

Volume 7, Issue 1 (Continuously Updated 2024)
Func Disabil J 2024, 7(1): 0-0 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moradi F, Azadi F, Vahedi M. Cross-culturally Adaptation, Validity, and Reliability of the Persian Version of the Constipation-related Disability Scale. Func Disabil J 2024; 7 (1) : 259.1
URL: http://fdj.iums.ac.ir/article-1-227-en.html
URL: http://fdj.iums.ac.ir/article-1-227-en.html



1- Department of Physical Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physical Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,fa.azadi@uswr.ac.ir
3- Iranian Research Center on Aging, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physical Therapy, School of Rehabilitation Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Iranian Research Center on Aging, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 1105 kb]
(512 Downloads)
| Abstract (HTML) (1039 Views)
Full-Text: (243 Views)
Introduction
Constipation is one of the most prevalent gastrointestinal tract diseases, especially in developed countries [1]. While constipation is often seen as harmless and can be cured with minimal treatment, chronic constipation can create various complications, from mild to severe disability, that require medical attention [2]. Functional constipation occurs when incoordination exists between the relaxation of the pelvic floor muscles, especially the puborectalis muscles, and the contractions of the abdominal wall muscles essential for normal defecation [3]. Constipation is diagnosed based on the Rome IV diagnostic criteria [4].
Chronic functional constipation (CFC) affects both genders of all age groups in the general population, with a prevalence of up to 27%. However, it is more common in females, older people, and low socioeconomic class [5, 6]. In the future, the prevalence of constipation patients may increase due to the recent changes in people’s lifestyles and inactivity [7, 8].
Constipation also imposes a significant economic burden on the patient and society. This burden is partly related to using resources for outpatient visits, hospitalization, laboratory tests, the cost of medicines, and the reduction of people’s work productivity due to constipation [9].
CFC seriously impacts the quality of life (QoL) and performing daily activities [10]. Reducing physical activity is associated with many illnesses, such as diabetes, high blood pressure, obesity, osteoporosis, heart and vascular diseases, breast and colon cancer, depression, and anxiety [11].
Evaluating the disabilities caused by constipation is crucial in order to manage the treatment effectively and reduce complications and disabilities. Physiotherapy plays a significant part in this regard [12].
Several tools have been devised to evaluate the effects of constipation on the QoL. However, the constipation-related disability scale (CRDS) stands out as the most effective tool for evaluating the impact of constipation on daily activities [2]. It is a more comprehensive assessment tool compared to previous questionnaires like PAC-QOL (patient assessment of constipation QoL) [13] and PAC-SYM (patient assessment of constipation symptoms) [14, 1].
The original version of CRDS was reviewed and developed in Canada and English. Although strong evidence supports the validity and reliability of this questionnaire, due to the cultural and linguistic differences in different societies, it is recommended to use valid culturally-adapted tools [15]. Therefore, the cultural adaptation of the CRDS in the Persian-speaking population can facilitate the comparison of research findings in different clinical conditions.
To address this matter, the current research aims to develop the Persian version of the CRDS and compare its psychometric properties with the original version. The study outcomes will provide valuable insights for assessing different interventions’ effectiveness in clinical and research settings.
Materials and Methods
This methodological study was conducted on a group of Iranian individuals diagnosed with CFC, based on the Rome IV criteria, to assess the reliability and validity of the Persian version of CRDS. The participants were recruited from public and private hospitals and gastroenterology and colorectal physician offices in Arak City, Iran, from April 2022 to August 2022. The study sampling method was purposive. The sample included 145 patients who met the inclusion criteria: Being ≥18 years old, fulfilling the Rome IV criteria for chronic functional constipation, and having the ability to read and speak Persian [15]. The exclusion criteria were as follows: Having secondary constipation, suffering from any systemic disease and psychological disorders, undertaking previous pelvic surgery, and lacking the mental disability to complete the questionnaire [16].
To assess the discriminant validity of the Persian version of CRDS, 130 healthy individuals were selected to participate. These healthy volunteers were recruited through ads, and to be eligible for participation, the healthy subjects were required to be at least 18 years old and proficient in speaking and reading Persian.
