

Volume 6, Issue 1 (Continuously Updated 2023)
Func Disabil J 2023, 6(1): 0-0 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
R D, Lonimath A, Santhosh G. Screening of Early Developmental Delay and Its Risk Factors Among Children Seeking Health Care in India-exploring Missed Opportunities. Func Disabil J 2023; 6 (1) : 260.1
URL: http://fdj.iums.ac.ir/article-1-222-en.html
URL: http://fdj.iums.ac.ir/article-1-222-en.html



1- Department of Community Medicine, ESIC Medical College & PGIMSR, Rajiv Gandhi University of Health Sciences, Bengaluru, India.
2- Department of Community Medicine, ESIC Medical College & PGIMSR, Rajiv Gandhi University of Health Sciences, Bengaluru, India. ,drgokulsanthosh@gmail.com
2- Department of Community Medicine, ESIC Medical College & PGIMSR, Rajiv Gandhi University of Health Sciences, Bengaluru, India. ,
Keywords: Developmental delay, Developmental screening, Early identification, Community child health, Prevalence, Low middle-income country
Full-Text [PDF 813 kb]
(190 Downloads)
| Abstract (HTML) (595 Views)
Full-Text: (169 Views)
Introduction
child development is an ongoing composite process through which they acquire the competence to function adequately. Developmental process majorly occurs within the initial few years of life [1]. Developmental delay is when a child displays a significant delay in the achievement of milestones or skills, in one or more domains of development (i.e. gross motor, fine motor, speech/language, cognitive, personal/social, or activities of daily living) [2]. Early developmental delay is a condition that affects a child’s physical, cognitive, and emotional development. It can lead to a range of long-term adverse outcomes, including poor academic performance, social isolation, and mental health problems [2].
According to a 2019 report by the World Health Organization (WHO), the global prevalence of developmental disabilities among children under 5 years of age is estimated at 6-7% [3]. In 2016, approximately 52.9 million children were under the age of 5 worldwide who reported developmental disabilities [4]. In children who do not receive precise and timely intervention, it can lead to irreversible life-long mental, physical, social, auditory or visual disability. Globally, it is reported that a minimum of 3.3 million children under five years of age succumb to death from birth defects annually and another 3.2 million of those who survive may end up disabled for life. Over 90% of all newborns with a serious birth defect are born in low- and middle-income countries [4].
Global research on development collaborators reported that India ranked one in intellectual disability, hearing and vision loss, and autism spectrum disorders [4]. An estimated 10% of children experience developmental delays leading to disability in India [5]. The Indian literature is limited regarding early identification and intervention of developmental delays in youngsters, given multiple barriers to implementing screening. No structured or planned program exists to address this issue. This lack of a comprehensive program has resulted in many children with developmental delays not receiving the necessary support and care they require, which can have long-lasting effects on their lives.
Recognizing the critical need to address developmental delays in children, the Indian government introduced the Rashtriya Bal Swasthya Karyakram (RBSK) program in 2013 [5]. The program aims to provide early identification and intervention for children with developmental delays, disabilities, and other health issues up to the age of 18 years. One of the key components of the RBSK program is simple screening for developmental delay, which involves assessing a child’s developmental milestones, such as sitting, crawling, walking, and talking appropriate for age. This screening is conducted by trained RBSK officials who are doctors (mostly AYUSH), who visit schools, Anganwadi centers, and community-based settings.
In this context, it is crucial to understand the current scenario in India and explore potential solutions to ensure that children with developmental delays receive the necessary care and support. Quick screening tools can be easily integrated into the routine work-up of infants and young children in the healthcare system and the literature has shown to be efficient in early identification and intervention for children born with high risk of disability. This emphasizes opportunistic screening of developmental delays during routine healthcare visits for other health issues, such as immunization, malnutrition, or other illnesses.
In Bengaluru, limited information is found on the prevalence of developmental delays and the risk factors associated with them among children accessing healthcare services. This study will provide valuable insights into the benefits of opportunistic screening for developmental delay of children during immunization and outpatient department (OPD) visits and assess the prevalence and risk factors of early developmental delay in Bengaluru. It will aid in the development of appropriate screening and intervention strategies to support children’s early development. The findings of this study could also have broader implications for improving child health outcomes in other regions of India and providing appropriate interventions is crucial for promoting their overall well-being and long-term success.
Materials and Methods
A cross-sectional study was conducted among children under 2 years of age from first July 2022 to thirtieth September 2022. The study participants were attendees of routine immunization clinics at three rural (R1 and R2) primary health care (PHCs), two urban (U1 and U2) PHCs, and an urban teaching hospital (T1) OPD setting, in Bangalore. The RBSK screening questionnaire [6] was used as a study tool to screen for developmental delay. The tool has age-specific questions for screening the development delays under the categories of 2-4, 4-6, 6-9, 9-12, 12-15, and 15-24 months which assessed specific components, such as gross motor, fine motor, hearing, cognition, vision, speech, and social development. Children who are delayed in two or more components are called global developmental delay. Each attribute was identified, and proportion of the development delay was assessed. The tool also captured the child’s socio-demographic details, such as age, gender, place of health care seeking (data collection), and possible maternal risk factors, such as the history of consanguinous marriage, intake of folic acid during pregnancy, any illness during pregnancy, along with foetal risk factors, such as preterm/assisted delivery, birth asphyxia, low birth weight (LBW) responsible for the developmental delay of the child was assessed. The sample size of 160 people was calculated considering the prevalence of developmental delay of 16.2% as Sharma et al. [7] at a 95% confidence interval (CI) with 6% absolute allowable error and a 10% dropout rate. Equal representation from the rural, urban, and teaching hospitals counterparts was ensured by a simple random sampling technique. Children accessing healthcare services aged under 2 years in selected PHCS and hospitals in Bengaluru were included in the study. The participants whose caregivers did not consent to participate were excluded from the study. Data was collected through caregiver interviews and developmental assessment done using screening tools is described below. The outcome of interest was the prevalence of early developmental delay and the risk factors associated with it.
