

Volume 7, Issue 1 (Continuously Updated 2024)
Func Disabil J 2024, 7(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Emadi S P, Mansour Sohani S, Salehi R, Darzi M T. Relationship Between Pain, Muscle Strength, Function, and Quality of Life in Overhead Players With Chronic Internal Shoulder Impingement. Func Disabil J 2024; 7 (1)
URL: http://fdj.iums.ac.ir/article-1-249-en.html
URL: http://fdj.iums.ac.ir/article-1-249-en.html



1- Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran. ,Sohani.soheil@gmail.com
3- Department of Physiotherapy, School of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
2- Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences, Tehran, Iran. ,
3- Department of Physiotherapy, School of Rehabilitation, Babol University of Medical Sciences, Babol, Iran.
Full-Text [PDF 1713 kb]
(46 Downloads)
| Abstract (HTML) (73 Views)
Full-Text: (16 Views)
Introduction
Shoulder pain has the third rank among other pains. Shoulder impingement syndrome is the most common disease of shoulder complaints among individuals. It is classified into three subsets, internal, subacromial, and subcoracoid impingement [1, 2].
These patients state pain during elevating the arm or lying on the painful shoulder [3]. The prevalence of this syndrome is estimated at about 44%–65% of all shoulder pain disorders [4]. This syndrome is one of the most common injuries happening in overhead throwers due to normal physiological contact between the posterosuperior glenoid and the greater tuberosity in repetitive hyperabduction and external rotation positions. This physiological contact can be symptomatic when repeated overhead motions result in partial articular-sided posterosuperior rotator cuff tears and lesions of the posterosuperior glenoid labrum, therefore, posterosuperior rotator cuff and labrum will be “pinched” in the space of greater tuberosity and the glenoid rim. This syndrome is multifactorial, such as shoulder physiological remodeling, contracture of the posterior capsule, and scapular dyskinesis. These factors cause shoulder pathologies like glenohumeral internal rotation deficit (GIRD), humeral hyper angulation, and superior labral anterior to posterior (SLAP) tears [5].
Jobe [6] and Walch et al. [7, 8] assert the mechanism of impingement syndrome as an entrapment between the greater tuberosity and glenoid labrum during shoulder abduction and lateral rotation in the interval between supraspinatus and infraspinatus tendons. Walch et al suggested that anterior glenohumeral (GH) laxity has an important role in this syndrome in overhead throwers [7].
This syndrome causes pain in the posterior of the shoulder and happens in the throwers usually during cocking phase of throwing or pitching in the GH joint, whether in excessive external rotation and horizontal abduction or in abduction and shoulder flexion. Other associated pathologies with this syndrome are labrum injury, rotator cuff tear; mostly infraspinatus muscle, greater tuberosity injury, Inferior glenohumeral ligament injury, GIRD, and scapular dyskinesis [9, 10].
According to Jobe’s categorization of the internal impingement syndrome into three stages regarding to patient’s symptoms and presentations, patients in the early stage complain of shoulder stiffness and required to warm–up longer but have no problem with activity daily livings [6]. During the intermediate stage, patients reported pain in the posterior side of the shoulder during the late phase of cocking and have no pain during activities of daily livings (ADLs). During the advanced stage, the patient’s symptoms are like an intermediate stage, but will not get better with rest and rehabilitation [11].
