

Volume 6, Issue 1 (Continuously Updated 2023)
Func Disabil J 2023, 6(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moallemi M, Rahbar N, Ahadi M, Maarefvand M. The Effects of a Home Personal Computer-based Auditory Training Program on the Binaural Listening Skills of Children With Specific Learning Disability: A Protocol for a Randomized Clinical Trial. Func Disabil J 2023; 6 (1) : 255.1
URL: http://fdj.iums.ac.ir/article-1-219-en.html
URL: http://fdj.iums.ac.ir/article-1-219-en.html



1- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,rahbar.n@iums.ac.ir
2- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 1093 kb]
(506 Downloads)
| Abstract (HTML) (1992 Views)
Full-Text: (765 Views)
Introduction
Materials and Methods
Design and registration
This study is a randomized clinical trial that examines the effectiveness of an auditory training program based on auditory brainstem function in children with a specific learning disability. Figure 1 shows the flowchart of the study.
 Figure 1. Flowchart of the study
Figure 1. Flowchart of the study
The Equation 1 is used to obtain an accurate sample size with a power of 80% and a type I error of 5% [22].
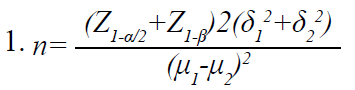
Based on the results (Mean±SD) of some auditory processing tests before and after intervention in a similar study [23], the sample size is determined as 9 in each group. Considering the possibility of withdrawal of several under-study children, we estimated the sample size to be 15 in each group.
Inclusion criteria
Data analysis
In descriptive statistics, tables and figures are used to present the data, central tendency, and dispersion indices. The Kolmogorov-Smirnov test is employed to assess the normal distribution of data. If the distribution of data is normal, for statistical analysis and comparing the results of before and after rehabilitation in each group, and comparing the results between the two groups, paired t-test, independent t-test, and analysis of covariance (ANCOVA) test are performed. In addition, suitable correlation tests and regression analysis are used to assess the potency of the relationship between the variables. Data is analyzed using the SPSS software, version 22.
Discussion
The first center in the ascending auditory pathway, in which binaural interaction and crossing of auditory pathways occur, is the brainstem. The advantages of binaural hearing largely depend on proper interaction between acoustic entrants of the two ears at the brainstem level [1-3]. Considering the functions of binaural hearing, it is clear that a deficit in binaural processing will interfere with the performance of the auditory system in noisy environments, and with accurate sound localization. The consequences of this defect seem to be more severe in school children who are in the early school years [1, 4, 5].
Children suffering from specific learning disabilities are one of the prominent groups with a high rate of complaints regarding sound localization and speech comprehension in noise. The reported prevalence of auditory processing disorder in children with learning disorders is around 30%-50% or higher [6]. A recent study conducted in Iran revealed that 74.2% of children with learning disabilities are at risk of auditory processing disorder [7]. Binaural processing difficulties are among the important difficulties of auditory processing in these individuals [2, 5, 8-10].
Rehabilitation of auditory processing disorder is essential due to the negative effect of the disorder on educational results [11]. Neural plasticity is the basis of the rehabilitation of central auditory processing disorders [12]. In the past, plasticity mechanisms were attributed to high-level sensory processing areas, such as the cortex. However, the results of recent studies on animal models as well as human studies using electrophysiological tools have provided considerable evidence on cellular and behavioral mechanisms of learning followed by repetitive experience or disease in the brainstem [13-17]. With a better understanding, it is recommended that auditory training programs should have a process-specific approach for individuals suffering from auditory processing disorders [5, 18]. Intervention in the central auditory processing disorder should arise from the nature of the hearing impairment that the individual suffers from, and how that defect is related to functional issues and behavioral consequences [19].
A review of scientific literature in the field of rehabilitation of central processing disorders in children with specific learning disabilities does not show a focused approach based on brainstem function to improve related abnormalities. In other words, no specific program has been provided that includes all the evaluations related to binaural interaction at the brainstem level that is home-centered at the same time. Opting for a computer-aided program at home is more cost-effective than frequent visits to a clinician, which would increase the patient’s expenses. In addition, exercising at any time of day at home can help build trust and motivate children to complete treatment.
Many studies containing auditory training programs for individuals with learning disorders have some limitations, such as lack of homogeneity of the study population in terms of the type of auditory processing impairment and especially, behavioral complaints related to them, and also lack of control groups for comparing the results, the absence of electrophysiological monitoring of the effects of the rehabilitation program, and lack of evaluation of the consistency of the effectiveness of auditory training program [20, 21].
Considering all the above-mentioned, the current study was conducted to develop a home-based auditory training program based on binaural interaction at the brainstem level and evaluate its effect on children with a specific learning disability and difficulty with speech perception in noise. This program is designed based on changes in different components of auditory-behavioral tests for binaural interaction.
Children suffering from specific learning disabilities are one of the prominent groups with a high rate of complaints regarding sound localization and speech comprehension in noise. The reported prevalence of auditory processing disorder in children with learning disorders is around 30%-50% or higher [6]. A recent study conducted in Iran revealed that 74.2% of children with learning disabilities are at risk of auditory processing disorder [7]. Binaural processing difficulties are among the important difficulties of auditory processing in these individuals [2, 5, 8-10].
Rehabilitation of auditory processing disorder is essential due to the negative effect of the disorder on educational results [11]. Neural plasticity is the basis of the rehabilitation of central auditory processing disorders [12]. In the past, plasticity mechanisms were attributed to high-level sensory processing areas, such as the cortex. However, the results of recent studies on animal models as well as human studies using electrophysiological tools have provided considerable evidence on cellular and behavioral mechanisms of learning followed by repetitive experience or disease in the brainstem [13-17]. With a better understanding, it is recommended that auditory training programs should have a process-specific approach for individuals suffering from auditory processing disorders [5, 18]. Intervention in the central auditory processing disorder should arise from the nature of the hearing impairment that the individual suffers from, and how that defect is related to functional issues and behavioral consequences [19].