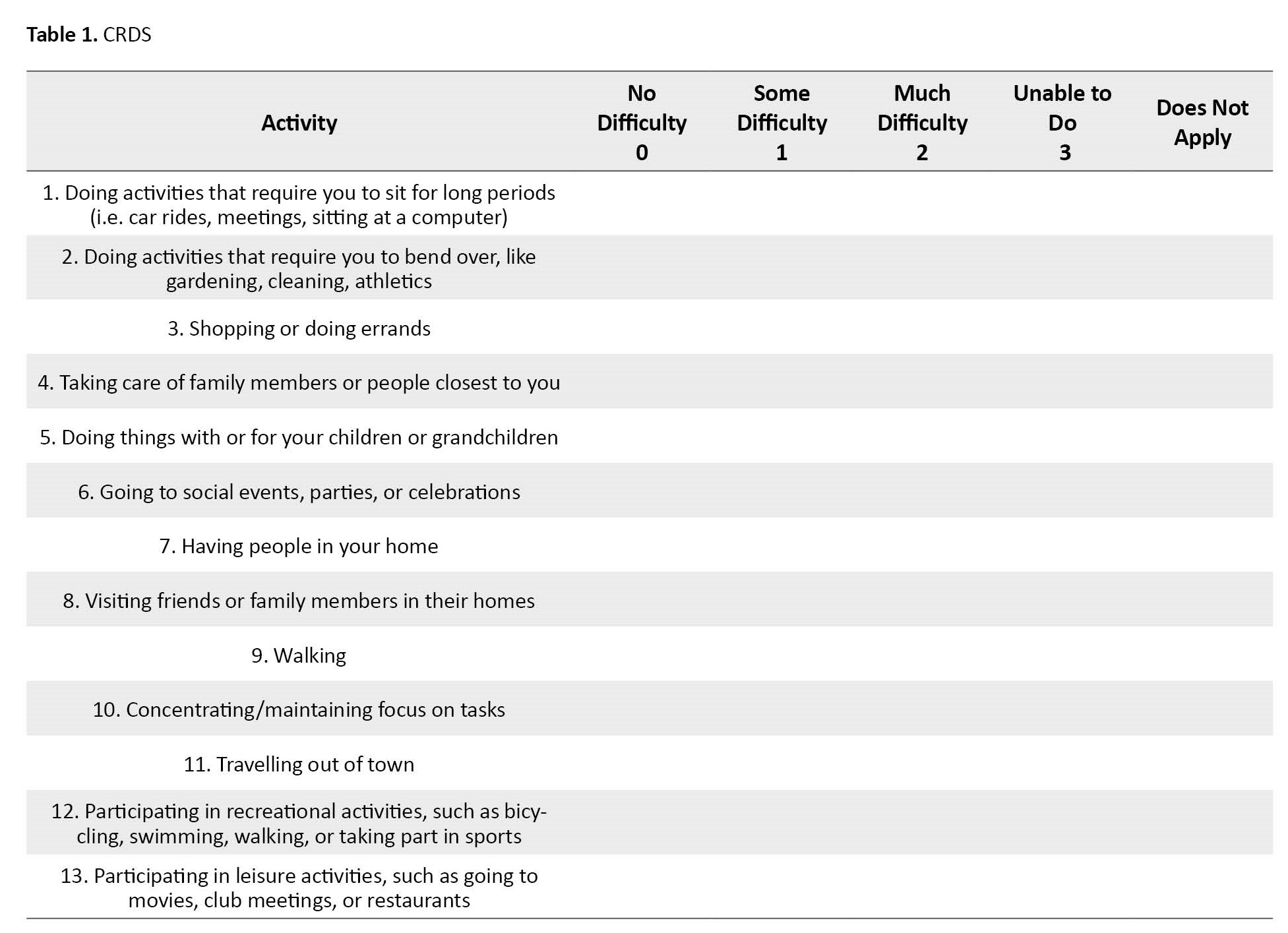
This questionnaire consists of 13 items in two subscales: Work/leisure activities (7 items) and daily life activities (6 items). The items are scored on a 4-point Likert scale, ranging from 0 (no difficulty) to 3 (unable to do). Additionally, a fifth response option called ‘does not apply’ was included for activities that participants did not do due to reasons unrelated to their bowel problems. These items were not considered in the scoring process (Table 1).
Cultural adaptation
At first, permission to translate the questionnaire into Persian was obtained from its authors. In this study, the cultural adaptation of the CRDS questionnaire to the Persian language was carried out according to the international QoL assessment (IQOLA) project presented by Bollinger et al. The project includes the following steps: Translation of the original version into Persian, evaluation of the quality of the translation, back-translating the Persian version into English, comparing the English back-translation with the original version, and assessing the conceptual consistency between the two. Adjustments will be made to the English-translated version if needed [17].