Procedure: Screening and assessing for development delay was a skillful process and the steps varied as per the child’s age mentioned above. Pre-requisites, such as the child should not be tired or hungry, the safety of the child, pleasant and comfortable settings at the OPD and immunization clinic, the accessible toys (age-appropriate literature or items) for young children as distracters were taken care of. Also observed for “readiness” clues and had taken adequate time to get “acquainted” with children. Used playful techniques for infants and young children and determined the best screening place (table, parent’s lap, examiner’s lap). Examined the least intrusive areas first (i.e. hands, arms); sensitive, painful, or intrusive test were administered last. A systematic approach was used but at the same time, we ensured flexibility to accommodate child’s behaviour and communication skills with children and their parents were also considered. A screening kit containing bangle, bell, crayons set, a small color book, torch, a small cube, and raisins were used during the time of data collection. The findings of the screening process were documented. After identifying the children with developmental delays, every first Thursday of the month, an integrated clinic with pediatrician, physical medicine and rehabilitation and public health expert was organized for follow-up and confirmation of those children. The confirmed cases were then registered under RBSK and appropriate treatment was given.
Analysis: Data were entered into Microsoft Office Excel sheet and analyzed using EPI INFO software, version 3.1. Descriptive data are presented as proportions and percentages and to summarize the prevalence of early developmental delay and the distribution of risk factors among the study population. A chi-square test was performed to deduce the association of developmental delay with various attributes. Bivariate logistic regression analysis was used to identify the risk factors associated with developmental delay and the odds ratio was calculated with and without adjustment for the confounding parameters.
Results
A total of 169 children was screened for developmental delay at OPD and immunization clinic in this study and the following results were generated after analyzing the data.
Socio-demographic details
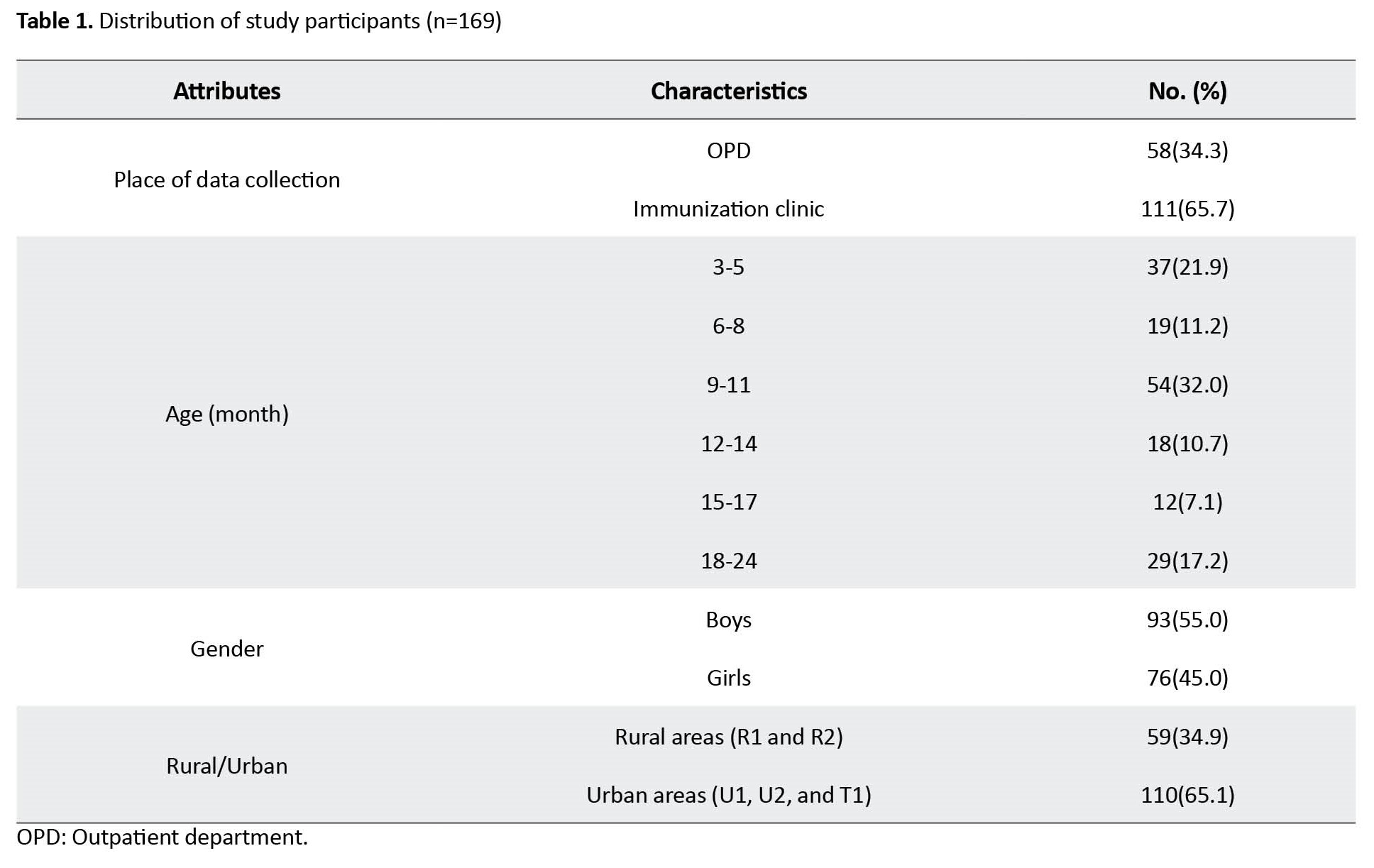
Table 1 presents that most study participants were from the immunization clinic (65.7%), in the age group of 9-11 months (32%), boys (55%) and from urban counterparts (65.1%).