A review of scientific literature in the field of rehabilitation of central processing disorders in children with specific learning disabilities does not show a focused approach based on brainstem function to improve related abnormalities. In other words, no specific program has been provided that includes all the evaluations related to binaural interaction at the brainstem level that is home-centered at the same time. Opting for a computer-aided program at home is more cost-effective than frequent visits to a clinician, which would increase the patient’s expenses. In addition, exercising at any time of day at home can help build trust and motivate children to complete treatment.
Many studies containing auditory training programs for individuals with learning disorders have some limitations, such as lack of homogeneity of the study population in terms of the type of auditory processing impairment and especially, behavioral complaints related to them, and also lack of control groups for comparing the results, the absence of electrophysiological monitoring of the effects of the rehabilitation program, and lack of evaluation of the consistency of the effectiveness of auditory training program [20, 21].
Considering all the above-mentioned, the current study was conducted to develop a home-based auditory training program based on binaural interaction at the brainstem level and evaluate its effect on children with a specific learning disability and difficulty with speech perception in noise. This program is designed based on changes in different components of auditory-behavioral tests for binaural interaction.
Materials and Methods
Design and registration
This study is a randomized clinical trial that examines the effectiveness of an auditory training program based on auditory brainstem function in children with a specific learning disability. Figure 1 shows the flowchart of the study.
Abbreviations: MLD: Masking level differences; PARWIN: Persian auditory recognition of words in noise; ABR: Auditory brainstem response; PRDDT: Persian randomized dichotic digits test, PPCW: Persian pediatric competing word; PPCST: Persian pediatric competing sentences test; APDQ: Auditory processing disorder questionnaire.
Study setting and participants
The target population is children with a specific learning disability in the age range of 7-12 years. The children are chosen with the convenience sampling method from centers related to the education of children with learning disorders in Isfahan City, Iran. After getting informed consent from their parents, these individuals are assessed for meeting inclusion criteria.Study setting and participants
The Equation 1 is used to obtain an accurate sample size with a power of 80% and a type I error of 5% [22].
Based on the results (Mean±SD) of some auditory processing tests before and after intervention in a similar study [23], the sample size is determined as 9 in each group. Considering the possibility of withdrawal of several under-study children, we estimated the sample size to be 15 in each group.
Inclusion criteria
The includin criteria were: Age 7-12 years, normal hearing threshold (≤20 dB HL) in frequencies between 250 Hz to 8 kHz, normal results in tympanometry and acoustic reflex tests, definitive diagnosis of specific learning disability by a psychologist based on DSM-5 criteria [24], right-handedness, a score of ≥90% in word recognition in silence, not undergoing music education and other rehabilitation programs, not having neurological and psychological disorders and not taking relevant medications, having a score result of <7 dB in the masking level differences (MLD) test [25], abnormality in the results of the Persian auditory recognition of words in noise (PARWIN) according to norms of Moradiju et al. study [26], and normal condition of auditory memory based on the digit span task [27].
Exclusion criteria
The child’s non-cooperation during the research, the parents’ lack of interest in continuing to cooperate with the research, and becoming infected with diseases that interfere with the study’s goal at the time of the research.
Procedures
Exclusion criteria
The child’s non-cooperation during the research, the parents’ lack of interest in continuing to cooperate with the research, and becoming infected with diseases that interfere with the study’s goal at the time of the research.
Procedures
Initial assessments, including binaural Speech-ABR, Persian randomized dichotic digits test (PRDDT), Persian pediatric competing word test (PPCWT), and Persian pediatric competing sentences test (PPCST) are conducted for all individuals who meet the inclusion criteria. Also, the Persian version of the auditory processing disorder questionnaire (APDQ-P) is completed by the student’s parents or teacher. We should remember that the MLD and PARWIN tests, while being part of the inclusion criteria, are also considered as an initial assessment.
Then students are randomly divided into intervention and control groups. Students who meet the inclusion criteria and take tests on even days are in the intervention group, and students who take tests on odd days are in the control group.
Intervention
1. Binaural fusion (BF) includes the ability to fuse two frequency ranges of one band-pass filtered speech unit (word) to comprehend and report the whole word [1].
Relevant exercise: The bandwidth of the filter, method of presenting words (diotic or dichotic), and type of word (monosyllabic or two-syllabic) are among the vital components for creating exercises in this section [1]. For example, if a certain word in the standard conditions of executing the test is passed through a low-pass filter with the range of 500-700 Hz and a high-pass filter with the range of 1900-2100 Hz, filters with a wider bandwidth are used in the first sessions in both high- and low-frequency ranges and the bandwidth of filters will become narrower gradually. The words are first presented to the ears diotically, which is easier to comprehend, and then they are presented dichotically in the harder stages. In the first sessions, we use two-syllabic words that have more redundancy and in the final sessions, we use monosyllabic words.
2- RASP includes the ability to combine time segments of verbal messages (sentences) presented alternately and sequentially between the two ears, and finally, comprehending one message [1].
Relevant exercise: In the RASP test, sentences comprising five to seven words are segmented into 300 ms parts that are alternately presented to both ears [1]. In creating exercises used in the rehabilitation program of the present study, these time segments lasted over 300 ms; therefore at the beginning of training, more information from each sentence is presented to each ear. For instance, the training starts with 500 ms segments. Logically, these time segments of sentence components get smaller over time, getting closer to 300 ms, and eventually reaching it. The other aspect considered in making exercises in this test is the use of sentences with easy-to-understand content or a richer linguistic texture at the beginning, and gradually making sentences harder in terms of content and texture of the language.
