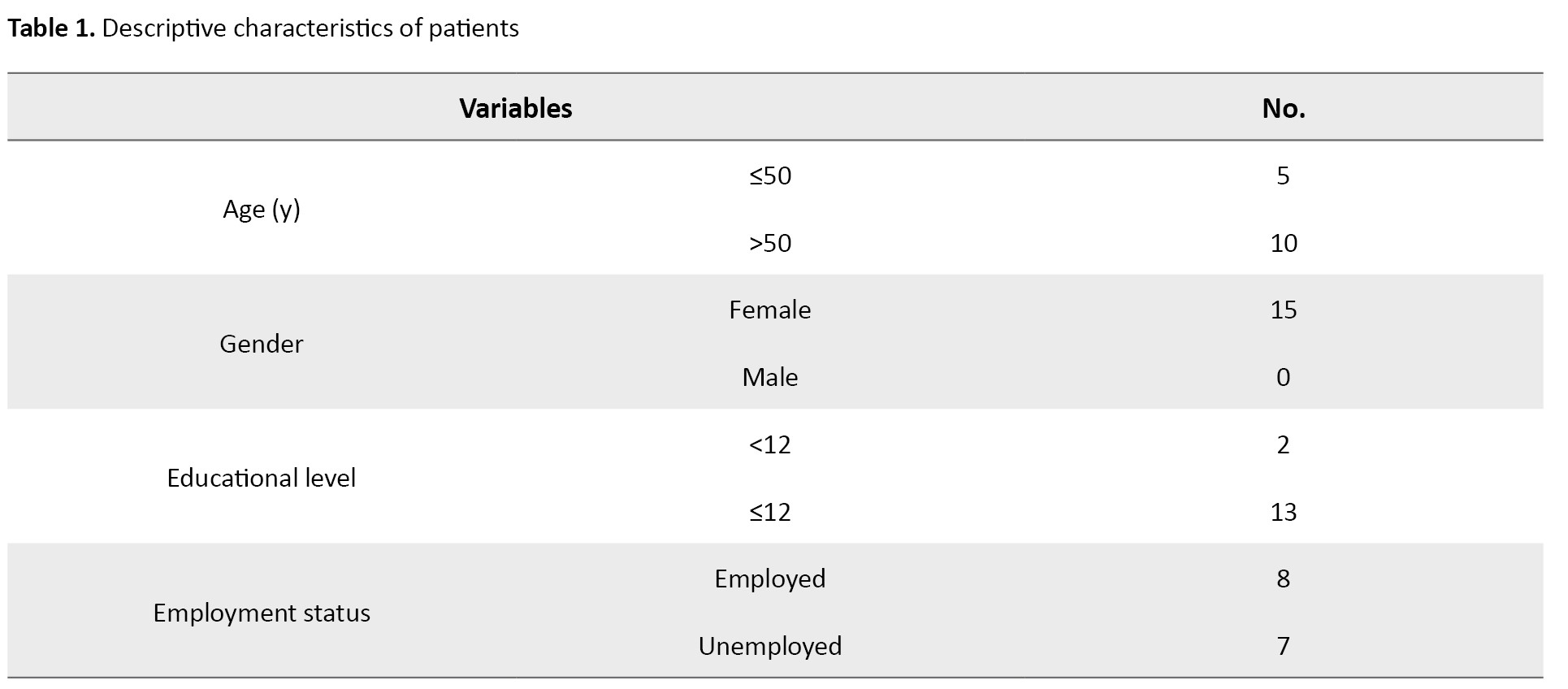
Table 1 presents the demographic characteristics of 15 participants who took part in the evaluation of the face validity.
In the quantitative study, all the items received item impact scores (IIS) above 1.5 indicating sufficient importance for all the items. IIS scores ranged from 3.03 to 4.62. Also, during qualitative interviews, none of the items were mentioned as ambiguous or incomprehensible. Since all the items were deemed comprehensible and received sufficient IIS scores, we decided not to eliminate any of them.