To qualitatively examine face validity, we gave the Persian version to 15 patients with CFC, who were asked to read the items and express their understanding to the researcher. They were also asked about their comprehension, ability to answer the questions, and appearance and arrangement of the questionnaire items. Considering the patients’ understanding of the questions, amendments were made to the questionnaire’s text to make the items clear and understandable. For example, in the translation of item number 4, the word “care” was replaced with “nursing” to better convey the concept to the patients.
After applying the changes, we submitted the revised English version of the questionnaire to the questionnaire authors for their approval. They reviewed and approved it, ensuring it maintained conceptual compatibility with the original version.
Reliability
The internal consistency of the tool was assessed through a reliability test using the Cronbach α coefficient. A coefficient value equal to or greater than 0.7 was deemed acceptable [18, 19].
To evaluate the test re-test reliability, 30 patients completed the questionnaire again two weeks later, while they had not received any new treatment for their constipation symptoms and had not changed their diet and nutrition. Also, the intra-class correlation coefficient was calculated as 0.8 to 1.0, indicating its perfect reproducibility [20].
Validity
The translated version was offered to 5 gastroenterologists or internists to assess the acceptance and content validity. Then, the content validity ratio and index were calculated.
We used the physical health composite of the medical outcomes study short form-36 (SF-36) to establish convergent validity for the CRDS due to its association with reduced QoL caused by disease-related disability [2]. A total of 145 patients were given the final Persian version of the CRDS. Additionally, they were asked to complete the SF-36, which consists of 36 questions assessing the overall health of individuals. These 36 items have 8 subscales: Physical functioning, role-physical, bodily pain, general health (physical health composite), vitality, social functioning, role-emotional, and mental health (mental health composite). The Persian version of the SF-36 was translated and culturally adapted by Montazeri et al. [21]. It was assessed by measuring the Pearson correlation coefficient (r) between the CRDS total score and the scores of the physical health section of SF-36.
To evaluate the discriminant validity questionnaire, 130 healthy people also completed it. Then, an independent t-test was used to check the difference between constipated patients and healthy groups.
A committee of 8 gastroenterologists and internists evaluated the instrument’s content validity. Content validity ensures the instrument contains appropriate examples to demonstrate the desired structure. Each expert provided a score of 1 to 3 for each question (1=necessary, 2=useful but not necessary, 3=not necessary). The content validity ratio was then calculated. With 8 experts, a minimum acceptable item content validity ratio of approximately 0.75 was established [22]. Additionally, each question was evaluated by experts on a scale of 1 to 4, with 1 indicating no relevance, 2 indicating relevance but requiring significant revisions, 3 indicating some need for revision, and 4 indicating close relevance. Subsequently, the content validity index for each item was computed, whose value exceeding 0.78 signifies strong content validity [23]. The effect of a ceiling or flooring was also evaluated. If more than 15% of the participants attained the maximum or minimum score, it confirms a ceiling or flooring effect.
Results
Participants
This study involved the participation of 145 patients suffering from CFC; 86(59.3%) were women, and 59(40.7%) were men. The mean age of men and women was 49.05 years (30 to 73 years) and 46.88 years (range: 32 to 72 years), respectively.
Also, 130 healthy people completed the questionnaire; 82(63%) were women, and 43(37%) were men, and their Mean±SD age was 39.83±12.74.
Reliability
The reliability of the Persian version of CRDS was assessed by internal consistency and reproducibility measures.
We calculated the Cronbach α value to analyze the internal consistency and found the reliability of the CRDS questionnaire. The Cronbach α coefficients for all items of the CRDS, as well as the work/leisure activities subscale and the ADL subscale, were 0.86, 0.77, and 0.75, respectively. These results indicate a high level of internal consistency for the CRDS questionnaire.
We calculated the intra-class correlation coefficient to determine the reproducibility of the CRDS. This coefficient value for the total scale score of the CRDS was 0.98 (95% CI, 0.92%, 0.96%) (Table 2).

The coefficient values for the work/leisure activities subscale and the ADL subscale were 0.92 and 0.96, respectively.
Validity
An independent t-test was conducted to evaluate the discriminant validity of CRDS. The results revealed a significant difference between the healthy and patient groups in the scores obtained. Specifically, the constipated sample had a higher CRDS total score (Mean±SD 25.60±2.71) compared to the healthy controls (Mean±SD 4.02±3.6), t (273)=- 55.62, P<0.001. This finding suggests that CRDS can distinguish between the two groups effectively.