The words and sentences used in the BF and RASP exercises were chosen from story books and the Persian elementary school book, all of which had content and language suitable for children aged 7-12 years.
3- Masking level differences (MLD): The ability to detect target signals in noise is evaluated in the MLD test based on the phase difference of the signals presented to the ears [1].
Relevant exercise: In making exercises based on this test, we consider several parameters to create an easy-to-complicated process. The first parameter is the type of noise. Amplitude-modulated (AM) noise is used in the initial sessions, which results in more release of masking than narrow-band noise [25, 28]. The next parameter is noise intensity level, which can be increased up to 70 dB sound pressure level (SPL) and it creates more release of masking. The intensity level of 60 dB SPL is used for the noise in standard conditions of executing the MLD test [1, 29]. The third consideration is to get the threshold at SπN0 state alone in several stages and then obtain MLD. It seems that due to the difficulties of this task, performing numerous practice trials accompanied by encouragement or increasing the intensity and duration of the signal compared to noise in the initial steps, can be crucial to get familiarize with the sound of the tone before final exercises [1, 30].
4 and 5-sound lateralization tests based on interaural intensity difference (IID) and interaural time difference (ITD) cues include the ability to locate a sound source inside the head in various ITDs and IIDs.
Exercises relevant to tasks 4 and 5: White noise, passed through low-pass and high-pass filter with a cutoff frequency of 2000 Hz and intensity of 50 dB SL, is used as stimulus. These stimuli with different ITDs and IIDs are provided to the subject using headphones. Noise passed through low-pass filter is used in trials related to the use of ITD cues, and the noise passed through high-pass filter is used in trials related to the use of IID cues. In the final software, one image is visualized during this auditory task that is comprised of several sound sources placed at certain angles that correspond to the time and intensity cues. By hearing each cue, the subject points to the corresponding sound source (by clicking on it or marking the right spot) [29, 31]. For making trials in this test with an easy-to-complicated approach, in the first sessions, the child is asked to determine whether the sound is from the right or the left. In addition, larger ITD and IID values are used for each sound source in the initial sessions, and gradually decrease. In the beginning, the child searches for the right angle among fewer angles, while more angles are gradually simulated for them on the image from which they must choose.
The designed exercises were evaluated for content validity by eight academic experts in the fields of speech therapy and audiology. Those experts were among faculty members of Tehran University of Medical Sciences, Iran University of Medical Sciences, Shahid Beheshti University of Medical Sciences, University of Social Welfare and Rehabilitation Sciences, and Isfahan University of Medical Sciences. A three-point scale table was provided to the academic experts and they were asked to rate each item with three choices of suitable, quite suitable, and unsuitable for the following items, the ability to strengthen binaural interaction skills at the level of the brainstem, the adequacy of the number of exercises per session, appropriateness of the total number of rehabilitation sessions, the correspondence between the explanation of an exercise and its proper execution, the suitability of speech content in binaural fusion and RASP exercises and stimuli employed for MLD, ITD, and interaural level difference (ILD) related exercises, and their progression from easy to difficult. Eventually, the required score for the content validity ratio and the content validity index was obtained and most of the experts confirmed the designed exercises.
Time schedule of intervention
The rehabilitation period lasts 12 weeks and is scheduled three times a week and every other day. The program has three levels of difficulty (easy, moderate, and hard). One month (four weeks) is allocated to each level. Each session includes all five tasks and five exercises are created for each task, which are executed twice. The subject must score 80% or higher on each task by the end of the session to access the next set of exercises [32]. Otherwise, they should repeat the exercises from the previous session. Exercises are presented randomly to avoid memorization. Figure 2 shows the intervention’s flowchart.

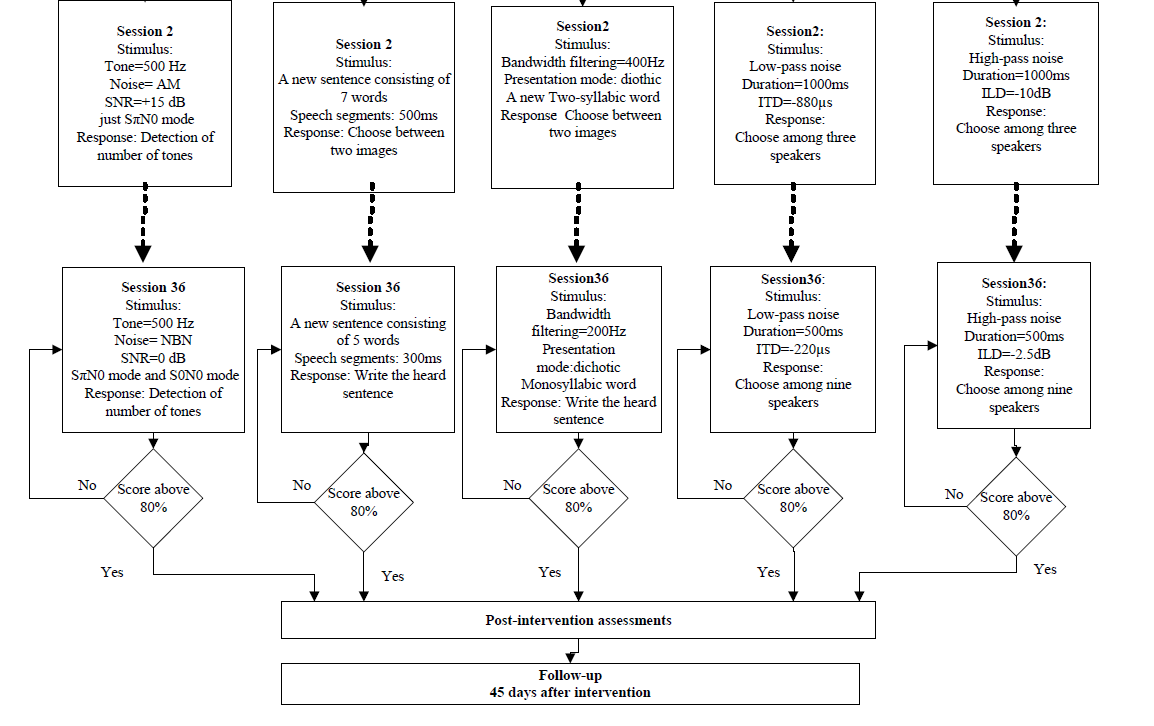
Figure 2. Flowchart of the intervention
The designed rehabilitation exercises were available on DVD, and the method of performing the exercises were explained to the child’s parents to be performed at home.