Content validity
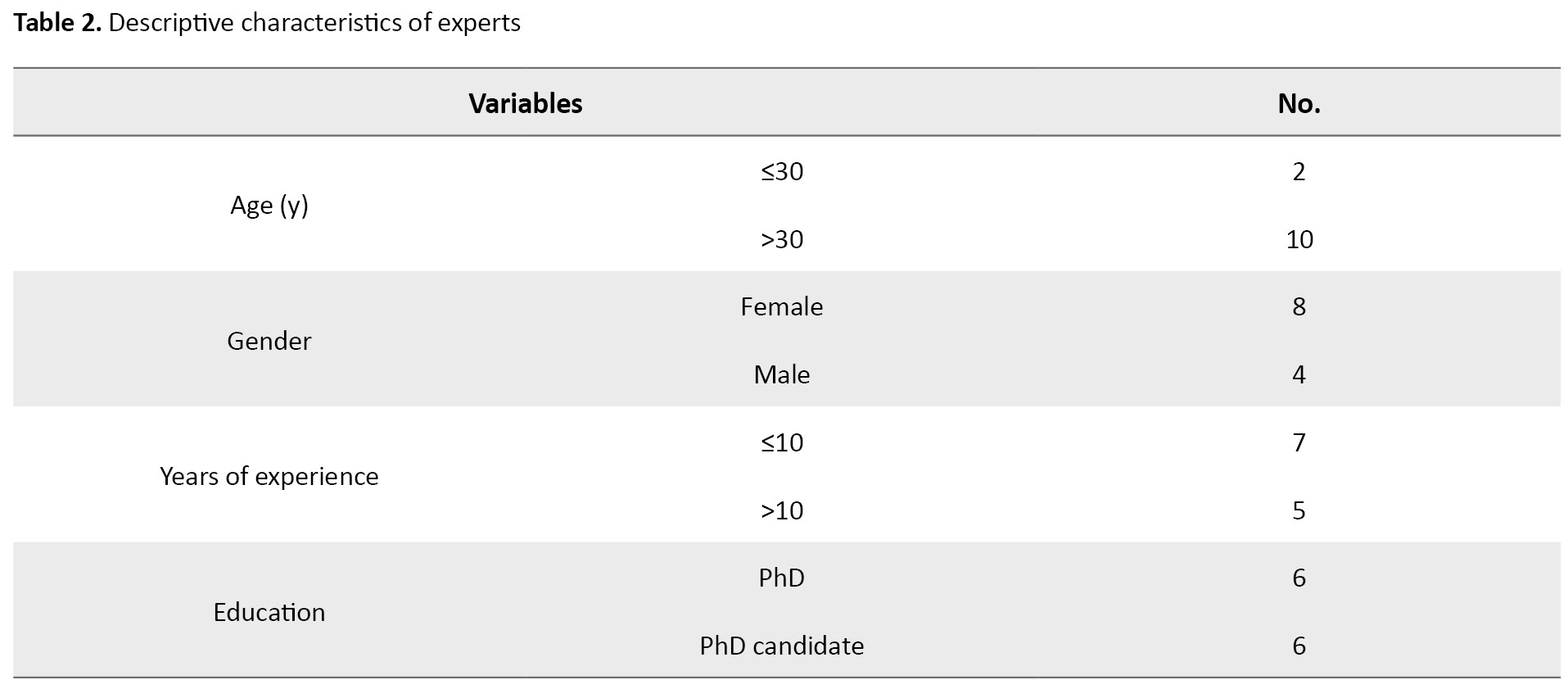
The study on CVR involved the participation of 12 occupational therapists; one of the experts was excluded because he did not complete the form or respond to our emails; therefore, calculations proceeded with the remaining 11 experts (Table 2).
According to Lawshe’s table, the CVR value for each item should be higher than 0.59 when evaluated by 11 experts [18]. Items with non-essential or less essential scores should be removed. In our study, all items received scores higher than the specified value of 0.59; therefore, we retained all the items. The scores for each item varied between 0.63 and 1. The average score of CVR was 0.89.