Furthermore, the total score and subscales of CRDS were found to be significantly correlated with the physical health composite score of SF-36 (R=-0.84 to -0.89, P<0.001) (Table 3).

This result indicates that individuals with higher levels of disability tend to have lower ratings of QoL.
Regarding content validity, the Lawshe content validity ratio for all items of the Persian CRDS was higher than 0.75, and the CVI for all items of the Persian CRDS was higher than 0.78. There was no ceiling/floor effect for the total score of the Persian CRDS and its subscales.
Discussion
The study results prove the reliability and validity of the Persian version of the CRDS to measure constipation’s impact on Iranian people’s daily activities. Although cross-cultural validity studies are challenging, they yield precious results. The provision of standard health tools enables the comparison of health status between countries. It provides reliable measurements to monitor health at the population level, estimate the disease burden, examine the consequences in clinical performance, and evaluate the therapeutic outcomes.
In this questionnaire, disability questions were simple and understandable. It makes it easy for people with a low literacy level, who comprise the most affected people, to complete the questionnaire. All patients completed all items of the Persian version of the CRDS, and no item was left unanswered. This high level of responsiveness indicates the patients’ good understanding of the questions, a sign of the acceptability of the Persian translation in this study.
A similar study [24] suggests that it is better to consider the type of chronic constipation and its cause in affected people because irritable bowel syndrome can also lead to chronic constipation. This syndrome results from the interaction between the brain and the intestine. The irritable bowel syndrome causes disability and affects people’s QoL differently. Thus, for the sake of homogeneity of the studied sample, patients with irritable bowel syndrome were excluded from the study, and only people with chronic functional constipation remained.
The Cronbach α and intra-class correlation coefficient values for the Persian version of CRDS and its subscales were lower than the English version, which can be due to the countries’ cultural differences and the translation and cultural adaptation processes. However, Cronbach α values in this study are also good and acceptable, which indicates good internal consistency of the Persian version of this questionnaire.
The intra-class correlation coefficient was measured by test re-test reliability over time. The coefficient value varies from 1 (the highest level of reliability) to 0 (the lowest level of reliability). Based on the findings of the statistical tests, the repeatability of the overall scores of the questionnaire and the subscales were 0.98, 0.92, and 0.96, respectively. According to the study of Hart et al. [2], the values are 0.88 and 0.87, respectively, and in both studies, the intra-class correlation coefficient values were greater than 0.85, indicating the good internal consistency of the questionnaire.
The correlation between the CRDS and SF-36 questionnaire scores was investigated to check the convergent validity. The Pearson correlation coefficient between the total score of the CRDS questionnaire and its subscales with the total score of the physical health composite of the SF-36 questionnaire was between -0.84 and -0.89 (high correlation). This coefficient has been obtained in a previous study [2] between -0.31 and -0.53 (moderate correlation). The reason for the lower correlation values in the English study is the separation of the subscales of the physical health composite of the SF-36 questionnaire. However, in this study, the total score from the physical health composite of the SF-36 questionnaire was considered, and its correlation with the total score of the CRDS questionnaire and its subscales was investigated. Negative correlation values indicate that higher levels of disability in people are associated with lower QoL.
This research’s limitations were related to the coronavirus disease and the need to gain the participants’ trust. It is suggested that in future studies, responsiveness could also be assessed and calculated, and the relationship between the CRDS questionnaire and the severity of constipation should be investigated.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the University of Social Welfare and Rehabilitation (Code:IR.USWR.REC.1400.338).
Funding
The research was not funded by any specific grants from public, commercial, or not-for-profit sectors.
Authors' contributions
All authors equally contributed to the preparation of all aspects of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank doctors and samples who helped in conducting this research.
References
Constipation is one of the most prevalent gastrointestinal tract diseases, especially in developed countries [1]. While constipation is often seen as harmless and can be cured with minimal treatment, chronic constipation can create various complications, from mild to severe disability, that require medical attention [2]. Functional constipation occurs when incoordination exists between the relaxation of the pelvic floor muscles, especially the puborectalis muscles, and the contractions of the abdominal wall muscles essential for normal defecation [3]. Constipation is diagnosed based on the Rome IV diagnostic criteria [4].
Chronic functional constipation (CFC) affects both genders of all age groups in the general population, with a prevalence of up to 27%. However, it is more common in females, older people, and low socioeconomic class [5, 6]. In the future, the prevalence of constipation patients may increase due to the recent changes in people’s lifestyles and inactivity [7, 8].