Following the completion of every stage, the score sheet should be sent to the therapist. The next stage can only be started when the previous stage is completed.
After completing all treatment sessions, both intervention and control groups are re-assessed again as post-intervention.
Considering that follow-up helps to more precisely assess the benefit of structured auditory training, the consistency of the probable effects of rehabilitation were re-evaluated after 45 days.
Primary outcome measures
MLD: A narrow-band in-phase noise at the intensity level of 60 dB SPL is provided to both ears, and the student listens to the noise for 4-5 s. Then, a 500 Hz tonal signal with the intensity of 60 dB SPL is delivered in phase to both ears (S0N0). If the child raises his hand, first the signal intensity reduces in 10 dB steps, and in case of not responding, the signal increases in 5 dB steps. When close to the threshold, these decreasing and increasing steps were 2 and 1 dB, respectively. This process is repeated at least three times near the threshold to obtain a reliable result. This method was then repeated for SπN0 conditions. SπN0 conditions mean a state in which the phase difference of the signals in the two ears is 180°, while the phase difference between the noises of the two ears is 0°. MLD is defined and calculated as the threshold difference between in-phase conditions (S0N0) and out-of-phase (SπN0) conditions [1, 4].
PARWIN: PARWIN is comprised of 35 monosyllabic words in the presence of the multi-talker babble noise, in which the ratio of signal to noise decreases from +24 dB to 0 dB in 5 dB steps, and in each signal-to-noise ratio (SNR), five monosyllabic words are provided binaurally. Test items are presented binaurally present at 55 dB SL (sensation level; ref: Speech reception threshold). This test measures the required SNR for 50% word recognition (SNR 50%) [33, 34].
The Spearman-Kärber equation (Equation 2) is used to calculate SNR 50%.
2. “SNR 50%=i+1/2(d)-(d)(#correct)/(w)”
Where i=+24 (the initial presentation level), d=4 (the decrement step size), w=5 (the number of words per decrement), and the term “correct” represents the number of words repeated accurately [35].
Speech-ABR: The 40 ms standard syllable /da/ is used as a stimulus to record Speech-ABR potential. /da/ stimulant includes an initial noise burst in the first 10 ms followed by a formant transition from consonant /d/ to vowel /a/ that is delivered by an insert phone and alternating polarity with the intensity of 80 dB SPL"
Responses are collected using 1024 digital sampling points in an 85.33 ms time window. Considering that response recording in the current study is binaural, thus electrode placement are in the form of two channels [36, 37]. Various Speech-ABR peaks (V-A-C-D-E-F-O) are identified in the last recorded traces. The analysis will include all peaks’ latency and amplitude, as well as VA slope (VA amplitude/VA duration) [38, 39].
Secondary outcome measures
We will also use some dichotic tests, including PRDDT, PPCST, and PPCWT to check the probable effect of the cortical areas on the study results or the possible effect of rehabilitation on the dichotic test results. Also, some behaviors related to auditory processing, attention, and language are evaluated using APDQ-P. These tests are done before and after rehabilitation.
PRDDT: PRDDT is among dichotic tests to evaluate central auditory processing. It is comprised of three groups of one, two, and three-pair digits. This test has several practice items and 54 trial items. The test is performed under free recall and at the intensity level of 70 dB HL [40]. In each list of this test, 108(100%) raw score is considered for each ear. Finally, the raw scores of the test are replaced by the correct percentage [33].
PPCWT: PPCWT is built according to screening test for auditory processing disorders in children (SCAN-C) competing words subtest and measures children’s dichotic hearing for monosyllabic words in a divided and directed attention manner. This test comprises four practice items and 30 trial items [34, 41]. The speech test materials are presented at 50 dB SL (sensation level; ref: Speech reception threshold) and the test is conducted under the conditions of pre-cued directed attention. PPCWT has a complete raw score of 30 for each ear and a total of 60, with one score assigned to each word. The final score is reported as the percentage of correct answer words [33, 34].
PPCST: PPCST is built according to SCAN-C competing sentences subtest, in which two short unrelated sentences are simultaneously provided to the child’s right and left ears. This test specifically measures binaural separation ability in dichotic listening. The test materials are presented to the ears of the children at 35 SL for the targeted ear and 50 dB SL for the non-targeted ear (sensation level; ref: Speech reception threshold). The test comprises 20 sentence pairs, with the initial 10 for the right ear scoring and the subsequent 10 for the left ear. The percentage of accurately answered sentences is reported for each ear [34, 42].