CVI evaluation was also conducted with the participation of these 12 experts. In this stage, item level CVI (I-CVI) scores for relevancy ranged from 0.83 to 1, demonstrating sufficient relevance. The S-CVI/UA score was calculated at 0.57. Furthermore, the S-CVI/Ave score was 0.94, showing excellent scale level content validity. However, we received comments from experts concerning adaptations for items 6 and 10. The experts’ opinions indicated that items 6 and 10 needed to be revised to be appropriate for PwMS (Table 3).
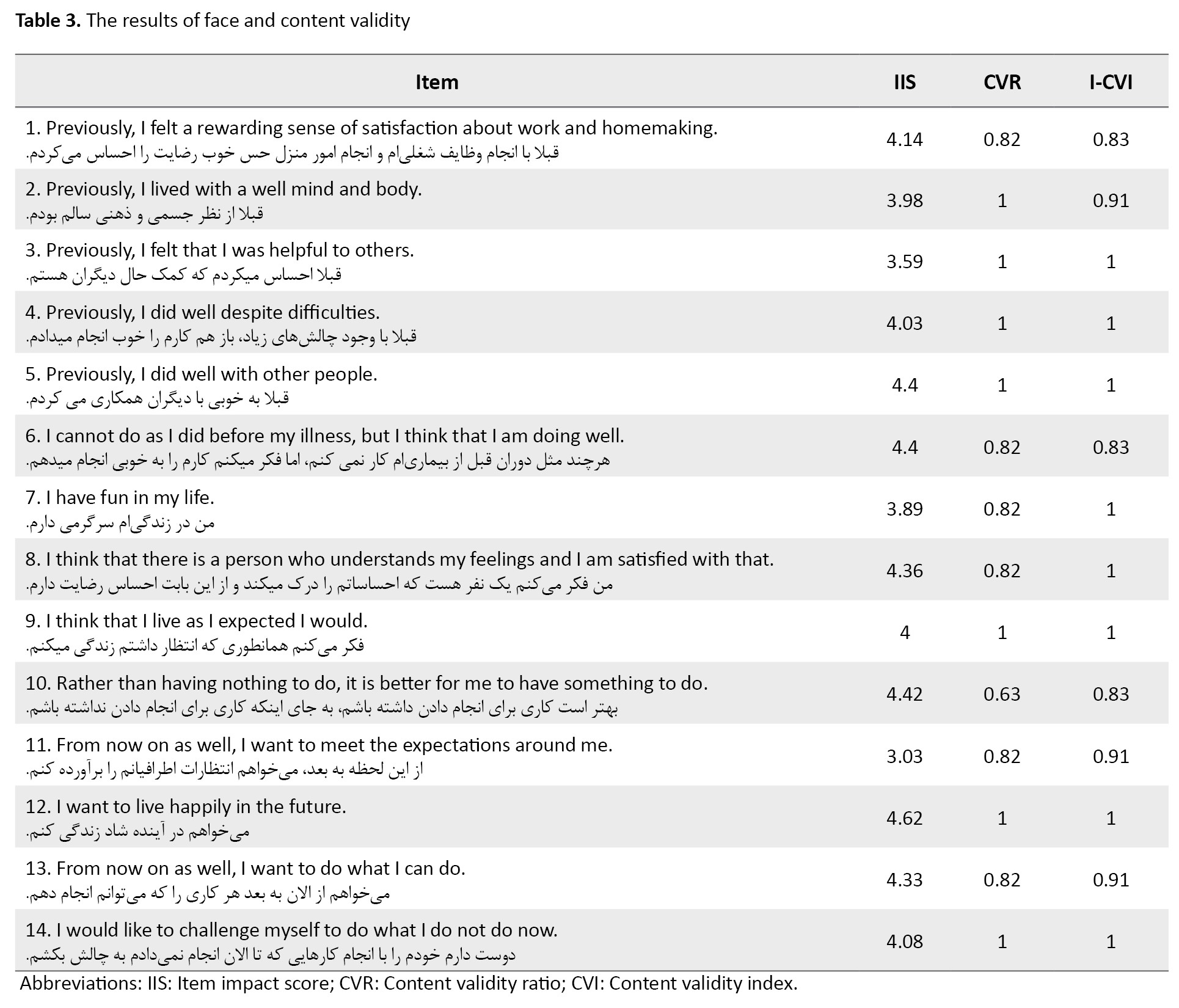
Based on these opinions, 2 out of 14 items (6 and 10) were modified to align with MS. In the original version of the questionnaire, item 6 was “I cannot do as I did when I was young, but I think that I am doing well” which was converted to “I cannot do as I did before my illness, but I think that I am doing well” in MS modified version. Item 10 converted from “rather than having nothing to do, it is better to have something to do” to “rather than having nothing to do, I should have something to do”. The revised version was submitted to the developers, and after receiving their approval, we implemented these modifications in the Persian version. Furthermore, the revised version was sent to experts who participated in the study, and their approval was also received.