Developmental delay
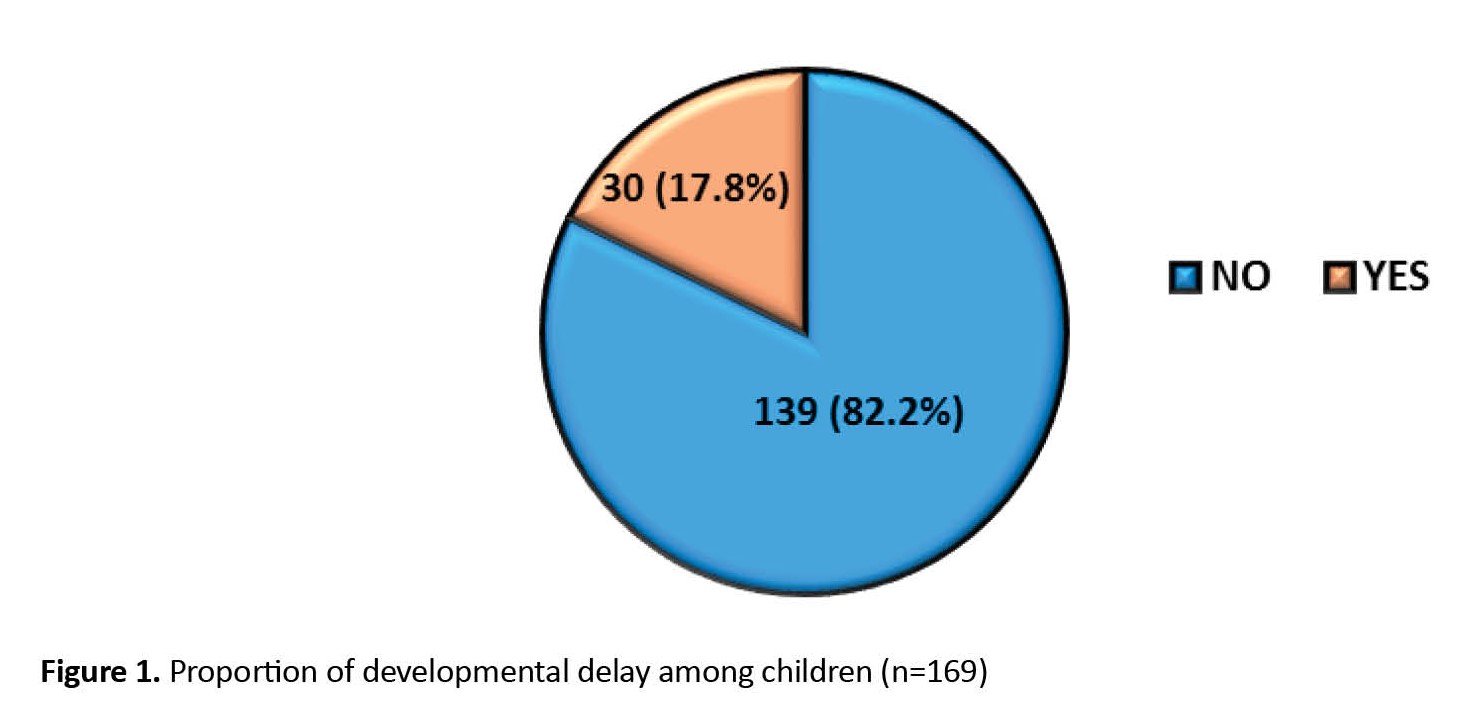
Figure 1 shows 17.8% had developmental delays when screened among all the study participants.
 Types of developmental delays
Types of developmental delays
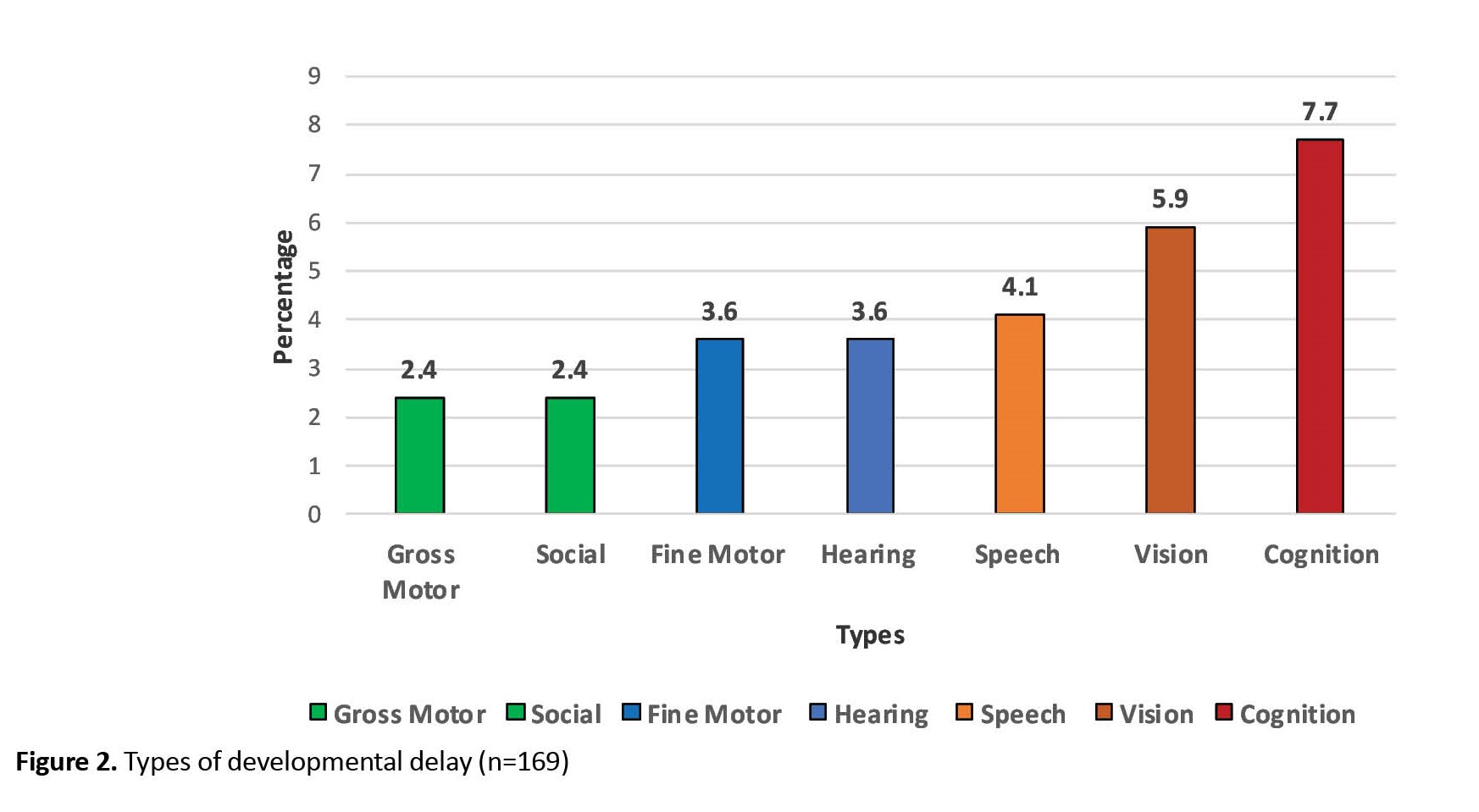
Figure 2 shows the distribution across types of developmental delay, the majority 7.7% of study participants had cognitive delay followed by delay in the development of cognition accounting for 5.9%. 9(5.3%) of the study participants had global developmental delay.