Materials and Methods
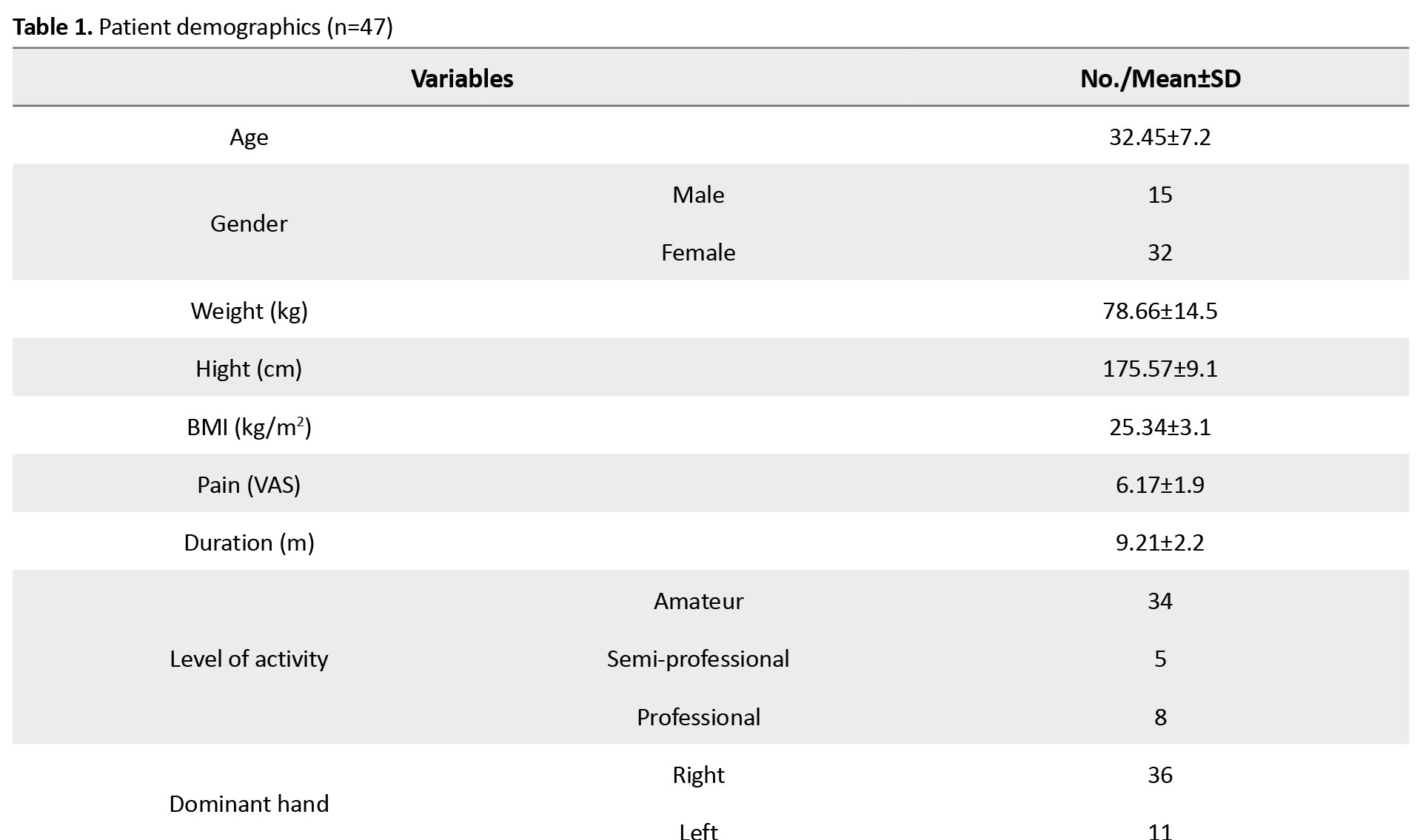
This is a correlation study that was conducted at a hospital in Tehran during the summer of 2023. Forty-seven participants (32 males, 15 females) overhead players (volleyball, basketball, badminton, bodybuilding, powerlifting, and swimming) with chronic shoulder internal impingement syndrome participated in this study. Players were tested by shoulder fellowship (orthopedic surgeon) and PhD in physiotherapy. Players entered by checking the inclusion and exclusion criteria and filling out the consent forms. Then, the pain was measured by a visual analogue scale (VAS). Muscle strength was measured by a handheld dynamometer (Imada design) with the ability to measure tensional strengths and a pressure capacity of 500 N, and a precision of 0.1 N (Figure 1).
Inclusion criteria
The inclusion criteria included 15 to 45-year-old male and female overhead throwers (elite, semi-professional, amateur) with chronic shoulder internal impingement [11, 12], players with no cortisone injection in the last 3 months [11], complaining reduction in ball speed, endurance and ball control during throwing [11, 12], and having the ability to read and write in Persian.
Exclusion criteria
The exclusion criteria included players with a history of neck, shoulder, elbow, and hand pain and injuries in the last 3 months, instability or dislocation of GH joint, undergoing neck and shoulder, elbow, and wrist surgeries last year, and player’s unwillingness to participate in this research [12].
Questionnaires
Disabilities of the arm, shoulder, and hand (DASH)
Persian form of DASH questionnaire was used to determine symptoms and degree of disability of musculoskeletal disorders of upper limbs. The severity of symptoms, pain, weakness and arm stiffness, function, work, and exercise were discussed. It was completed by players [13]. The scores were converted to percentages by computer program.
Shoulder pain and disability index (SPADI)
Persian form of SPADI questionnaire was used to measure shoulder pain and disability, disability, pain in different situations, and the ability of a person to perform ADL are discussed. It was completed by the players [14]. The scores were converted to percentages by computer program.
Short form (SF)-36
We used the Persian short form (SF)-36 with eight subgroups. Physical and mental aspects were discussed, which examines the pain, health status and its impact on ADL and social activities [15, 16]. The scores were converted to percentages by computer program.
Handheld dynamometer
It was used to measure the isometric strength of all shoulder muscles on both healthy and affected sides in Newton and players were asked to hold the maximal voluntary isometric contraction (MVIC) in the middle range for 3 s and rest 30 s between tests and contractions were asked for 3 times on both sides and the average of the contractions was calculated [17] (Figure 1).
Muscle tests MVIC
Shoulder flexors (anterior deltoid, biceps, coracobrachialis)
For MVIC of shoulder flexors, players lay in a supine position with shoulder 90° flexion, elbow extension, and the palm faced to the lower limb. It was placed exactly proximal to the styloid process of the ulna at the level of the extensors. Players were asked to apply force to the dynamometer for 3 s in the direction of shoulder flexion, and after each contraction, they rested for 30 s, we considered the average contractions of both shoulder sides [18] (Figure 2).