Discussion
The face validity of the OIQ was qualitatively and quantitatively assessed for PwMS. In the qualitative study, participants evaluated whether the items on the questionnaire were clear and understandable. The feedback indicated that all the items were understandable for patients and they did not report any ambiguity. In the quantitative study, they evaluated OIQ items in terms of their importance and results indicated that all the items were perceived as crucial for assessing occupational identity in PwMS. The high face validity suggests that the items are perceived as crucial and comprehensible by patients, which is crucial to ensure respondents understand and engage with the questionnaire. In addition, high face validity may lead to improved factor analysis and enhance the questionnaire [19].
Content validity was evaluated by the involvement of occupational therapy experts. Each expert rated the necessity and relevance of each item on the OIQ. The CVR and CVI were calculated to quantify the content validity. The CVR and CVI scores were above determined cut-off points, indicating a high level of content validity. These high CVR and CVI scores suggest that the items cover the domain of occupational identity for PwMS. According to experts’ comments, two items were identified as needing revision to better adapt for PwMS. These items were subsequently modified based on the suggestions. 8 out of 14 items scored a 1 in the CVI/UA evaluation, indicating complete agreement among experts. Therefore, these items appear to be essential to assess OI. The results from content validity assessments demonstrated that the OIQ is a suitable tool to assess OI. The high content validity, as demonstrated by CVR and CVI, shows that the items are essential to assess OI and they adequately cover all relevant aspects of OI. These results were consistent with the results of Shikata et al. that OIQ showed sufficient validity for the elderly [9, 20].
Evaluating occupational identity is crucial in the occupational therapy process because when therapists have a better understanding of how MS affects their client’s roles and sense of occupational identity, they can plan their interventions based on those changes [21]. OIQ can be a useful tool for this evaluation if more studies prove its psychometric properties. Furthermore, OIQ was originally designed in the East, allowing for better cultural adaptation with the Iranian community, requiring more investigations. The briefness of the OIQ is another advantage, making it more suitable for PwMS who often experience fatigue. However, insufficient evidence is available for the validity and reliability of this questionnaire, and future investigations are needed to evaluate its psychometric properties, such as test re-test reliability, internal consistency, construct validity, and discriminant validity. It is essential to remember that occupational identity is a multi-dimensional concept and it is still unclear that if OIQ can assess all those dimensions or not; therefore, it is necessary to do more research on its usability.
This study had some strengths and limitations. One of the strengths is the involvement of experienced occupational therapists, which enhances the robustness of the validity assessments. However, there were some limitations in the study; for example, the sample size of patients was adequate, but it could be expanded. In addition, all participants were female in the face validity study.
Conclusion
The Persian version of the OIQ demonstrated strong face and content validity, indicating that it is a suitable tool for assessing occupational identity. The high validity scores suggest that the questionnaire items are comprehensible, crucial, essential, and relevant. Future studies must evaluate other psychometric properties, such as test re-test reliability, internal consistency, construct validity, and discriminant validity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Science (Code: IR. IUMS.REC.1402.771).