Constipation also imposes a significant economic burden on the patient and society. This burden is partly related to using resources for outpatient visits, hospitalization, laboratory tests, the cost of medicines, and the reduction of people’s work productivity due to constipation [9].
CFC seriously impacts the quality of life (QoL) and performing daily activities [10]. Reducing physical activity is associated with many illnesses, such as diabetes, high blood pressure, obesity, osteoporosis, heart and vascular diseases, breast and colon cancer, depression, and anxiety [11].
Evaluating the disabilities caused by constipation is crucial in order to manage the treatment effectively and reduce complications and disabilities. Physiotherapy plays a significant part in this regard [12].
Several tools have been devised to evaluate the effects of constipation on the QoL. However, the constipation-related disability scale (CRDS) stands out as the most effective tool for evaluating the impact of constipation on daily activities [2]. It is a more comprehensive assessment tool compared to previous questionnaires like PAC-QOL (patient assessment of constipation QoL) [13] and PAC-SYM (patient assessment of constipation symptoms) [14, 1].
The original version of CRDS was reviewed and developed in Canada and English. Although strong evidence supports the validity and reliability of this questionnaire, due to the cultural and linguistic differences in different societies, it is recommended to use valid culturally-adapted tools [15]. Therefore, the cultural adaptation of the CRDS in the Persian-speaking population can facilitate the comparison of research findings in different clinical conditions.
To address this matter, the current research aims to develop the Persian version of the CRDS and compare its psychometric properties with the original version. The study outcomes will provide valuable insights for assessing different interventions’ effectiveness in clinical and research settings.
Materials and Methods
This methodological study was conducted on a group of Iranian individuals diagnosed with CFC, based on the Rome IV criteria, to assess the reliability and validity of the Persian version of CRDS. The participants were recruited from public and private hospitals and gastroenterology and colorectal physician offices in Arak City, Iran, from April 2022 to August 2022. The study sampling method was purposive. The sample included 145 patients who met the inclusion criteria: Being ≥18 years old, fulfilling the Rome IV criteria for chronic functional constipation, and having the ability to read and speak Persian [15]. The exclusion criteria were as follows: Having secondary constipation, suffering from any systemic disease and psychological disorders, undertaking previous pelvic surgery, and lacking the mental disability to complete the questionnaire [16].
To assess the discriminant validity of the Persian version of CRDS, 130 healthy individuals were selected to participate. These healthy volunteers were recruited through ads, and to be eligible for participation, the healthy subjects were required to be at least 18 years old and proficient in speaking and reading Persian.
This questionnaire consists of 13 items in two subscales: Work/leisure activities (7 items) and daily life activities (6 items). The items are scored on a 4-point Likert scale, ranging from 0 (no difficulty) to 3 (unable to do). Additionally, a fifth response option called ‘does not apply’ was included for activities that participants did not do due to reasons unrelated to their bowel problems. These items were not considered in the scoring process (Table 1).
Cultural adaptation
At first, permission to translate the questionnaire into Persian was obtained from its authors. In this study, the cultural adaptation of the CRDS questionnaire to the Persian language was carried out according to the international QoL assessment (IQOLA) project presented by Bollinger et al. The project includes the following steps: Translation of the original version into Persian, evaluation of the quality of the translation, back-translating the Persian version into English, comparing the English back-translation with the original version, and assessing the conceptual consistency between the two. Adjustments will be made to the English-translated version if needed [17].
To qualitatively examine face validity, we gave the Persian version to 15 patients with CFC, who were asked to read the items and express their understanding to the researcher. They were also asked about their comprehension, ability to answer the questions, and appearance and arrangement of the questionnaire items. Considering the patients’ understanding of the questions, amendments were made to the questionnaire’s text to make the items clear and understandable. For example, in the translation of item number 4, the word “care” was replaced with “nursing” to better convey the concept to the patients.
After applying the changes, we submitted the revised English version of the questionnaire to the questionnaire authors for their approval. They reviewed and approved it, ensuring it maintained conceptual compatibility with the original version.
Reliability
The internal consistency of the tool was assessed through a reliability test using the Cronbach α coefficient. A coefficient value equal to or greater than 0.7 was deemed acceptable [18, 19].
To evaluate the test re-test reliability, 30 patients completed the questionnaire again two weeks later, while they had not received any new treatment for their constipation symptoms and had not changed their diet and nutrition. Also, the intra-class correlation coefficient was calculated as 0.8 to 1.0, indicating its perfect reproducibility [20].
Validity
The translated version was offered to 5 gastroenterologists or internists to assess the acceptance and content validity. Then, the content validity ratio and index were calculated.