APDQ-P: APDQ-P was first designed by Brain O’Hara in 2006. The APDQ is the only questionnaire for APD screening that has been translated into Persian and has achieved validity and reliability [7, 43]. In addition to auditory processing skills, other skills, such as language and some aspects of attention in individuals aged 7-17 years are evaluated by this questionnaire. It has 52 items that are answered by the child’s parents or teacher [6, 7]. The questionnaire consists of 4 subscales, auditory processing (31 items), attention control (10 items), language (11 items), and targeted auditory processing (18 items). Each subset’s items can be scored 4 (always), 3 (often), 1 (sometimes), and 0 (rarely) [44]. The score of the questionnaire is calculated from the Equation 3 [7]:

Then students are randomly divided into intervention and control groups. Students who meet the inclusion criteria and take tests on even days are in the intervention group, and students who take tests on odd days are in the control group.
Intervention
1. Binaural fusion (BF) includes the ability to fuse two frequency ranges of one band-pass filtered speech unit (word) to comprehend and report the whole word [1].
Relevant exercise: The bandwidth of the filter, method of presenting words (diotic or dichotic), and type of word (monosyllabic or two-syllabic) are among the vital components for creating exercises in this section [1]. For example, if a certain word in the standard conditions of executing the test is passed through a low-pass filter with the range of 500-700 Hz and a high-pass filter with the range of 1900-2100 Hz, filters with a wider bandwidth are used in the first sessions in both high- and low-frequency ranges and the bandwidth of filters will become narrower gradually. The words are first presented to the ears diotically, which is easier to comprehend, and then they are presented dichotically in the harder stages. In the first sessions, we use two-syllabic words that have more redundancy and in the final sessions, we use monosyllabic words.
2- RASP includes the ability to combine time segments of verbal messages (sentences) presented alternately and sequentially between the two ears, and finally, comprehending one message [1].
Relevant exercise: In the RASP test, sentences comprising five to seven words are segmented into 300 ms parts that are alternately presented to both ears [1]. In creating exercises used in the rehabilitation program of the present study, these time segments lasted over 300 ms; therefore at the beginning of training, more information from each sentence is presented to each ear. For instance, the training starts with 500 ms segments. Logically, these time segments of sentence components get smaller over time, getting closer to 300 ms, and eventually reaching it. The other aspect considered in making exercises in this test is the use of sentences with easy-to-understand content or a richer linguistic texture at the beginning, and gradually making sentences harder in terms of content and texture of the language.
The words and sentences used in the BF and RASP exercises were chosen from story books and the Persian elementary school book, all of which had content and language suitable for children aged 7-12 years.
3- Masking level differences (MLD): The ability to detect target signals in noise is evaluated in the MLD test based on the phase difference of the signals presented to the ears [1].
Relevant exercise: In making exercises based on this test, we consider several parameters to create an easy-to-complicated process. The first parameter is the type of noise. Amplitude-modulated (AM) noise is used in the initial sessions, which results in more release of masking than narrow-band noise [25, 28]. The next parameter is noise intensity level, which can be increased up to 70 dB sound pressure level (SPL) and it creates more release of masking. The intensity level of 60 dB SPL is used for the noise in standard conditions of executing the MLD test [1, 29]. The third consideration is to get the threshold at SπN0 state alone in several stages and then obtain MLD. It seems that due to the difficulties of this task, performing numerous practice trials accompanied by encouragement or increasing the intensity and duration of the signal compared to noise in the initial steps, can be crucial to get familiarize with the sound of the tone before final exercises [1, 30].
4 and 5-sound lateralization tests based on interaural intensity difference (IID) and interaural time difference (ITD) cues include the ability to locate a sound source inside the head in various ITDs and IIDs.
Exercises relevant to tasks 4 and 5: White noise, passed through low-pass and high-pass filter with a cutoff frequency of 2000 Hz and intensity of 50 dB SL, is used as stimulus. These stimuli with different ITDs and IIDs are provided to the subject using headphones. Noise passed through low-pass filter is used in trials related to the use of ITD cues, and the noise passed through high-pass filter is used in trials related to the use of IID cues. In the final software, one image is visualized during this auditory task that is comprised of several sound sources placed at certain angles that correspond to the time and intensity cues. By hearing each cue, the subject points to the corresponding sound source (by clicking on it or marking the right spot) [29, 31]. For making trials in this test with an easy-to-complicated approach, in the first sessions, the child is asked to determine whether the sound is from the right or the left. In addition, larger ITD and IID values are used for each sound source in the initial sessions, and gradually decrease. In the beginning, the child searches for the right angle among fewer angles, while more angles are gradually simulated for them on the image from which they must choose.
The designed exercises were evaluated for content validity by eight academic experts in the fields of speech therapy and audiology. Those experts were among faculty members of Tehran University of Medical Sciences, Iran University of Medical Sciences, Shahid Beheshti University of Medical Sciences, University of Social Welfare and Rehabilitation Sciences, and Isfahan University of Medical Sciences. A three-point scale table was provided to the academic experts and they were asked to rate each item with three choices of suitable, quite suitable, and unsuitable for the following items, the ability to strengthen binaural interaction skills at the level of the brainstem, the adequacy of the number of exercises per session, appropriateness of the total number of rehabilitation sessions, the correspondence between the explanation of an exercise and its proper execution, the suitability of speech content in binaural fusion and RASP exercises and stimuli employed for MLD, ITD, and interaural level difference (ILD) related exercises, and their progression from easy to difficult. Eventually, the required score for the content validity ratio and the content validity index was obtained and most of the experts confirmed the designed exercises.
Time schedule of intervention
The rehabilitation period lasts 12 weeks and is scheduled three times a week and every other day. The program has three levels of difficulty (easy, moderate, and hard). One month (four weeks) is allocated to each level. Each session includes all five tasks and five exercises are created for each task, which are executed twice. The subject must score 80% or higher on each task by the end of the session to access the next set of exercises [32]. Otherwise, they should repeat the exercises from the previous session. Exercises are presented randomly to avoid memorization. Figure 2 shows the intervention’s flowchart.