Shoulder extensors (latisimus dorsi, teres major, posterior deltoid)
For MVIC of shoulder extensors, players lay in a supine position with shoulder 90° flexion, and elbow was completely extended and the palm was facing to the lower limb. The dynamometer was placed proximal to the styloid process of the ulna at the level of the flexors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder internal rotators (subscapularis, pectoralis major, teres major, latisimus dorsi)
For MVIC of shoulder internal rotators, players lay in a supine position with the shoulder in 90° flexion, elbow was 90° flexed, and forearm in a neutral position. The dynamometer was placed exactly proximal to the styloid process of the ulna at the level of flexors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder abductors (supraspinatus, middle deltoid)
For MVIC of shoulder abductors, players lay in a supine position with the shoulder in 90° abduction, elbow fully extended, palm facing the lower limb. The dynamometer was placed proximal to the styloid process of the ulna at the level of extensors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder external rotators (infraspinatus, teres minor)
For MVIC of shoulder external rotators, players lay in a supine position with the shoulder in 90° flexion, and elbow was 90° flexed, and forearm in a neutral position. The handheld dynamometer was placed exactly proximal to the styloid process of the ulna and at the level of the extensors. The players were asked to apply force to the dynamometer similar to previous measurements [18, 19] (Figure 2).
Data analysis
All statistical analyses were performed by SPSS software, version 26. The significance level for all tests was set at a value of 0.05. The differences in the means and proportions were evaluated using t-test. Descriptive statistics included the mean and dispersion of the data, and analytical statistics included the Kolmogorov-Smirnov method to determine the normal distribution of the data. In the case of normal distribution of data, two-by-two correlation was measured with Pearson correlation.
Results
Table 1 shows the demographic data of the overhead thrower players.
According to Tables 2 and 3, the pain had a moderate negative relation with the isometric strength of all muscle groups.


The relationship between pain and the DASH score (function) and disability part of the SPADI and SF-36 was significant. Duration of the syndrome had no relationship with other parameters.
The strength of shoulder muscle groups on both sides showed that the MVIC of the healthy side is more than affected side and the strength of the internal rotators of the affected shoulder significantly decreased more than others. The MVIC of flexors of the healthy side was higher than the MVIC of other muscle groups.
The strength of all muscles had a high positive relation with other muscle groups. Also, it had a moderate positive relationship with quality of life (QoL), but a moderate negative relationship with the DASH questionnaire (function) and a low negative relation with SPADI questionnaire (pain and disability).
The DASH questionnaire had a high positive relationship with the SPADI questionnaire and its relationship with QoL was negative and high.
Also, the results of the SPADI questionnaire had a high negative relationship with QoL. It showed that the MVIC of male players was higher than female players. However, no significant difference was observed between men and women to compare the disability.
Based on the t-test, the MVIC of the flexors was higher than the MVIC of other muscles in the healthy side. However, the MVIC of abductors was lower than the MVIC of other muscle groups on the healthy side. Also, in the affected hand, the MVIC of the extensors was higher than MVIC of other muscle groups but the MVIC of the abductors was lower than MVIC of other muscles.
According to the average results of the DASH (function) questionnaire, the rate of decrease in function and disability between female players was higher than male players and the average results of the SPADI questionnaire demonstrated more pain and disability in men than in women. The results of the SF-36 questionnaire showed that the quality of both the physical and mental life of women is higher than that of men.
Discussion
In the past research, the relationship was two-by-two (the amount of pain with strength or pain with the amount of decreased range of motion, especially the decrease in the range of internal rotation) was investigated. However, in this focal research, several factors that were affected after this injury were investigated. Also, previous studies focused on other shoulder syndromes, such as subacromial syndrome.
Players’ function showed a very high and significant indirect relation with pain intensity. Also, the decrease in shoulder flexor muscle strength had the most relationship with the decrease in the function of players, and the decrease in the strength of shoulder extensor muscles had the least relation with the decrease of function in players. Also, it had a significant direct relationship with players’ QoL (physical and mental).
Pain is an unpleasant sensory and emotional experience, associated with tissue damage or tissue destruction [20]. It usually protects a person by preventing them from doing activities that may damage the tissue. The crucial concept is that pain is not a sign of tissue damage, but shows the brain’s belief that a particular tissue needs protection. The mechanisms of pain are divided into three categories of nociceptive, peripheral neuropathic, and central sensitivity. In this research, the pain of players with this syndrome was central sensitization and biopsychosocial [21].
According to this syndrome, increased response of nociceptors in the central nervous system to normal or subthreshold afferent input leads to hypersensitivity to stimuli. A pathophysiological process in which the central nervous system undergoes changes that alter the processing of pain and other sensory stimuli. This kind of pain often does not respond to medications [21].
Effect of pain on muscle strength
Muscle strength is the maximum force that muscles can generate at a determined speed. This ability of skeletal muscle to generate force is important for functional stability and mobility.
The relationship between pain and normal motor response is justified by pain adaptation theory.
This theory suggests facilitated and inhibited motor responses depending on their relationship to the painful area, partially combining the vicious cycle theory and the inhibition theory. It means agonist’s muscles show decreased activity, while antagonist’s muscles show increased muscle activity [22]. Lund et al. suggested that through a mechanism, nociceptive input converges on group II interneurons and leads to a decrease in muscle strength [23].