We used the physical health composite of the medical outcomes study short form-36 (SF-36) to establish convergent validity for the CRDS due to its association with reduced QoL caused by disease-related disability [2]. A total of 145 patients were given the final Persian version of the CRDS. Additionally, they were asked to complete the SF-36, which consists of 36 questions assessing the overall health of individuals. These 36 items have 8 subscales: Physical functioning, role-physical, bodily pain, general health (physical health composite), vitality, social functioning, role-emotional, and mental health (mental health composite). The Persian version of the SF-36 was translated and culturally adapted by Montazeri et al. [21]. It was assessed by measuring the Pearson correlation coefficient (r) between the CRDS total score and the scores of the physical health section of SF-36.
To evaluate the discriminant validity questionnaire, 130 healthy people also completed it. Then, an independent t-test was used to check the difference between constipated patients and healthy groups.
A committee of 8 gastroenterologists and internists evaluated the instrument’s content validity. Content validity ensures the instrument contains appropriate examples to demonstrate the desired structure. Each expert provided a score of 1 to 3 for each question (1=necessary, 2=useful but not necessary, 3=not necessary). The content validity ratio was then calculated. With 8 experts, a minimum acceptable item content validity ratio of approximately 0.75 was established [22]. Additionally, each question was evaluated by experts on a scale of 1 to 4, with 1 indicating no relevance, 2 indicating relevance but requiring significant revisions, 3 indicating some need for revision, and 4 indicating close relevance. Subsequently, the content validity index for each item was computed, whose value exceeding 0.78 signifies strong content validity [23]. The effect of a ceiling or flooring was also evaluated. If more than 15% of the participants attained the maximum or minimum score, it confirms a ceiling or flooring effect.
Results
Participants
This study involved the participation of 145 patients suffering from CFC; 86(59.3%) were women, and 59(40.7%) were men. The mean age of men and women was 49.05 years (30 to 73 years) and 46.88 years (range: 32 to 72 years), respectively.
Also, 130 healthy people completed the questionnaire; 82(63%) were women, and 43(37%) were men, and their Mean±SD age was 39.83±12.74.
Reliability
The reliability of the Persian version of CRDS was assessed by internal consistency and reproducibility measures.
We calculated the Cronbach α value to analyze the internal consistency and found the reliability of the CRDS questionnaire. The Cronbach α coefficients for all items of the CRDS, as well as the work/leisure activities subscale and the ADL subscale, were 0.86, 0.77, and 0.75, respectively. These results indicate a high level of internal consistency for the CRDS questionnaire.
We calculated the intra-class correlation coefficient to determine the reproducibility of the CRDS. This coefficient value for the total scale score of the CRDS was 0.98 (95% CI, 0.92%, 0.96%) (Table 2).
The coefficient values for the work/leisure activities subscale and the ADL subscale were 0.92 and 0.96, respectively.
Validity
An independent t-test was conducted to evaluate the discriminant validity of CRDS. The results revealed a significant difference between the healthy and patient groups in the scores obtained. Specifically, the constipated sample had a higher CRDS total score (Mean±SD 25.60±2.71) compared to the healthy controls (Mean±SD 4.02±3.6), t (273)=- 55.62, P<0.001. This finding suggests that CRDS can distinguish between the two groups effectively.
Furthermore, the total score and subscales of CRDS were found to be significantly correlated with the physical health composite score of SF-36 (R=-0.84 to -0.89, P<0.001) (Table 3).
This result indicates that individuals with higher levels of disability tend to have lower ratings of QoL.
Regarding content validity, the Lawshe content validity ratio for all items of the Persian CRDS was higher than 0.75, and the CVI for all items of the Persian CRDS was higher than 0.78. There was no ceiling/floor effect for the total score of the Persian CRDS and its subscales.
Discussion
The study results prove the reliability and validity of the Persian version of the CRDS to measure constipation’s impact on Iranian people’s daily activities. Although cross-cultural validity studies are challenging, they yield precious results. The provision of standard health tools enables the comparison of health status between countries. It provides reliable measurements to monitor health at the population level, estimate the disease burden, examine the consequences in clinical performance, and evaluate the therapeutic outcomes.
In this questionnaire, disability questions were simple and understandable. It makes it easy for people with a low literacy level, who comprise the most affected people, to complete the questionnaire. All patients completed all items of the Persian version of the CRDS, and no item was left unanswered. This high level of responsiveness indicates the patients’ good understanding of the questions, a sign of the acceptability of the Persian translation in this study.