Figure 2. Flowchart of the intervention
The designed rehabilitation exercises were available on DVD, and the method of performing the exercises were explained to the child’s parents to be performed at home.
Following the completion of every stage, the score sheet should be sent to the therapist. The next stage can only be started when the previous stage is completed.
After completing all treatment sessions, both intervention and control groups are re-assessed again as post-intervention.
Considering that follow-up helps to more precisely assess the benefit of structured auditory training, the consistency of the probable effects of rehabilitation were re-evaluated after 45 days.
Primary outcome measures
MLD: A narrow-band in-phase noise at the intensity level of 60 dB SPL is provided to both ears, and the student listens to the noise for 4-5 s. Then, a 500 Hz tonal signal with the intensity of 60 dB SPL is delivered in phase to both ears (S0N0). If the child raises his hand, first the signal intensity reduces in 10 dB steps, and in case of not responding, the signal increases in 5 dB steps. When close to the threshold, these decreasing and increasing steps were 2 and 1 dB, respectively. This process is repeated at least three times near the threshold to obtain a reliable result. This method was then repeated for SπN0 conditions. SπN0 conditions mean a state in which the phase difference of the signals in the two ears is 180°, while the phase difference between the noises of the two ears is 0°. MLD is defined and calculated as the threshold difference between in-phase conditions (S0N0) and out-of-phase (SπN0) conditions [1, 4].
PARWIN: PARWIN is comprised of 35 monosyllabic words in the presence of the multi-talker babble noise, in which the ratio of signal to noise decreases from +24 dB to 0 dB in 5 dB steps, and in each signal-to-noise ratio (SNR), five monosyllabic words are provided binaurally. Test items are presented binaurally present at 55 dB SL (sensation level; ref: Speech reception threshold). This test measures the required SNR for 50% word recognition (SNR 50%) [33, 34].
The Spearman-Kärber equation (Equation 2) is used to calculate SNR 50%.
2. “SNR 50%=i+1/2(d)-(d)(#correct)/(w)”
Where i=+24 (the initial presentation level), d=4 (the decrement step size), w=5 (the number of words per decrement), and the term “correct” represents the number of words repeated accurately [35].
Speech-ABR: The 40 ms standard syllable /da/ is used as a stimulus to record Speech-ABR potential. /da/ stimulant includes an initial noise burst in the first 10 ms followed by a formant transition from consonant /d/ to vowel /a/ that is delivered by an insert phone and alternating polarity with the intensity of 80 dB SPL"
Responses are collected using 1024 digital sampling points in an 85.33 ms time window. Considering that response recording in the current study is binaural, thus electrode placement are in the form of two channels [36, 37]. Various Speech-ABR peaks (V-A-C-D-E-F-O) are identified in the last recorded traces. The analysis will include all peaks’ latency and amplitude, as well as VA slope (VA amplitude/VA duration) [38, 39].
Secondary outcome measures
We will also use some dichotic tests, including PRDDT, PPCST, and PPCWT to check the probable effect of the cortical areas on the study results or the possible effect of rehabilitation on the dichotic test results. Also, some behaviors related to auditory processing, attention, and language are evaluated using APDQ-P. These tests are done before and after rehabilitation.
PRDDT: PRDDT is among dichotic tests to evaluate central auditory processing. It is comprised of three groups of one, two, and three-pair digits. This test has several practice items and 54 trial items. The test is performed under free recall and at the intensity level of 70 dB HL [40]. In each list of this test, 108(100%) raw score is considered for each ear. Finally, the raw scores of the test are replaced by the correct percentage [33].
PPCWT: PPCWT is built according to screening test for auditory processing disorders in children (SCAN-C) competing words subtest and measures children’s dichotic hearing for monosyllabic words in a divided and directed attention manner. This test comprises four practice items and 30 trial items [34, 41]. The speech test materials are presented at 50 dB SL (sensation level; ref: Speech reception threshold) and the test is conducted under the conditions of pre-cued directed attention. PPCWT has a complete raw score of 30 for each ear and a total of 60, with one score assigned to each word. The final score is reported as the percentage of correct answer words [33, 34].
PPCST: PPCST is built according to SCAN-C competing sentences subtest, in which two short unrelated sentences are simultaneously provided to the child’s right and left ears. This test specifically measures binaural separation ability in dichotic listening. The test materials are presented to the ears of the children at 35 SL for the targeted ear and 50 dB SL for the non-targeted ear (sensation level; ref: Speech reception threshold). The test comprises 20 sentence pairs, with the initial 10 for the right ear scoring and the subsequent 10 for the left ear. The percentage of accurately answered sentences is reported for each ear [34, 42].
APDQ-P: APDQ-P was first designed by Brain O’Hara in 2006. The APDQ is the only questionnaire for APD screening that has been translated into Persian and has achieved validity and reliability [7, 43]. In addition to auditory processing skills, other skills, such as language and some aspects of attention in individuals aged 7-17 years are evaluated by this questionnaire. It has 52 items that are answered by the child’s parents or teacher [6, 7]. The questionnaire consists of 4 subscales, auditory processing (31 items), attention control (10 items), language (11 items), and targeted auditory processing (18 items). Each subset’s items can be scored 4 (always), 3 (often), 1 (sometimes), and 0 (rarely) [44]. The score of the questionnaire is calculated from the Equation 3 [7]:
Data analysis
In descriptive statistics, tables and figures are used to present the data, central tendency, and dispersion indices. The Kolmogorov-Smirnov test is employed to assess the normal distribution of data. If the distribution of data is normal, for statistical analysis and comparing the results of before and after rehabilitation in each group, and comparing the results between the two groups, paired t-test, independent t-test, and analysis of covariance (ANCOVA) test are performed. In addition, suitable correlation tests and regression analysis are used to assess the potency of the relationship between the variables. Data is analyzed using the SPSS software, version 22.