 Risk factors
Risk factors
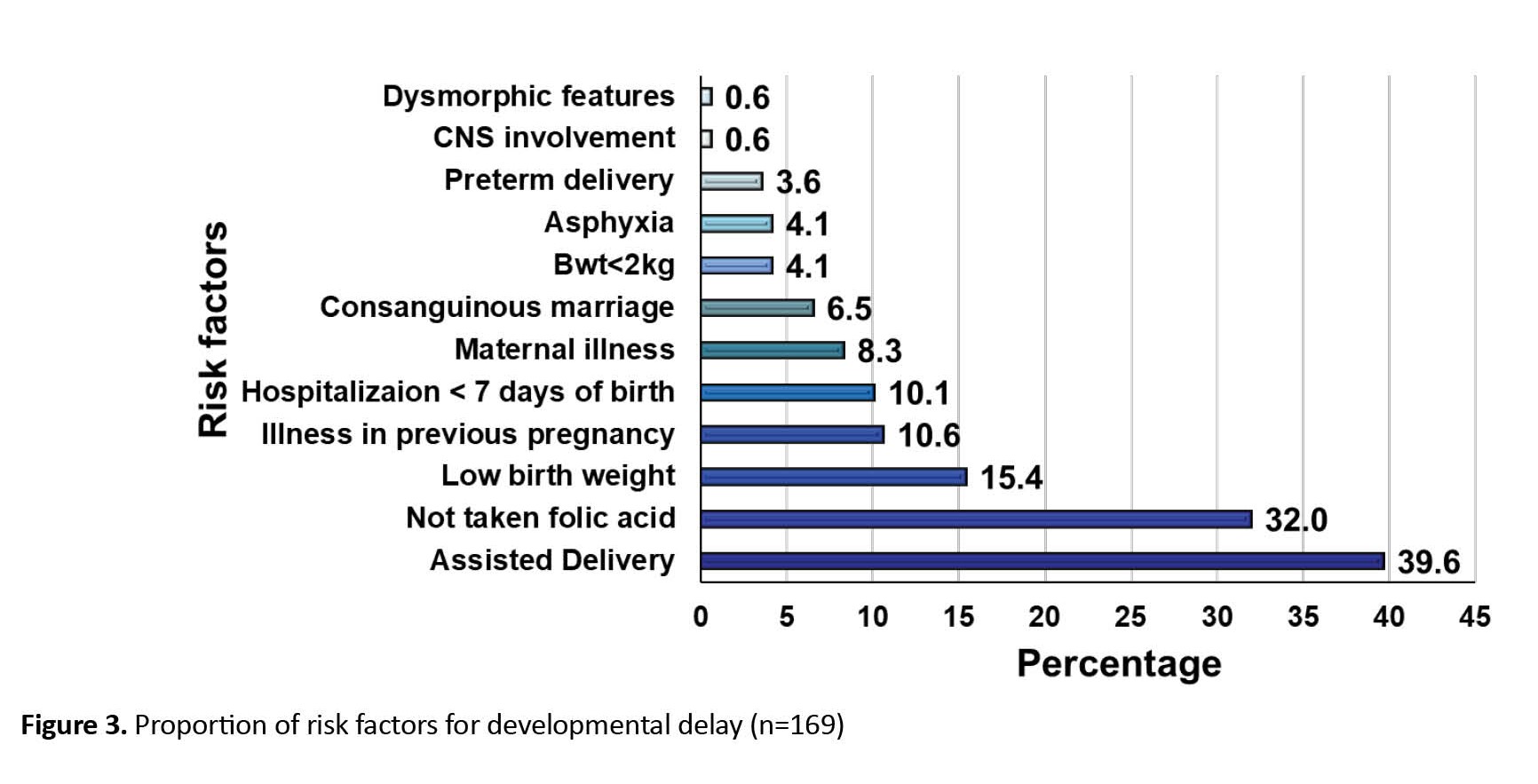
Figure 3 shows that assisted delivery (39.6%) was the major risk factor for the developmental delay followed by no folic acid intake (32%), low birth weight (15.4%), and illness in a previous pregnancy (10.6%).
Association of developmental delay
Table 2 presents the relationship of various attributes with developmental delay, a significant difference was observed between the age group and place of data collection with that of developmental with a P of 0.006 and 0.025, respectively.