A similar study [24] suggests that it is better to consider the type of chronic constipation and its cause in affected people because irritable bowel syndrome can also lead to chronic constipation. This syndrome results from the interaction between the brain and the intestine. The irritable bowel syndrome causes disability and affects people’s QoL differently. Thus, for the sake of homogeneity of the studied sample, patients with irritable bowel syndrome were excluded from the study, and only people with chronic functional constipation remained.
The Cronbach α and intra-class correlation coefficient values for the Persian version of CRDS and its subscales were lower than the English version, which can be due to the countries’ cultural differences and the translation and cultural adaptation processes. However, Cronbach α values in this study are also good and acceptable, which indicates good internal consistency of the Persian version of this questionnaire.
The intra-class correlation coefficient was measured by test re-test reliability over time. The coefficient value varies from 1 (the highest level of reliability) to 0 (the lowest level of reliability). Based on the findings of the statistical tests, the repeatability of the overall scores of the questionnaire and the subscales were 0.98, 0.92, and 0.96, respectively. According to the study of Hart et al. [2], the values are 0.88 and 0.87, respectively, and in both studies, the intra-class correlation coefficient values were greater than 0.85, indicating the good internal consistency of the questionnaire.
The correlation between the CRDS and SF-36 questionnaire scores was investigated to check the convergent validity. The Pearson correlation coefficient between the total score of the CRDS questionnaire and its subscales with the total score of the physical health composite of the SF-36 questionnaire was between -0.84 and -0.89 (high correlation). This coefficient has been obtained in a previous study [2] between -0.31 and -0.53 (moderate correlation). The reason for the lower correlation values in the English study is the separation of the subscales of the physical health composite of the SF-36 questionnaire. However, in this study, the total score from the physical health composite of the SF-36 questionnaire was considered, and its correlation with the total score of the CRDS questionnaire and its subscales was investigated. Negative correlation values indicate that higher levels of disability in people are associated with lower QoL.
This research’s limitations were related to the coronavirus disease and the need to gain the participants’ trust. It is suggested that in future studies, responsiveness could also be assessed and calculated, and the relationship between the CRDS questionnaire and the severity of constipation should be investigated.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the University of Social Welfare and Rehabilitation (Code:IR.USWR.REC.1400.338).
Funding
The research was not funded by any specific grants from public, commercial, or not-for-profit sectors.
Authors' contributions
All authors equally contributed to the preparation of all aspects of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank doctors and samples who helped in conducting this research.
References
- Wald A, Scarpignato C, Kamm MA, Mueller-Lissner S, Helfrich I, Schuijt C, et al. The burden of constipation on quality of life: Results of a multinational survey. Alimentary Pharmacology & Therapeutics. 2007; 26(2):227-36. [DOI:10.1111/j.1365-2036.2007.03376.x] [PMID]
- Hart SL, Albiani JJ, Crangle CJ, Torbit LA, Varma MG. Development and assessment of the constipation-related disability scale. Alimentary Pharmacology & Therapeutics. 2012; 35(1):183-92. [DOI:10.1111/j.1365-2036.2011.04910.x] [PMID]
- Peppas G, Alexiou VG, Mourtzoukou E, Falagas ME. Epidemiology of constipation in Europe and Oceania: A systematic review. BMC Gastroenterology. 2008; 8:5. [DOI:10.1186/1471-230X-8-5] [PMID] [PMCID]
- Schmulson MJ, Drossman DA. What is new in rome IV. Journal of Neurogastroenterology and Motility. 2017; 23(2):151-63. [DOI:10.5056/jnm16214] [PMID] [PMCID]
- Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: Systematic review and meta-analysis. The American Journal of Gastroenterology. 2011; 106(9):1582-91. [DOI:10.1038/ajg.2011.164] [PMID]
- Nojkov B, Baker J, Lee A, Eswaran SL, Menees SB, Saad RJ, et al. Impact of age and gender to severity of constipation-related symptoms and quality of life indices in patients with chronic idiopathic constipation. Gastroenterology. 2017; 152(5):S514-5. [DOI:10.1016/S0016-5085(17)31896-6]