Funding
This article was extracted from Msc thesis of the Mahya Eshghiو approved in the Departement of Occupational Therapy, Faculty of Rehabilitation, Iran University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Thanks to all the experts and respondants who contributed to the study. And our special thanks to individuals who participated in the study.
References
Multiple sclerosis (MS) is a common neurological condition among young adults that has a chronic, degenerative, and disabling nature [1]. People with multiple sclerosis (PwMS) often face a variety of symptoms, such as visual impairments, tremors, ataxia, fatigue, imbalance, bowel/bladder problems, cognitive decline, and psychological disorders [2]. These symptoms can prevent them from engaging in their typical occupations and changes in occupational abilities may change their understanding of how they perform in their occupations [3]. The effect of this inability on their sense of occupational identity is not fairly understood.
Occupational identity is shaped by a sense that we are as an occupational being and it depends on our past, current, and future occupations [4]. This definition shows that occupation and identity are separate but connected concepts [5]. When an illness or condition leads to reduced engagement in occupations, it may have detrimental impacts on one’s occupational identity; as a result, individuals consistently try to restore their occupational performance and regain their occupational identity [6]. Furthermore, occupational identity can influence clients’ motivation and adherence to therapy. A well-defined occupational identity enhances patients’ perceptions of their occupational roles and helps them set meaningful goals for their therapy [7, 8].
The occupational identity questionnaire (OIQ) is a new tool exclusively intended to assess occupational identity (OI); Shikata developed this questionnaire in Japan to assess OI in the elderly [9]. OIQ has 14 items and is divided into three sections, individuals’ feelings about themselves in present and future expectations, individuals’ feelings about their past, and satisfaction with the present condition. This questionnaire is self-reported, allowing clients to respond on a 4-point Likert scale [9]. Since this questionnaire was originally designed for the elderly, it was predicted that it may need some adaptations to be suitable for PwMS. As a result, the study was conducted to assess the face and content validity of the OIQ and make necessary changes according to patients’ and experts’ opinions.
Materials and Methods
In this study, the Persian version of OIQ was used after permission was obtained from the developer. The study used a methodological design and was completed in May 2024. In this study, we evaluated the content and face validity of OIQ. The Research Ethics Committee of the Iran University of Medical Science assessed and approved the study design. The authors informed all participants about the study’s objectives, and informed consent forms were signed by the participants.
Face validity
A total of 15 Iranian patients diagnosed with MS participated in the face validity study. The inclusion criteria included being diagnosed with MS by 2 neurologists according to the revised McDonald criteria [10], diagnosis duration ≥ 6 months, education level ≥5 years, Montreal cognitive assessment scores (MoCA) ≥26 [11], Beck depression inventory scores (BDI-II) ≤29 [12], not having other neurological disorders or visual impairment according to the patient’s statement.
Content validity
A total of 12 PhDs in occupational therapy and PhD candidates participated in the study of the content validity ratio (CVR) and content validity index (CVI). The inclusion criteria included having ≥5 years of experience in the field of neurology especially MS, being familiar with the concepts of occupational therapy and occupational identity, or having published articles in these fields.
Measures
Dr. Shikata created OIQ in Japan. Initially, its purpose was to evaluate the occupational identity among the elderly population. The questionnaire is composed of 14 items, divided into three sections, individuals’ feelings about themselves in present and future expectations, individuals’ feelings about their past and satisfaction with present condition. Respondents answer the items on a Likert scale from ‘strongly agree’ to ‘strongly disagree’. Scores are assigned on a scale from 4 (strongly agree) to 1 (strongly disagree). Scores range from 14 to 56; higher scores indicate a stronger sense of OI and lower scores indicate a weaker sense of OI [9].
Face validity
The face validity was first assessed qualitatively through in-person interviews. Each participant evaluated every item about its comprehensibility, clarity, and potential ambiguity. Second, a quantitative assessment was conducted by measuring each item’s importance with the item impact method (IIM). The measurement was performed using a 5-point Likert scale which ranged from 1 (not important at all) to 5 (quite important). Items IIM was calculated according to Equation 1:
1. Impact Score: Importance×Frequency (%).
Items which receive a score >1.5 are suitable for subsequent analysis.