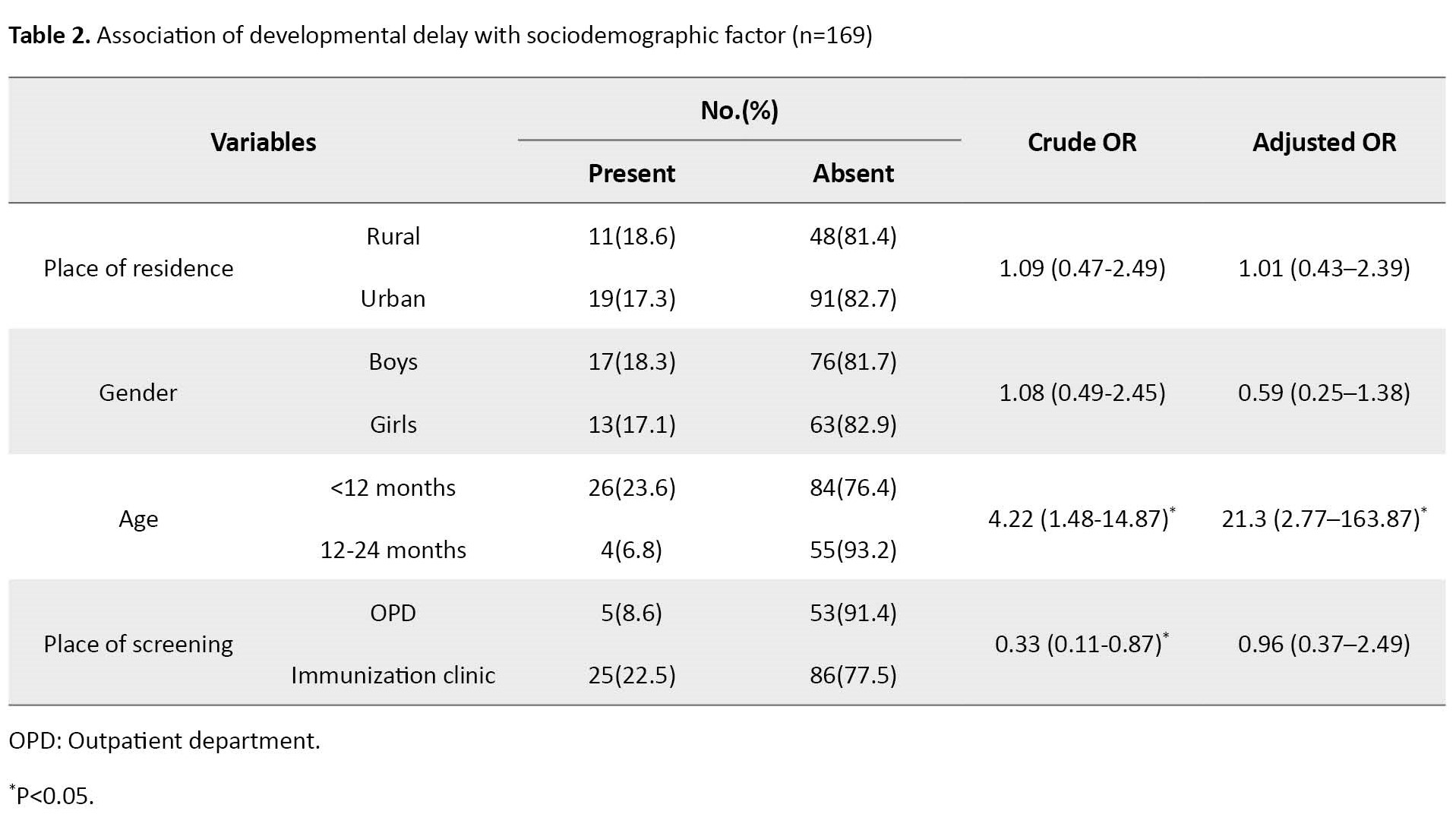
However, when adjustment was done for the risk factors, the child’s age was still associated with developmental delay. However, the location of the screening had no association.
Discussion
The present study was conducted among 169 children aged between 3- 24 months seeking healthcare services. Most study participants were from the Immunization Clinic (65.7%), in the age group of 9-11 months (32%), boys (55%), and from urban counterparts (65.1%). The present study reports a developmental delay prevalence of 17.8%. Cognitive delay was seen among 7.7% of the study participants followed by visual developmental delay in 5.9%. A total of 9 study participants (5.3%) had global developmental delays. Assisted delivery (39.6%) was identified as the major risk factor for developmental delay, followed by the lack of folic acid intake during the antenatal period (32%).
According to global research on developmental disabilities collaborators, the global burden of developmental disability among children under five years in 195 countries is estimated to be 8.4% [4]. A study conducted by Sharma et al. Uttar Pradesh showed that the recorded proportion of developmental delay was 16.2% [7]. A study conducted by Gupta et al showed similar findings prevalence of developmental delay at 6.6% (95% CI, 3.6%-9.8%) [8]. Similarly, a study conducted by Zablotsky et al. in the United States reported a comparable proportion of developmental delay among preschool children, ranging from 16.2% to 17.8%, which aligns with the findings of this study [9]. While the prevalence rates are somewhat similar to the current study, it is crucial to note the substantial disparities in geographical location and living conditions of the respective study areas. Furthermore, Nair et al.’s study in Kerala revealed that a developmental delay rate was 2.5% lower compared to the present study. Nair et al. study covered a larger geographic area and a higher number of participants and was conducted by community health workers (accredited social health activist [ASHA] workers). A total of 24.9% had language delay and 25% had multiple disabilities [10].
Global research on developmental disabilities collaborators showed that the proportion of developmental delay was higher in boys than females [4]. A study conducted by Gupta et al showed similar findings in developmental delay proportion which was more among male infants [8]. A study conducted by Zablotsky et al, also showed that boys were more likely to be diagnosed with any developmental disability than girls [9].