Discussion
One of the critical populations with a high rate of complaints regarding speech comprehension in noise and sound localization is students suffering from special learning disabilities [2]. Since speech comprehension in noise and sound localization are the results of normal binaural processing, improving such aspects of auditory processing can facilitate learning for these children at school [10, 45]. Direct training of skills is one of the crucial approaches to the rehabilitation of central auditory processing disorders. In this approach, it is directly focused on strengthening some special skills involved in central auditory activities [45]. Relying on this approach, this study will try to design exercises based on the auditory brainstem function and to improve the auditory behaviors related to the brainstem. This specialization will probably result in a more efficient treatment program. Studies in the field of auditory training in individuals suffering from learning disabilities mainly consist of formal auditory training methods, such as Earobics and fast forward. These methods simultaneously address various skills of auditory and language processing, and do not focus on a specific aspect of listening skills [2, 3, 9, 10, 23, 46]. However, some studies have evaluated the efficacy of auditory training programs based on some auditory processing skills in children with a learning disorder. For example, in a study, Mahdavi et al specifically designed a temporal dichotic auditory training program and reported its effectiveness in improving speech recognition in children with learning disabilities. The consistency of auditory training results was not investigated in this study [33]. In another study, Mahdavi et al designed a dichotic interaural time difference training program and reported its positive effects on the components of dichotic tests [42]. Although a control group was not used and the consistency of training effects was not explored.
In this research, due to the use of speech materials, such as sentences and words in some exercises to evoke high-level cognitive demands (auditory working memory and attention), and also comprehend tone in the presence of noise in some other exercises, the brainstem that is part of an integrated network including afferent and efferent processes [47] will implicitly be considered. In the case of repeated encounters, not only higher levels are forced to use inputs from lower levels but also affect the way by which lower levels encode the input stimuli in a context-dependent manner [47]. According to the above, it is not yet understood to what extent plasticity in the subcortical area is directly affected by the cortex or the other way around, how it affects it. It seems that in the execution of various rehabilitation programs related to binaural processing in the entire pathway of the auditory system, studying the correlation between the results of hearing tests related to the brainstem and dichotic listening tests that evaluate the higher centers in the auditory system can help in clarifying this subject.
Conclusion
The auditory brainstem has shown considerable evidence of neuroplasticity following repeated experiences. Thus, focused auditory training of brainstem-based binaural auditory pathways is anticipated to enhance binaural hearing abilities. We will pursue this for children with learning disabilities, the largest classification among students receiving special education services, by designing an auditory training program tailored to their binaural auditory processing disorder. It is critical to consider the potential effects of the associated neural pathways when assessing the effectiveness of any rehabilitation program that focuses on a particular area.
Ethical Considerations
Compliance with ethical guidelines
Iran University of Medical Sciences approved the study (Code: IR.IUMS.REC.1399.300).
Funding
This paper was extracted from PhD thesis of Marziyeh Moallemi, approved by Department of Audiology, Iran University of Medical Sciences.
Authors' contributions
Conceptualization: Nariman Rahbar, Mohsen Ahadi and Marziyeh Moallemi; Supervision: Nariman Rahbar and Mohsen Ahadi; Methodology: Mohammad Maarefvand; Funding acqusition: Nariman Rahbar; Writing original draft: Marziyeh Moallemi; Review, editing and validation: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Conclusion
The auditory brainstem has shown considerable evidence of neuroplasticity following repeated experiences. Thus, focused auditory training of brainstem-based binaural auditory pathways is anticipated to enhance binaural hearing abilities. We will pursue this for children with learning disabilities, the largest classification among students receiving special education services, by designing an auditory training program tailored to their binaural auditory processing disorder. It is critical to consider the potential effects of the associated neural pathways when assessing the effectiveness of any rehabilitation program that focuses on a particular area.
Ethical Considerations
Compliance with ethical guidelines
Iran University of Medical Sciences approved the study (Code: IR.IUMS.REC.1399.300).
Funding
This paper was extracted from PhD thesis of Marziyeh Moallemi, approved by Department of Audiology, Iran University of Medical Sciences.