Content validity
CVR and CVI were employed to evaluate the validity of the content [13, 14]. To calculate the CVR, the necessity and essentiality of each item were evaluated using a 3-point Likert scale [15]. The assessment involved 12 occupational therapists but one was excluded due to filling the form incompletely and not responding to our emails. The formula of the CVR is (Equation 2):
2. CVR=(Ne–N/2)/(N/2);
Ne represents the number of experts indicating an item as “essential” and N represents the number of experts participating in the evaluation. According to Lawshe’s Table, a critical value of CVR >0.59 is acceptable for 11 experts [14]. CVI is a widely used method to examine content validity [14]. In this research, item-level-CVI (I-CVI) and scale-level-CVI (S-CVI) were employed. I-CVI assesses the relevance of each item according to the Likert scale. For each category, we calculate the proportion of experts who selected ratings 3 and 4 on the Likert scale, relative to the total number of experts [16]. The result of this calculation varies between 0 to 1. An item is considered eligible if its I-CVI exceeds 0.79. If the value falls between 0.7 to 0.79, it indicates that the item requires revisions. Items with values below 0.7 are considered for elimination [16]. In addition, the overall CVI of the scale was calculated by methods of scale CVI/universal agreement (S-CVI/UA) and scale CVI/average proportion (S-CVI)/Ave. S-CVI/UA indicates the proportion of items that receive a relevancy score of 1 by all the respondents and it shows agreement among experts on each item’s relevancy. S-CVI/Ave is an average of I-CVI scores for all the items [17].
Results
Face validity
Table 1 presents the demographic characteristics of 15 participants who took part in the evaluation of the face validity.
In the quantitative study, all the items received item impact scores (IIS) above 1.5 indicating sufficient importance for all the items. IIS scores ranged from 3.03 to 4.62. Also, during qualitative interviews, none of the items were mentioned as ambiguous or incomprehensible. Since all the items were deemed comprehensible and received sufficient IIS scores, we decided not to eliminate any of them.
Content validity
The study on CVR involved the participation of 12 occupational therapists; one of the experts was excluded because he did not complete the form or respond to our emails; therefore, calculations proceeded with the remaining 11 experts (Table 2).
According to Lawshe’s table, the CVR value for each item should be higher than 0.59 when evaluated by 11 experts [18]. Items with non-essential or less essential scores should be removed. In our study, all items received scores higher than the specified value of 0.59; therefore, we retained all the items. The scores for each item varied between 0.63 and 1. The average score of CVR was 0.89.
CVI evaluation was also conducted with the participation of these 12 experts. In this stage, item level CVI (I-CVI) scores for relevancy ranged from 0.83 to 1, demonstrating sufficient relevance. The S-CVI/UA score was calculated at 0.57. Furthermore, the S-CVI/Ave score was 0.94, showing excellent scale level content validity. However, we received comments from experts concerning adaptations for items 6 and 10. The experts’ opinions indicated that items 6 and 10 needed to be revised to be appropriate for PwMS (Table 3).
Based on these opinions, 2 out of 14 items (6 and 10) were modified to align with MS. In the original version of the questionnaire, item 6 was “I cannot do as I did when I was young, but I think that I am doing well” which was converted to “I cannot do as I did before my illness, but I think that I am doing well” in MS modified version. Item 10 converted from “rather than having nothing to do, it is better to have something to do” to “rather than having nothing to do, I should have something to do”. The revised version was submitted to the developers, and after receiving their approval, we implemented these modifications in the Persian version. Furthermore, the revised version was sent to experts who participated in the study, and their approval was also received.