According to the study conducted by global research on developmental disabilities collaborators, vision loss was prevalent compared to hearing loss and intellectual disability [4]. In a review study conducted by Pascal et al., the prevalence of cognitive and motor delays was 16.9% and 20.6%, respectively [11]. These findings highlight significant variations in the prevalence rates of developmental delays, possibly attributable to geographical differences. Notably, this study stands out as one of the few studies conducted in India that specifically investigated the prevalence of various types of developmental delays, shedding light on the multifaceted nature of these conditions.
In the present study, pregnant women who did not receive folic acid (32%), assisted deliveries (39.6%) and the occurrence of low birth weight (15.4%), among newborns were identified as significant risk factors for developmental delay. A study conducted by Gupta et al showed that non-institutional deliveries contributed more towards the risk of developmental delay compared to institutional deliveries, which correlates with the findings of this study [8]. A study conducted by Vora H et al reported that pre-term children with small gestational age constituted a 33.3% risk factor for developmental delay [12]. A study conducted by Bhattacharya et al showed that children with birth weights less than 2500 grams and non-institutional deliveries had 8.3 times and 16 times higher odds of developing delay, respectively [13].
Conclusion
The prevalence of development delay and risk factors in the study population is high. Despite reporting the highest burden of development delays in India, no improvement in health outcomes, and no systematic interventions or policies to address their needs are observed. Moreover, more children diagnosed with developmental delays were identified during visits to immunization clinics compared to those attending outpatient clinics for specific illnesses. These findings emphasize the importance of implementing mandatory monitoring and opportunistic screening during immunization sessions to effectively identify developmental delays early in children.
Limitation
The study was conducted in and around a well-developed city in South India. So, the result cannot be generalized for the whole population of the country. To provide a better picture, an extensive study with a larger sample size is required. Since it is a screening tool, the final prevalence of the condition may vary, additionally, the study may be limited by the use of screening tools that may not capture all developmental delays, leading to an underestimation of the prevalence of the condition.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained by the Institutional of ESIC Medical College and Postgraduate Institute of Medical Science and Research (Code: 532/L/11/12/Ethics/ESICMC&PGIMSR/Estt.Vol.IV, dated 03.06.2022). Informed written consent was obtained from the caregivers of the study participants and all data was kept confidential and secure.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Deepthi R, Supervision, methodology, review & editing: Deepthi R and Ashwini Lonimath; Investigation: Ashwini Lonimath; Data collection, data curation and writing original draft: Gokul Santos.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to all the Urban and Rural Primary Health Centres who provided an opportunity to screen the children during immunization clinics and OPDs and provided us the platform to conduct the study.
References
child development is an ongoing composite process through which they acquire the competence to function adequately. Developmental process majorly occurs within the initial few years of life [1]. Developmental delay is when a child displays a significant delay in the achievement of milestones or skills, in one or more domains of development (i.e. gross motor, fine motor, speech/language, cognitive, personal/social, or activities of daily living) [2]. Early developmental delay is a condition that affects a child’s physical, cognitive, and emotional development. It can lead to a range of long-term adverse outcomes, including poor academic performance, social isolation, and mental health problems [2].
According to a 2019 report by the World Health Organization (WHO), the global prevalence of developmental disabilities among children under 5 years of age is estimated at 6-7% [3]. In 2016, approximately 52.9 million children were under the age of 5 worldwide who reported developmental disabilities [4]. In children who do not receive precise and timely intervention, it can lead to irreversible life-long mental, physical, social, auditory or visual disability. Globally, it is reported that a minimum of 3.3 million children under five years of age succumb to death from birth defects annually and another 3.2 million of those who survive may end up disabled for life. Over 90% of all newborns with a serious birth defect are born in low- and middle-income countries [4].
Global research on development collaborators reported that India ranked one in intellectual disability, hearing and vision loss, and autism spectrum disorders [4]. An estimated 10% of children experience developmental delays leading to disability in India [5]. The Indian literature is limited regarding early identification and intervention of developmental delays in youngsters, given multiple barriers to implementing screening. No structured or planned program exists to address this issue. This lack of a comprehensive program has resulted in many children with developmental delays not receiving the necessary support and care they require, which can have long-lasting effects on their lives.
Recognizing the critical need to address developmental delays in children, the Indian government introduced the Rashtriya Bal Swasthya Karyakram (RBSK) program in 2013 [5]. The program aims to provide early identification and intervention for children with developmental delays, disabilities, and other health issues up to the age of 18 years. One of the key components of the RBSK program is simple screening for developmental delay, which involves assessing a child’s developmental milestones, such as sitting, crawling, walking, and talking appropriate for age. This screening is conducted by trained RBSK officials who are doctors (mostly AYUSH), who visit schools, Anganwadi centers, and community-based settings.
In this context, it is crucial to understand the current scenario in India and explore potential solutions to ensure that children with developmental delays receive the necessary care and support. Quick screening tools can be easily integrated into the routine work-up of infants and young children in the healthcare system and the literature has shown to be efficient in early identification and intervention for children born with high risk of disability. This emphasizes opportunistic screening of developmental delays during routine healthcare visits for other health issues, such as immunization, malnutrition, or other illnesses.
In Bengaluru, limited information is found on the prevalence of developmental delays and the risk factors associated with them among children accessing healthcare services. This study will provide valuable insights into the benefits of opportunistic screening for developmental delay of children during immunization and outpatient department (OPD) visits and assess the prevalence and risk factors of early developmental delay in Bengaluru. It will aid in the development of appropriate screening and intervention strategies to support children’s early development. The findings of this study could also have broader implications for improving child health outcomes in other regions of India and providing appropriate interventions is crucial for promoting their overall well-being and long-term success.