Disability refers to difficulty in performing tasks or activities of ADL. The patient cannot take care of him/herself. Shoulder pain in athletes caused a decrease in their muscle strength and disability and their participation in sport [24].
Function refers to the person’s ability to do tasks and activities at home, at work, in the community, and during recreational activities independently.
The international classification of functioning, disability and health (ICF) model, suggests a framework of function, disability, and health to help us for describing and organizing patient’s information about the function. It divides health-related information into two parts. First one contains function and disability, which is divided into two subsets, functions and structure of the body, activities and participations and activity limitations.
The second part includes factors that are divided into two components:, environmental factors, and personal factors [25].
A person’s level of function is a combination of dynamic interaction between his/her health conditions, environmental factors, and personal factors.
According to the international classification of functioning, disability and health (ICF) model, activity limitations take place whenever a person or player has difficulty performing activities or is unable to accomplish tasks or daily activities. Participation limitations are difficulties that a person may have in engaging in life situations [25].
The effect of QoL
Controlling pain plays a crucial role in QoL. Pain has a destructive influence on every aspect of a player’s life with this syndrome and it causes anxiety and emotional problems for athletes, negatively affects their general well-being, and caused problems for abilities related to family, society, and work. Therefore, it had negative impacts on their physical and mental QoL [26].
In a study by Sahinoglu et al. [27] all patients with unilateral rotator cuff injuries received a physical therapy program for 6 weeks. Finally, a weak relationship was observed between changes in the range of motion of abduction and the SPADI score. Also, a relationship was observed between changes in external rotation strength and the score of the SPADI questionnaire.
Almeida et al. [26] studied on patients with subacromial impingement syndrome. They reported that the strength of the muscles between the healthy and affected side is significantly different in all movements. Also, a significant indirect relationship between shoulder pain and function and isometric muscle strength of shoulder flexion and internal rotation and a significant direct relationship with the level of fear of movement.
Celik et al. [28] investigated the relationship between pain and upper, middle, lower trapezius, serratus anterior, supraspinatus, anterior deltoid muscle strengths bilaterally in patients with subacromial impingement syndrome. The strength of the middle trapezius, serratus anterior, supraspinatus, and anterior deltoid of the affected side was lower than the healthy side. A significant relationship was observed between pain and weakness of the middle trapezius, serratus anterior, and supraspinatus.
Gutierrez et al. [29] examined the relationship between shoulder pain and QoL, physical activities, and social activities in spinal cord injury patients. It showed a significant relationship between pain and QoL and physical activities but no relationship between pain and social activities was found.
This correlation study shows that in overhead players with this syndrome, to return to sports, pain must first be reduced. Then, special exercises should be done for strengthening shoulder muscles, particularly internal rotators, and enhancing function and QoL of the players and their activity and participation should be considered and prevention of returning to sports until the above conditions are met.
Conclusion
Players with this syndrome showed a negative relationship between pain and muscle strength of the symptomatic shoulder. A high negative relationship between pain and function and QoL was considerable. A positive relationship between muscle groups’ strength of the affected shoulder and function and QoL was palpable. Reduction in all muscle strengths of the affected shoulder in comparison with the asymptomatic side was observed. Therefore, a significant relationship was observed between pain, muscle strength, function, and QoL in overhead players with this syndrome.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Iran University of Medical Sciences (Code: IR.IUMS.REC.1401.340).
Funding
The paper is extracted from master's thesis of SeyedehPardis Emadi, approved by Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Soheil Mansour; Methodology: SeyedehPardis Emadi; Writing the original draft; SeyedehPardis Emadi and Reza Salehi; Investigation, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Shoulder pain has the third rank among other pains. Shoulder impingement syndrome is the most common disease of shoulder complaints among individuals. It is classified into three subsets, internal, subacromial, and subcoracoid impingement [1, 2].
These patients state pain during elevating the arm or lying on the painful shoulder [3]. The prevalence of this syndrome is estimated at about 44%–65% of all shoulder pain disorders [4]. This syndrome is one of the most common injuries happening in overhead throwers due to normal physiological contact between the posterosuperior glenoid and the greater tuberosity in repetitive hyperabduction and external rotation positions. This physiological contact can be symptomatic when repeated overhead motions result in partial articular-sided posterosuperior rotator cuff tears and lesions of the posterosuperior glenoid labrum, therefore, posterosuperior rotator cuff and labrum will be “pinched” in the space of greater tuberosity and the glenoid rim. This syndrome is multifactorial, such as shoulder physiological remodeling, contracture of the posterior capsule, and scapular dyskinesis. These factors cause shoulder pathologies like glenohumeral internal rotation deficit (GIRD), humeral hyper angulation, and superior labral anterior to posterior (SLAP) tears [5].
Jobe [6] and Walch et al. [7, 8] assert the mechanism of impingement syndrome as an entrapment between the greater tuberosity and glenoid labrum during shoulder abduction and lateral rotation in the interval between supraspinatus and infraspinatus tendons. Walch et al suggested that anterior glenohumeral (GH) laxity has an important role in this syndrome in overhead throwers [7].