Discussion
The face validity of the OIQ was qualitatively and quantitatively assessed for PwMS. In the qualitative study, participants evaluated whether the items on the questionnaire were clear and understandable. The feedback indicated that all the items were understandable for patients and they did not report any ambiguity. In the quantitative study, they evaluated OIQ items in terms of their importance and results indicated that all the items were perceived as crucial for assessing occupational identity in PwMS. The high face validity suggests that the items are perceived as crucial and comprehensible by patients, which is crucial to ensure respondents understand and engage with the questionnaire. In addition, high face validity may lead to improved factor analysis and enhance the questionnaire [19].
Content validity was evaluated by the involvement of occupational therapy experts. Each expert rated the necessity and relevance of each item on the OIQ. The CVR and CVI were calculated to quantify the content validity. The CVR and CVI scores were above determined cut-off points, indicating a high level of content validity. These high CVR and CVI scores suggest that the items cover the domain of occupational identity for PwMS. According to experts’ comments, two items were identified as needing revision to better adapt for PwMS. These items were subsequently modified based on the suggestions. 8 out of 14 items scored a 1 in the CVI/UA evaluation, indicating complete agreement among experts. Therefore, these items appear to be essential to assess OI. The results from content validity assessments demonstrated that the OIQ is a suitable tool to assess OI. The high content validity, as demonstrated by CVR and CVI, shows that the items are essential to assess OI and they adequately cover all relevant aspects of OI. These results were consistent with the results of Shikata et al. that OIQ showed sufficient validity for the elderly [9, 20].
Evaluating occupational identity is crucial in the occupational therapy process because when therapists have a better understanding of how MS affects their client’s roles and sense of occupational identity, they can plan their interventions based on those changes [21]. OIQ can be a useful tool for this evaluation if more studies prove its psychometric properties. Furthermore, OIQ was originally designed in the East, allowing for better cultural adaptation with the Iranian community, requiring more investigations. The briefness of the OIQ is another advantage, making it more suitable for PwMS who often experience fatigue. However, insufficient evidence is available for the validity and reliability of this questionnaire, and future investigations are needed to evaluate its psychometric properties, such as test re-test reliability, internal consistency, construct validity, and discriminant validity. It is essential to remember that occupational identity is a multi-dimensional concept and it is still unclear that if OIQ can assess all those dimensions or not; therefore, it is necessary to do more research on its usability.
This study had some strengths and limitations. One of the strengths is the involvement of experienced occupational therapists, which enhances the robustness of the validity assessments. However, there were some limitations in the study; for example, the sample size of patients was adequate, but it could be expanded. In addition, all participants were female in the face validity study.
Conclusion
The Persian version of the OIQ demonstrated strong face and content validity, indicating that it is a suitable tool for assessing occupational identity. The high validity scores suggest that the questionnaire items are comprehensible, crucial, essential, and relevant. Future studies must evaluate other psychometric properties, such as test re-test reliability, internal consistency, construct validity, and discriminant validity.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Iran University of Medical Science (Code: IR. IUMS.REC.1402.771).
Funding
This article was extracted from Msc thesis of the Mahya Eshghiو approved in the Departement of Occupational Therapy, Faculty of Rehabilitation, Iran University of Medical Science.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Thanks to all the experts and respondants who contributed to the study. And our special thanks to individuals who participated in the study.