Materials and Methods
A cross-sectional study was conducted among children under 2 years of age from first July 2022 to thirtieth September 2022. The study participants were attendees of routine immunization clinics at three rural (R1 and R2) primary health care (PHCs), two urban (U1 and U2) PHCs, and an urban teaching hospital (T1) OPD setting, in Bangalore. The RBSK screening questionnaire [6] was used as a study tool to screen for developmental delay. The tool has age-specific questions for screening the development delays under the categories of 2-4, 4-6, 6-9, 9-12, 12-15, and 15-24 months which assessed specific components, such as gross motor, fine motor, hearing, cognition, vision, speech, and social development. Children who are delayed in two or more components are called global developmental delay. Each attribute was identified, and proportion of the development delay was assessed. The tool also captured the child’s socio-demographic details, such as age, gender, place of health care seeking (data collection), and possible maternal risk factors, such as the history of consanguinous marriage, intake of folic acid during pregnancy, any illness during pregnancy, along with foetal risk factors, such as preterm/assisted delivery, birth asphyxia, low birth weight (LBW) responsible for the developmental delay of the child was assessed. The sample size of 160 people was calculated considering the prevalence of developmental delay of 16.2% as Sharma et al. [7] at a 95% confidence interval (CI) with 6% absolute allowable error and a 10% dropout rate. Equal representation from the rural, urban, and teaching hospitals counterparts was ensured by a simple random sampling technique. Children accessing healthcare services aged under 2 years in selected PHCS and hospitals in Bengaluru were included in the study. The participants whose caregivers did not consent to participate were excluded from the study. Data was collected through caregiver interviews and developmental assessment done using screening tools is described below. The outcome of interest was the prevalence of early developmental delay and the risk factors associated with it.
Procedure: Screening and assessing for development delay was a skillful process and the steps varied as per the child’s age mentioned above. Pre-requisites, such as the child should not be tired or hungry, the safety of the child, pleasant and comfortable settings at the OPD and immunization clinic, the accessible toys (age-appropriate literature or items) for young children as distracters were taken care of. Also observed for “readiness” clues and had taken adequate time to get “acquainted” with children. Used playful techniques for infants and young children and determined the best screening place (table, parent’s lap, examiner’s lap). Examined the least intrusive areas first (i.e. hands, arms); sensitive, painful, or intrusive test were administered last. A systematic approach was used but at the same time, we ensured flexibility to accommodate child’s behaviour and communication skills with children and their parents were also considered. A screening kit containing bangle, bell, crayons set, a small color book, torch, a small cube, and raisins were used during the time of data collection. The findings of the screening process were documented. After identifying the children with developmental delays, every first Thursday of the month, an integrated clinic with pediatrician, physical medicine and rehabilitation and public health expert was organized for follow-up and confirmation of those children. The confirmed cases were then registered under RBSK and appropriate treatment was given.
Analysis: Data were entered into Microsoft Office Excel sheet and analyzed using EPI INFO software, version 3.1. Descriptive data are presented as proportions and percentages and to summarize the prevalence of early developmental delay and the distribution of risk factors among the study population. A chi-square test was performed to deduce the association of developmental delay with various attributes. Bivariate logistic regression analysis was used to identify the risk factors associated with developmental delay and the odds ratio was calculated with and without adjustment for the confounding parameters.
Results
A total of 169 children was screened for developmental delay at OPD and immunization clinic in this study and the following results were generated after analyzing the data.
Socio-demographic details
Table 1 presents that most study participants were from the immunization clinic (65.7%), in the age group of 9-11 months (32%), boys (55%) and from urban counterparts (65.1%).
Developmental delay
Figure 1 shows 17.8% had developmental delays when screened among all the study participants.
Figure 2 shows the distribution across types of developmental delay, the majority 7.7% of study participants had cognitive delay followed by delay in the development of cognition accounting for 5.9%. 9(5.3%) of the study participants had global developmental delay.
Figure 3 shows that assisted delivery (39.6%) was the major risk factor for the developmental delay followed by no folic acid intake (32%), low birth weight (15.4%), and illness in a previous pregnancy (10.6%).
Association of developmental delay
Table 2 presents the relationship of various attributes with developmental delay, a significant difference was observed between the age group and place of data collection with that of developmental with a P of 0.006 and 0.025, respectively.
However, when adjustment was done for the risk factors, the child’s age was still associated with developmental delay. However, the location of the screening had no association.
Discussion
The present study was conducted among 169 children aged between 3- 24 months seeking healthcare services. Most study participants were from the Immunization Clinic (65.7%), in the age group of 9-11 months (32%), boys (55%), and from urban counterparts (65.1%). The present study reports a developmental delay prevalence of 17.8%. Cognitive delay was seen among 7.7% of the study participants followed by visual developmental delay in 5.9%. A total of 9 study participants (5.3%) had global developmental delays. Assisted delivery (39.6%) was identified as the major risk factor for developmental delay, followed by the lack of folic acid intake during the antenatal period (32%).
According to global research on developmental disabilities collaborators, the global burden of developmental disability among children under five years in 195 countries is estimated to be 8.4% [4]. A study conducted by Sharma et al. Uttar Pradesh showed that the recorded proportion of developmental delay was 16.2% [7]. A study conducted by Gupta et al showed similar findings prevalence of developmental delay at 6.6% (95% CI, 3.6%-9.8%) [8]. Similarly, a study conducted by Zablotsky et al. in the United States reported a comparable proportion of developmental delay among preschool children, ranging from 16.2% to 17.8%, which aligns with the findings of this study [9]. While the prevalence rates are somewhat similar to the current study, it is crucial to note the substantial disparities in geographical location and living conditions of the respective study areas. Furthermore, Nair et al.’s study in Kerala revealed that a developmental delay rate was 2.5% lower compared to the present study. Nair et al. study covered a larger geographic area and a higher number of participants and was conducted by community health workers (accredited social health activist [ASHA] workers). A total of 24.9% had language delay and 25% had multiple disabilities [10].
Global research on developmental disabilities collaborators showed that the proportion of developmental delay was higher in boys than females [4]. A study conducted by Gupta et al showed similar findings in developmental delay proportion which was more among male infants [8]. A study conducted by Zablotsky et al, also showed that boys were more likely to be diagnosed with any developmental disability than girls [9].