This syndrome causes pain in the posterior of the shoulder and happens in the throwers usually during cocking phase of throwing or pitching in the GH joint, whether in excessive external rotation and horizontal abduction or in abduction and shoulder flexion. Other associated pathologies with this syndrome are labrum injury, rotator cuff tear; mostly infraspinatus muscle, greater tuberosity injury, Inferior glenohumeral ligament injury, GIRD, and scapular dyskinesis [9, 10].
According to Jobe’s categorization of the internal impingement syndrome into three stages regarding to patient’s symptoms and presentations, patients in the early stage complain of shoulder stiffness and required to warm–up longer but have no problem with activity daily livings [6]. During the intermediate stage, patients reported pain in the posterior side of the shoulder during the late phase of cocking and have no pain during activities of daily livings (ADLs). During the advanced stage, the patient’s symptoms are like an intermediate stage, but will not get better with rest and rehabilitation [11].
Materials and Methods
This is a correlation study that was conducted at a hospital in Tehran during the summer of 2023. Forty-seven participants (32 males, 15 females) overhead players (volleyball, basketball, badminton, bodybuilding, powerlifting, and swimming) with chronic shoulder internal impingement syndrome participated in this study. Players were tested by shoulder fellowship (orthopedic surgeon) and PhD in physiotherapy. Players entered by checking the inclusion and exclusion criteria and filling out the consent forms. Then, the pain was measured by a visual analogue scale (VAS). Muscle strength was measured by a handheld dynamometer (Imada design) with the ability to measure tensional strengths and a pressure capacity of 500 N, and a precision of 0.1 N (Figure 1).
Inclusion criteria
The inclusion criteria included 15 to 45-year-old male and female overhead throwers (elite, semi-professional, amateur) with chronic shoulder internal impingement [11, 12], players with no cortisone injection in the last 3 months [11], complaining reduction in ball speed, endurance and ball control during throwing [11, 12], and having the ability to read and write in Persian.
Exclusion criteria
The exclusion criteria included players with a history of neck, shoulder, elbow, and hand pain and injuries in the last 3 months, instability or dislocation of GH joint, undergoing neck and shoulder, elbow, and wrist surgeries last year, and player’s unwillingness to participate in this research [12].
Questionnaires
Disabilities of the arm, shoulder, and hand (DASH)
Persian form of DASH questionnaire was used to determine symptoms and degree of disability of musculoskeletal disorders of upper limbs. The severity of symptoms, pain, weakness and arm stiffness, function, work, and exercise were discussed. It was completed by players [13]. The scores were converted to percentages by computer program.
Shoulder pain and disability index (SPADI)
Persian form of SPADI questionnaire was used to measure shoulder pain and disability, disability, pain in different situations, and the ability of a person to perform ADL are discussed. It was completed by the players [14]. The scores were converted to percentages by computer program.
Short form (SF)-36
We used the Persian short form (SF)-36 with eight subgroups. Physical and mental aspects were discussed, which examines the pain, health status and its impact on ADL and social activities [15, 16]. The scores were converted to percentages by computer program.
Handheld dynamometer
It was used to measure the isometric strength of all shoulder muscles on both healthy and affected sides in Newton and players were asked to hold the maximal voluntary isometric contraction (MVIC) in the middle range for 3 s and rest 30 s between tests and contractions were asked for 3 times on both sides and the average of the contractions was calculated [17] (Figure 1).
Muscle tests MVIC
Shoulder flexors (anterior deltoid, biceps, coracobrachialis)
For MVIC of shoulder flexors, players lay in a supine position with shoulder 90° flexion, elbow extension, and the palm faced to the lower limb. It was placed exactly proximal to the styloid process of the ulna at the level of the extensors. Players were asked to apply force to the dynamometer for 3 s in the direction of shoulder flexion, and after each contraction, they rested for 30 s, we considered the average contractions of both shoulder sides [18] (Figure 2).
Shoulder extensors (latisimus dorsi, teres major, posterior deltoid)
For MVIC of shoulder extensors, players lay in a supine position with shoulder 90° flexion, and elbow was completely extended and the palm was facing to the lower limb. The dynamometer was placed proximal to the styloid process of the ulna at the level of the flexors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder internal rotators (subscapularis, pectoralis major, teres major, latisimus dorsi)
For MVIC of shoulder internal rotators, players lay in a supine position with the shoulder in 90° flexion, elbow was 90° flexed, and forearm in a neutral position. The dynamometer was placed exactly proximal to the styloid process of the ulna at the level of flexors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder abductors (supraspinatus, middle deltoid)
For MVIC of shoulder abductors, players lay in a supine position with the shoulder in 90° abduction, elbow fully extended, palm facing the lower limb. The dynamometer was placed proximal to the styloid process of the ulna at the level of extensors. Players were asked to apply force to the dynamometer similar to previous measurements [18] (Figure 2).
Shoulder external rotators (infraspinatus, teres minor)
For MVIC of shoulder external rotators, players lay in a supine position with the shoulder in 90° flexion, and elbow was 90° flexed, and forearm in a neutral position. The handheld dynamometer was placed exactly proximal to the styloid process of the ulna and at the level of the extensors. The players were asked to apply force to the dynamometer similar to previous measurements [18, 19] (Figure 2).