- Jun DW, Park HY, Lee OY, Lee HL, Yoon BC, Choi HS, et al. A population-based study on bowel habits in a Korean community: Prevalence of functional constipation and self-reported constipation. Digestive Diseases and Sciences. 2006; 51(8):1471-7. [DOI:10.1007/s10620-006-9087-3] [PMID]
- Dennison C, Prasad M, Lloyd A, Bhattacharyya SK, Dhawan R, Coyne K. The health-related quality of life and economic burden of constipation. Pharmacoeconomics. 2005; 23(5):461-76. [DOI:10.2165/00019053-200523050-00006] [PMID]
- Belsey J, Greenfield S, Candy D, Geraint M. Systematic review: Impact of constipation on quality of life in adults and children. Alimentary Pharmacology & Therapeutics. 2010; 31(9):938-49. [DOI:10.1111/j.1365-2036.2010.04273.x] [PMID]
- Beunen G. Physical activity, fitness, and health: International proceedings and consensus statement. by Claude Bouchard, Roy J. Shephard, and Thomas Stephens. XXIV+ 1,055 pp. Champaign, IL: Human kinetics. 1994. $95.00 (cloth). American Journal of Human Biology. 1994; 6(5):675-6. [DOI:10.1002/ajhb.1310060517]
- van Engelenburg-van Lonkhuyzen ML, Bols EM, Benninga MA, Verwijs WA, Bluijssen NM, de Bie RA. The effect of pelvic physiotherapy on reduction of functional constipation in children: Design of a multicentre randomised controlled trial. BMC Pediatrics. 2013; 13:112. [DOI:10.1186/1471-2431-13-112] [PMID] [PMCID]
- Marquis P, De La Loge C, Dubois D, McDermott A, Chassany O. Development and validation of the patient assessment of constipation quality of life questionnaire. Scandinavian Journal of Gastroenterology. 2005; 40(5):540-51. [DOI:10.1080/00365520510012208] [PMID]
- Frank L, Kleinman L, Farup C, Taylor L, Miner P Jr. Psychometric validation of a constipation symptom assessment questionnaire. Scandinavian Journal of Gastroenterology. 1999; 34(9):870-7. [DOI:10.1080/003655299750025327] [PMID]
- Maher CG, Latimer J, Costa LOP. The relevance of cross-cultural adaptation and clinimetrics for physical therapy instruments. Revista Brasileira de Fisioterapia. 2007; 11(4):245-52. [DOI:10.1590/S1413-35552007000400002]
- Drossman DA, Dumitrascu DL. Rome III: New standard for functional gastrointestinal disorders. Drossman and Dumitrascu. 2006; 15(3):237. [Link]
- Agachan F, Chen T, Pfeifer J, Reissman P, Wexner SD. A constipation scoring system to simplify evaluation and management of constipated patients. Diseases of the Colon and Rectum. 1996; 39(6):681-5. [DOI:10.1007/BF02056950] [PMID]
- Bullinger M, Alonso J, Apolone G, Leplège A, Sullivan M, Wood-Dauphinee S, et al. Translating health status questionnaires and evaluating their quality: The IQOLA project approach. International Quality of Life Assessment. Journal of Clinical Epidemiology. 1998: 51(11):913-23. [DOI:10.1016/s0895-4356(98)00082-1] [PMID]
- Fermanian J. [Validation of assessment scales in physical medicine and rehabilitation: How are psychometric properties determined? (French)]. Annales de Readaptation et de Medecine Physique. 2005; 48(6):281-7. [DOI:10.1016/j.annrmp.2005.04.004] [PMID]
- Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. Journal of Clinical Epidemiology. 2007; 60(1):34-42. [DOI:10.1016/j.jclinepi.2006.03.012] [PMID]
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. Journal of Chiropractic Medicine. 2016; 15(2):155-63. [DOI:10.1016/j.jcm.2016.02.012] [PMID] [PMCID]
- Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The short form health survey (SF-36): Translation and validation study of the Iranian version. Quality of Life Research. 2005; 14(3):875-82. [DOI:10.1007/s11136-004-1014-5] [PMID]
- Lawshe CH. A quantitative approach to content validity. Personal Psychology. 1975; 28(4):563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
- Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Research in Nursing & Healthh. 2007; 30(4):459-67. [DOI:10.1002/nur.20199] [PMID]
- Nikjooy A, Jafari H, Saba MA, Ebrahimi N, Mirzaei R. Patient assessment of constipation quality of life questionnaire: Translation, cultural adaptation, reliability, and validity of the Persian version. Iranian Journal of Medical Sciences. 2018; 43(3):261-8. [PMID] [PMCID]
Type of Study: Research |
Subject:
Physiotherapy
Received: 2023/07/21 | Accepted: 2023/10/15 | Published: 2024/04/30
Received: 2023/07/21 | Accepted: 2023/10/15 | Published: 2024/04/30
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.