According to the study conducted by global research on developmental disabilities collaborators, vision loss was prevalent compared to hearing loss and intellectual disability [4]. In a review study conducted by Pascal et al., the prevalence of cognitive and motor delays was 16.9% and 20.6%, respectively [11]. These findings highlight significant variations in the prevalence rates of developmental delays, possibly attributable to geographical differences. Notably, this study stands out as one of the few studies conducted in India that specifically investigated the prevalence of various types of developmental delays, shedding light on the multifaceted nature of these conditions.
In the present study, pregnant women who did not receive folic acid (32%), assisted deliveries (39.6%) and the occurrence of low birth weight (15.4%), among newborns were identified as significant risk factors for developmental delay. A study conducted by Gupta et al showed that non-institutional deliveries contributed more towards the risk of developmental delay compared to institutional deliveries, which correlates with the findings of this study [8]. A study conducted by Vora H et al reported that pre-term children with small gestational age constituted a 33.3% risk factor for developmental delay [12]. A study conducted by Bhattacharya et al showed that children with birth weights less than 2500 grams and non-institutional deliveries had 8.3 times and 16 times higher odds of developing delay, respectively [13].
Conclusion
The prevalence of development delay and risk factors in the study population is high. Despite reporting the highest burden of development delays in India, no improvement in health outcomes, and no systematic interventions or policies to address their needs are observed. Moreover, more children diagnosed with developmental delays were identified during visits to immunization clinics compared to those attending outpatient clinics for specific illnesses. These findings emphasize the importance of implementing mandatory monitoring and opportunistic screening during immunization sessions to effectively identify developmental delays early in children.
Limitation
The study was conducted in and around a well-developed city in South India. So, the result cannot be generalized for the whole population of the country. To provide a better picture, an extensive study with a larger sample size is required. Since it is a screening tool, the final prevalence of the condition may vary, additionally, the study may be limited by the use of screening tools that may not capture all developmental delays, leading to an underestimation of the prevalence of the condition.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained by the Institutional of ESIC Medical College and Postgraduate Institute of Medical Science and Research (Code: 532/L/11/12/Ethics/ESICMC&PGIMSR/Estt.Vol.IV, dated 03.06.2022). Informed written consent was obtained from the caregivers of the study participants and all data was kept confidential and secure.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Deepthi R, Supervision, methodology, review & editing: Deepthi R and Ashwini Lonimath; Investigation: Ashwini Lonimath; Data collection, data curation and writing original draft: Gokul Santos.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful to all the Urban and Rural Primary Health Centres who provided an opportunity to screen the children during immunization clinics and OPDs and provided us the platform to conduct the study.
References
- Illingworth RS. The development of the infant and young child: normal and abnormal. Amsterdam: Elsevier Health Sciences; 2012. [Link]
- Poon JK, LaRosa AC, Pai GS. Developmental delay timely identification and assessment. Indian Pediatr. 2010; 47(5):415-22. [DOI:10.1007/s13312-010-0077-3] [PMID]
- World Health Organization. Disability. Geneva: World Health Organization; 2023. [Link]
- Global Research on Developmental Disabilities Collaborators. Developmental disabilities among children younger than 5 years in 195 countries and territories, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Glob Health. 2018; 6(10):e1100-21. [DOI:10.1016/S2214-109X(18)30309-7] [PMID]
- Ministry of Health & Family Welfare Government of India. Rashtriya Bal Swasthya Karyakram (RBSK): Child health screening and early intervention services under NRHM. New Delhi: Ministry of Health & Family Welfare Government of India; 2013. [Link]
- Ministry of Health & Family Welfare Government of India. Child health screening and early intervention services national rural health mission. Bharati Pawar: Ministry of Health & Family Welfare Government of India; 2014. [Link]
- Sharma N, Masood J, Singh SN, Ahmad N, Mishra P, Singh S, et al. Assessment of risk factors for developmental delays among children in a rural community of North India: A cross sectional study. J Educ Health Promot. 2019; 8:112. [PMID]
- Gupta S, Shrivastava P, Samsuzzaman M, Banerjee N, Das DK. Developmental delay among children under two years of age in slums of Burdwan Municipality: A cross-sectional study. J Family Med Prim Care. 2021; 10(5):1945-9. [DOI:10.4103/jfmpc.jfmpc_1926_20] [PMID] [PMCID]
- Zablotsky B, Black LI, Maenner MJ, Schieve LA, Danielson ML, Bitsko RH, et al. Prevalence and trends of developmental disabilities among children in the United States: 2009-2017. Pediatrics. 2019; 144(4):e20190811. [DOI:10.1542/peds.2019-0811] [PMID] [PMCID]
- Nair MK, Harikumaran Nair GS, Beena M, Princly P, Abhiram Chandran S, George B, et al. CDC Kerala 16: Early Detection of developmental delay/disability among children below 6 y--a district model. Indian J Pediatr. 2014; 81(Suppl 2):S151-5. [DOI:10.1007/s12098-014-1589-y] [PMID]
- Pascal A, Govaert P, Oostra A, Naulaers G, Ortibus E, Van den Broeck C. Neurodevelopmental outcome in very preterm and very-low-birthweight infants born over the past decade: A meta-analytic review. Dev Med Child Neurol. 2018; 60(4):342-355. [DOI:10.1111/dmcn.13675] [PMID]
- Vora H, Shah P, Mansuri SH. A study on developmental delay among children less than 2 year attending well baby clinic - Prevalence and antecedents factors. Int J Med Sci Public Health. 2013; 2(4):1084. [Link]
- Bhattacharya T, Ray S, Das DK. Developmental delay among children below two years of age: A cross-sectional study in a community development block of Burdwan district, West Bengal. Int J Community Med Public Health. 2017; 4(5):1762-7. [DOI:10.18203/2394-6040.ijcmph20171798]
Type of Study: Research |
Subject:
Professional education and practice
Received: 2023/06/16 | Accepted: 2023/07/24 | Published: 2023/02/6
Received: 2023/06/16 | Accepted: 2023/07/24 | Published: 2023/02/6
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.