Data analysis
All statistical analyses were performed by SPSS software, version 26. The significance level for all tests was set at a value of 0.05. The differences in the means and proportions were evaluated using t-test. Descriptive statistics included the mean and dispersion of the data, and analytical statistics included the Kolmogorov-Smirnov method to determine the normal distribution of the data. In the case of normal distribution of data, two-by-two correlation was measured with Pearson correlation.
Results
Table 1 shows the demographic data of the overhead thrower players.
According to Tables 2 and 3, the pain had a moderate negative relation with the isometric strength of all muscle groups.
The relationship between pain and the DASH score (function) and disability part of the SPADI and SF-36 was significant. Duration of the syndrome had no relationship with other parameters.
The strength of shoulder muscle groups on both sides showed that the MVIC of the healthy side is more than affected side and the strength of the internal rotators of the affected shoulder significantly decreased more than others. The MVIC of flexors of the healthy side was higher than the MVIC of other muscle groups.
The strength of all muscles had a high positive relation with other muscle groups. Also, it had a moderate positive relationship with quality of life (QoL), but a moderate negative relationship with the DASH questionnaire (function) and a low negative relation with SPADI questionnaire (pain and disability).
The DASH questionnaire had a high positive relationship with the SPADI questionnaire and its relationship with QoL was negative and high.
Also, the results of the SPADI questionnaire had a high negative relationship with QoL. It showed that the MVIC of male players was higher than female players. However, no significant difference was observed between men and women to compare the disability.
Based on the t-test, the MVIC of the flexors was higher than the MVIC of other muscles in the healthy side. However, the MVIC of abductors was lower than the MVIC of other muscle groups on the healthy side. Also, in the affected hand, the MVIC of the extensors was higher than MVIC of other muscle groups but the MVIC of the abductors was lower than MVIC of other muscles.
According to the average results of the DASH (function) questionnaire, the rate of decrease in function and disability between female players was higher than male players and the average results of the SPADI questionnaire demonstrated more pain and disability in men than in women. The results of the SF-36 questionnaire showed that the quality of both the physical and mental life of women is higher than that of men.
Discussion
In the past research, the relationship was two-by-two (the amount of pain with strength or pain with the amount of decreased range of motion, especially the decrease in the range of internal rotation) was investigated. However, in this focal research, several factors that were affected after this injury were investigated. Also, previous studies focused on other shoulder syndromes, such as subacromial syndrome.
Players’ function showed a very high and significant indirect relation with pain intensity. Also, the decrease in shoulder flexor muscle strength had the most relationship with the decrease in the function of players, and the decrease in the strength of shoulder extensor muscles had the least relation with the decrease of function in players. Also, it had a significant direct relationship with players’ QoL (physical and mental).
Pain is an unpleasant sensory and emotional experience, associated with tissue damage or tissue destruction [20]. It usually protects a person by preventing them from doing activities that may damage the tissue. The crucial concept is that pain is not a sign of tissue damage, but shows the brain’s belief that a particular tissue needs protection. The mechanisms of pain are divided into three categories of nociceptive, peripheral neuropathic, and central sensitivity. In this research, the pain of players with this syndrome was central sensitization and biopsychosocial [21].
According to this syndrome, increased response of nociceptors in the central nervous system to normal or subthreshold afferent input leads to hypersensitivity to stimuli. A pathophysiological process in which the central nervous system undergoes changes that alter the processing of pain and other sensory stimuli. This kind of pain often does not respond to medications [21].
Effect of pain on muscle strength
Muscle strength is the maximum force that muscles can generate at a determined speed. This ability of skeletal muscle to generate force is important for functional stability and mobility.
The relationship between pain and normal motor response is justified by pain adaptation theory.
This theory suggests facilitated and inhibited motor responses depending on their relationship to the painful area, partially combining the vicious cycle theory and the inhibition theory. It means agonist’s muscles show decreased activity, while antagonist’s muscles show increased muscle activity [22]. Lund et al. suggested that through a mechanism, nociceptive input converges on group II interneurons and leads to a decrease in muscle strength [23].
Disability refers to difficulty in performing tasks or activities of ADL. The patient cannot take care of him/herself. Shoulder pain in athletes caused a decrease in their muscle strength and disability and their participation in sport [24].
Function refers to the person’s ability to do tasks and activities at home, at work, in the community, and during recreational activities independently.
The international classification of functioning, disability and health (ICF) model, suggests a framework of function, disability, and health to help us for describing and organizing patient’s information about the function. It divides health-related information into two parts. First one contains function and disability, which is divided into two subsets, functions and structure of the body, activities and participations and activity limitations.
The second part includes factors that are divided into two components:, environmental factors, and personal factors [25].
A person’s level of function is a combination of dynamic interaction between his/her health conditions, environmental factors, and personal factors.
According to the international classification of functioning, disability and health (ICF) model, activity limitations take place whenever a person or player has difficulty performing activities or is unable to accomplish tasks or daily activities. Participation limitations are difficulties that a person may have in engaging in life situations [25].