References
- Oh J, Vidal-Jordana A, Montalban X. Multiple sclerosis: Clinical aspects. Curr Opin Neurol. 2018; 31(6):752-9. [DOI:10.1097/WCO.0000000000000622] [PMID]
- Battaglia MA, Bezzini D, Cecchini I, Cordioli C, Fiorentino F, Manacorda T, et al. Patients with multiple sclerosis: A burden and cost of illness study. J Neurol. 2022; 269(9):5127-35. [DOI:10.1007/s00415-022-11169-w] [PMID]
- Squillace M, Linden P. The lived experiences and occupational performance and satisfaction of young adults with Multiple Sclerosis (MS) as related to fine motor skills. Open J Occup Ther. 2022; 10(2):1-9. [DOI:10.15453/2168-6408.1920]
- Bryson-Campbell M. Examining the shift in occupational identity after a brain injury [PhD dissertation]. Ontario: The University of Western Ontario (Canada); 2013. [Link]
- Hansson SO, Björklund Carlstedt A, Morville AL. Occupational identity in occupational therapy: A concept analysis. Scand J Occup Ther. 2022; 29(3):198-209. [DOI:10.1080/11038128.2021.1948608] [PMID]
- Walder K, Molineux M. Re-establishing an occupational identity after stroke-a theoretical model based on survivor experience. Br J Occup Ther. 2017; 80(10):620-30. [DOI:10.1177/0308022617722711]
- Kielhofner G. Conceptual foundations of occupational therapy practice. Pennsylvania: F. A. Davis Company; 2009. [Link]
- Wilcock A, Hocking C. An occupational perspective of health. New York: Routledge; 2024. [DOI:10.4324/9781003525233]
- Shikata M, Notoh H, Shinohara K, Yabuwaki K, Ishii Y, Yamada T, et al. An examination of the psychometric properties of the occupational identity questionnaire for community-living elderly who require care. Hong Kong J Occup Ther. 2021; 34(1):30-8. [DOI:10.1177/1569186121997936] [PMID]
- Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018; 17(2):162-73.[DOI:10.1016/S1474-4422(17)30470-2] [PMID]
- Rashedi V, Foroughan M, Chehrehnegar N. Psychometric properties of the Persian Montreal Cognitive Assessment in mild cognitive impairment and Alzheimer disease. Dement Geriatr Cogn Dis Extra. 2021; 11(1):51-7. [DOI:10.1159/000514673] [PMID]
- Hamidi R, Fekrizadeh Z, Azadbakht M, Garmaroudi G, Taheri Tanjani P, Fathizadeh S, et al. [Validity and reliability Beck Depression Inventory-II among the Iranian elderly population (Persian)]. J Sabzevar Univ Med Sci. 2015; 22(1):189-98. [Link]
- Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007; 30(4):459-67. [DOI:10.1002/nur.20199] [PMID]
- Lawshe CH. A quantitative approach to content validity. Pers Psychol. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Yamada J, Stevens B, Sidani S, Watt-Watson J, de Silva N. Content validity of a process evaluation checklist to measure intervention implementation fidelity of the EPIC intervention. Worldviews Evid Based Nurs. 2010; 7(3):158-64. [DOI:10.1111/j.1741-6787.2010.00182.x] [PMID]
- Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar AR. Design and implementation content validity study: Development of an instrument for measuring patient-centered communication. J Caring Sci. 2015; 4(2):165-78. [DOI:10.15171/jcs.2015.017] [PMID]
- Polit DF, Beck CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. 2006; 29(5):489-97. [DOI:10.1002/nur.20147] [PMID]
- Ayre C, Scally AJ. Critical values for Lawshe's content validity ratio: revisiting the original methods of calculation. Meas Eval Couns Dev. 2014; 47(1):79-86. [DOI:10.1177/0748175613513808]
- Wetzel AP. Factor analysis methods and validity evidence: A review of instrument development across the medical education continuum. Acad Med. 2012; 87(8):1060-9. [DOI:10.1097/ACM.0b013e31825d305d] [PMID]
- Shikata M, Notoh H, Shinohara K, Yabuwaki K, Ishii Y, Yamada T. Content and face validity of an occupational identity questionnaire based on MOHO concept for community-living elderly people requiring support. J Japan Acad Health Sci. 2020; 23(2):75-87. [Link]
- Vitturi BK, Rahmani A, Dini G, Montecucco A, Debarbieri N, Sbragia E, et al. Occupational outcomes of people with multiple sclerosis: A scoping review. BMJ Open. 2022; 12(7):e058948. [DOI:10.1136/bmjopen-2021-058948] [PMID]
Type of Study: Research |
Subject:
Occupational Therapy
Received: 2024/10/19 | Accepted: 2024/11/3 | Published: 2024/03/12
Received: 2024/10/19 | Accepted: 2024/11/3 | Published: 2024/03/12
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.