The effect of QoL
Controlling pain plays a crucial role in QoL. Pain has a destructive influence on every aspect of a player’s life with this syndrome and it causes anxiety and emotional problems for athletes, negatively affects their general well-being, and caused problems for abilities related to family, society, and work. Therefore, it had negative impacts on their physical and mental QoL [26].
In a study by Sahinoglu et al. [27] all patients with unilateral rotator cuff injuries received a physical therapy program for 6 weeks. Finally, a weak relationship was observed between changes in the range of motion of abduction and the SPADI score. Also, a relationship was observed between changes in external rotation strength and the score of the SPADI questionnaire.
Almeida et al. [26] studied on patients with subacromial impingement syndrome. They reported that the strength of the muscles between the healthy and affected side is significantly different in all movements. Also, a significant indirect relationship between shoulder pain and function and isometric muscle strength of shoulder flexion and internal rotation and a significant direct relationship with the level of fear of movement.
Celik et al. [28] investigated the relationship between pain and upper, middle, lower trapezius, serratus anterior, supraspinatus, anterior deltoid muscle strengths bilaterally in patients with subacromial impingement syndrome. The strength of the middle trapezius, serratus anterior, supraspinatus, and anterior deltoid of the affected side was lower than the healthy side. A significant relationship was observed between pain and weakness of the middle trapezius, serratus anterior, and supraspinatus.
Gutierrez et al. [29] examined the relationship between shoulder pain and QoL, physical activities, and social activities in spinal cord injury patients. It showed a significant relationship between pain and QoL and physical activities but no relationship between pain and social activities was found.
This correlation study shows that in overhead players with this syndrome, to return to sports, pain must first be reduced. Then, special exercises should be done for strengthening shoulder muscles, particularly internal rotators, and enhancing function and QoL of the players and their activity and participation should be considered and prevention of returning to sports until the above conditions are met.
Conclusion
Players with this syndrome showed a negative relationship between pain and muscle strength of the symptomatic shoulder. A high negative relationship between pain and function and QoL was considerable. A positive relationship between muscle groups’ strength of the affected shoulder and function and QoL was palpable. Reduction in all muscle strengths of the affected shoulder in comparison with the asymptomatic side was observed. Therefore, a significant relationship was observed between pain, muscle strength, function, and QoL in overhead players with this syndrome.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Iran University of Medical Sciences (Code: IR.IUMS.REC.1401.340).
Funding
The paper is extracted from master's thesis of SeyedehPardis Emadi, approved by Department of Physiotherapy, School of Rehabilitation, Iran University of Medical Sciences.
Authors' contributions
Conceptualization and supervision: Soheil Mansour; Methodology: SeyedehPardis Emadi; Writing the original draft; SeyedehPardis Emadi and Reza Salehi; Investigation, review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Horowitz EH, Aibinder WR. Shoulder Impingement syndrome. Physical Medicine and Rehabilitation Clinics of North America. 2023; 34(2):311-34. [DOI:10.1016/j.pmr.2022.12.001] [PMID]
- Nazari G, MacDermid JC, Bryant D, Athwal GS. The effectiveness of surgical vs conservative interventions on pain and function in patients with shoulder impingement syndrome. A systematic review and meta-analysis. PLoS One. 2019; 14(5):e0216961. [DOI:10.1371/journal.pone.0216961] [PMID]
- Garving C, Jakob S, Bauer I, Nadjar R, Brunner UH. Impingement Syndrome of the shoulder. Deutsches Arzteblatt international. 2017; 114(45):765-76. [DOI:10.3238/arztebl.2017.0765] [PMID]
- De Yang Tien J, Tan AHC. Shoulder Impingement syndrome, a common Affliction of the shoulder: A comprehensive review. Proceedings of Singapore Healthcare. 2014; 23(4):297-305. [DOI:10.1177/201010581402300406]
- Spiegl UJ, Warth RJ, Millett PJ. Symptomatic internal impingement of the shoulder in overhead athletes. Sports Medicine and Arthroscopy Review. 2014; 22(2):120-9. [DOI:10.1097/JSA.0000000000000017] [PMID]
- Jobe C. Superior glenoid impingement: Current concepts. Clinical Orthopaedics and Related Research. 1996; 330:98-107. [DOI:10.1097/00003086-199609000-00012]
- Walch G, Boileau P, Noel E, Donell ST. Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. Journal of Shoulder and Elbow Surgery. 1992; 1(5):238-45. [DOI:10.1016/S1058-2746(09)80065-7] [PMID]
- Walch G, Liotard JP, Boileau P, Noël E. [Postero-superior glenoid impingement. Another impingement of the shoulder (French)]. Journal of Radiology. 1993; 74(1):47-50. [Link]
- Cools AM, Declercq G, Cagnie B, Cambier D, Witvrouw E. Internal impingement in the tennis player: Rehabilitation guidelines. British Journal of Sports Medicine. 2008; 42(3):165-71. [DOI:10.1136/bjsm.2007.036830] [PMID]
- Manske RC, Grant-Nierman M, Lucas B. Shoulder posterior internal impingement in the overhead athlete. International Journal of Sports Physical Therapy. 2013; 8(2):194-204. [PMID]
- Halbrecht JL, Tirman P, Atkin D. Internal impingement of the shoulder: Comparison of findings between the throwing and nonthrowing shoulders of college baseball players. Arthroscopy: The Journal of Arthroscopic & Related Surgery: Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 1999; 15(3):253-8. [DOI:10.1016/S0749-8063(99)70030-7] [PMID]
- Burkhart SS. Internal impingement of the shoulder. Instructional Course Lectures. 2006; 55:29-34. [PMID]
- Mousavi SJ, Parnianpour M, Abedi M, Askary-Ashtiani A, Karimi A, Khorsandi A, et al. Cultural adaptation and validation of the Persian version of the Disabilities of the Arm, Shoulder and Hand (DASH) outcome measure. Clinical Rehabilitation. 2008; 22(8):749-57. [DOI:10.1177/0269215508085821] [PMID]
- Ebrahimzadeh MH, Birjandinejad A, Golhasani F, Moradi A, Vahedi E, Kachooei AR. Cross-cultural adaptation, validation, and reliability testing of the Shoulder Pain and Disability Index in the Persian population with shoulder problems. International Journal of Rehabilitation Research. 2015; 38(1):84-7. [DOI:10.1097/MRR.0000000000000088] [PMID]
- Ware JE, Kosinsk M, Keller Keller SD. SF-36 physical and mental health summary scales: A user’s manual. Boston: Health Institute, New England Medical Center; 1994. [Link]
- Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): Translation and validation study of the Iranian version. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation. 2005;14(3):875-82. [DOI:10.1007/s11136-004-1014-5] [PMID]
- Meldrum D, Cahalane E, Conroy R, Fitzgerald D, Hardiman O. Maximum voluntary isometric contraction: Reference values and clinical application. Amyotrophic Lateral Sclerosis: Official Publication of the World Federation of Neurology Research Group on Motor Neuron Diseases. 2007; 8(1):47-55. [DOI:10.1080/17482960601012491] [PMID]
- University of Delaware. Rehab guidelines & protocols shoulder [internet]. 2024. [Updated May 2024]. Available from: [Link]
- Committee on Pain, Disability, and Chronic Illness Behavior. Pain and disability clinical, behavioral, and public policy perspectives. Washington (DC): National Academies Press; 1987. [Link]
- Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet (London, England). 2021; 397(10289):2098-110. [DOI:10.1016/S0140-6736(21)00392-5] [PMID]
- Merkle SL, Sluka KA, Frey-Law LA. The interaction between pain and movement. Journal of Hand Therapy: Official Journal of the American Society of Hand Therapists. 2020; 33(1):60-6. [DOI:10.1016/j.jht.2018.05.001] [PMID]
- Parks KA, Crichton KS, Goldford RJ, McGill SM. A comparison of lumbar range of motion and functional ability scores in patients with low back pain: Assessment for range of motion validity. Spine. 2003; 28(4):380-4. [DOI:10.1097/00007632-200302150-00014] [PMID]
- Lund JP, Donga R, Widmer CG, Stohler CS. The pain-adaptation model: A discussion of the relationship between chronic musculoskeletal pain and motor activity. Canadian Journal of Physiology and Pharmacology. 1991; 69(5):683-94. [DOI:10.1139/y91-102] [PMID]
- Kisner C, Colby LA, Borstad J. Therapeutic exercise, Foundations and techniques. Philadelphia: F.A. Davis Company; 2018. [Link]
- Soyuer F, Varol BK. Quality of life and pain. International Journal of Family & Community Medicine. 2019; 3(3):110-4. [DOI:10.15406/ijfcm.2019.03.00140]
- Almeida EPD, Salgasso ME, Oliveira ASD, Libardoni TDC. Comparison of isometric muscle strength between painful and non-painful shoulders in patients with symptoms of subacromial impingement. Brazilian Journal of Pain. 2021; 3(4):305-9. [DOI:10.5935/2595-0118.20200201]
- Şahinoğlu E, Ünver B, Yamak K. The relationship of range of motion and muscle strength to patients’ perspectives in pain, disability, and health-related quality of life in patients with rotator cuff disease. Irish Journal of Medical Science. 2021; 190(1):177-83. [DOI:10.1007/s11845-020-02305-4] [PMID]
- Celik D, Sirmen B, Demirhan M. The relationship of muscle strength and pain in subacromial impingement syndrome. Acta Orthopaedica et Traumatologica Turcica. 2011; 45(2):79-84. [DOI:10.3944/AOTT.2011.2425] [PMID]
- Gutierrez DD, Thompson L, Kemp B, Mulroy SJ. The relationship of shoulder pain intensity to quality of life, physical activity, and community participation in persons with paraplegia. The Journal of Spinal Cord Medicine. 2007; 30(3):251-5. [DOI:10.1080/10790268.2007.11753933] [PMID]
Type of Study: Case Study |
Subject:
Physiotherapy
Received: 2024/02/12 | Accepted: 2024/03/11 | Published: 2024/03/21
Received: 2024/02/12 | Accepted: 2024/03/11 | Published: 2024/03/21
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.