Authors' contributions
Conceptualization: Nariman Rahbar, Mohsen Ahadi and Marziyeh Moallemi; Supervision: Nariman Rahbar and Mohsen Ahadi; Methodology: Mohammad Maarefvand; Funding acqusition: Nariman Rahbar; Writing original draft: Marziyeh Moallemi; Review, editing and validation: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- In: Musiek FE, Chermak GD, editors. Handbook of central auditory processing disorder. Auditory neuroscience and diagnosis. San Diego: Plural Publishing; 2013. [Link]
- Banai K, Kraus N. Neurobiology of (central) auditory processing disorder and language-based learning disability. In: Musiek FE, Chermak GD, editors. Handbook of central auditory processing disorder. Auditory neuroscience and diagnosis. San Diego: Plural Publishing; 2007. [Link]
- Russo NM, Nicol TG, Zecker SG, Hayes EA, Kraus N. Auditory training improves neural timing in the human brainstem. Behav Brain Res. 2005; 156(1):95-103. [DOI:10.1016/j.bbr.2004.05.012] [PMID]
- Śpiewak P, Markowski J, Śpiewak B. Binaural masking levels difference in children with language-based learning disability correspond to speech in noise comprehensiveness. Otorynolaryngologia. 2012; 11(2). [Link]
- Iliadou V, Bamiou DE, Kaprinis S, Kandylis D, Kaprinis G. Auditory processing disorders in children suspected of learning disabilities-a need for screening?. Int J Pediatr Otorhinolaryngol. 2009; 73(7):1029-34. [DOI:10.1016/j.ijporl.2009.04.004] [PMID]
- Jarollahi F, Pourbakht A, Jalaie S, Oruie M. Screening of auditory processing disorders in school-aged children in Tehran, using the auditory processing domain questionnaire. Aud Vestib Res. 2022; 31(1):17-22. [DOI:10.18502/avr.v31i1.8130]
- Ahmadi Z, Jarollahi F, Ahadi M, Hosseini F, Khamisabadi S. Screening of auditory processing disorder in children with learning disabilities using the Persian version of the auditory processing domains questionnaire. Aud Vest Res. 2020; 29(3):156-64. [DOI:10.18502/avr.v29i3.3848]
- Koiek S, Pourbakht A, Mahdavi ME, Tahaei AA. Acceptable noise level in learning disordered children. Aud Vestib Res. 2018; 27(2):86-92. [Link]
- Pinheiro FH, Capellini SA. [Auditory training in students with learning disabilities (Portuguese)]. Pro Fono. 2010; 22(1):49-54. [DOI:10.1590/S0104-56872010000100010] [PMID]
- King C, Warrier CM, Hayes E, Kraus N. Deficits in auditory brainstem pathway encoding of speech sounds in children with learning problems. Neurosci Lett. 2002; 319(2):111-5. [DOI:10.1016/S0304-3940(01)02556-3] [PMID]
- Dawes P, Bishop D. Auditory processing disorder in relation to developmental disorders of language, communication and attention: a review and critique. Int J Lang Commun Disord. 2009; 44(4):440-65. [DOI:10.1080/13682820902929073] [PMID]
- Ferre JM. Treating central auditory processing disorders (CAPDs) among children and adults. Can Audiol. 2016; 3(4):1-7. [Link]
- Zheng Y, Baek JH, Smith PF, Darlington CL. Cannabinoid receptor down-regulation in the ventral cochlear nucleus in a salicylate model of tinnitus. Hear Res. 2007; 228(1-2):105-11. [DOI:10.1016/j.heares.2007.01.028] [PMID]
- Krishnan A, Xu Y, Gandour J, Cariani P. Encoding of pitch in the human brainstem is sensitive to language experience. Brain Res Cogn Brain Res. 2005; 25(1):161-8. [DOI:10.1016/j.cogbrainres.2005.05.004] [PMID]
- Musacchia G, Sams M, Skoe E, Kraus N. Musicians have enhanced subcortical auditory and audiovisual processing of speech and music. Proc Natl Acad Sci USA. 2007; 104(40):15894-8. [DOI:10.1073/pnas.0701498104] [PMID]
- Magnusson AK, Park TJ, Pecka M, Grothe B, Koch U. Retrograde GABA signaling adjusts sound localization by balancing excitation and inhibition in the brainstem. Neuron. 2008; 59(1):125-37. [DOI:10.1016/j.neuron.2008.05.011] [PMID]
- Song JH, Skoe E, Banai K, Kraus N. Training to improve hearing speech in noise: Biological mechanisms. Cereb Cortex. 2012; 22(5):1180-90. [DOI:10.1093/cercor/bhr196] [PMID]
- Weihing J, Chermak GD, Musiek FE. Auditory training for central auditory processing disorder. Semin Hear. 2015; 36(4):199-215. [DOI:10.1055/s-0035-1564458] [PMID]
- Cameron S, Dillon H. Spatial hearing deficits as a major cause of auditory processing disorders: Diagnosis with the LISN-S and management options. Paper presened at: Proceedings of A Sound Foundation Through Early Amplication International Conference. 6-8 December 2007; Chicago: Phonak. [Link]
- Loo JH, Bamiou DE, Campbell N, Luxon LM. Computer-based auditory training (CBAT): Benefits for children with language- and reading-related learning difficulties. Dev Med Child Neurol. 2010; 52(8):708-17 [DOI:10.1111/j.1469-8749.2010.03654.x] [PMID]
- Simões HD, Zanchetta S, Furtado EF. Auditory training methods in children with psychiatric diagnosis: An integrative literature review. Revista CEFAC. 2019; 22. [DOI:10.1590/1982-0216/202022218318]
- Jarollahi F, Amiri M, Jalaie S, Sameni SJ. The effects of auditory spatial training on informational masking release in elderly listeners: A study protocol for a randomized clinical trial. F1000Res. 2019; 8:420. [DOI:10.12688/f1000research.18602.2] [PMID]
- Hayes EA, Warrier CM, Nicol TG, Zecker SG, Kraus N. Neural plasticity following auditory training in children with learning problems. Clin Neurophysiol. 2003; 114(4):673-84. [DOI:10.1016/S1388-2457(02)00414-5] [PMID]
- Tannock R. DSM-5 changes in diagnostic criteria for specific learning disabilities (SLD): What are the implications. Pikesville: International Dyslexia Association; 2014. [Link]
- da Silva de Paula P , Frota SMMC, Felipe L. Masking level difference (MLD): Literature review. Glob J Oto. 2017; 5(1):555655. [DOI:10.19080/GJO.2017.05.555655]
- Moradiju E, Mahdavi ME, Zarrinkoob H, Tabatabaee SM. [Relative and absolute test re-test reliability of several Persian auditory processing tests for dichotic listening and recognition of speech-in-noise in normal children aged 6-12 years (Persian)]. Sci J Rehabil Med. 2017; 6(4):160-7. [DOI:10.22037/JRM.2017.110584.1389]
- Moossavi A, Etemadi M, Javanbakht M, Bakhshi E, Sharafi MA. Relationship between working memory capacity and speech perception in noise among children with cochlear implant. Aud Vest Res. 2016; 25(4):227-33. [Link]
- Burnham MN. Normal masking level difference parameters for use in the clinical evaluation of auditory processing disorders [MSc thesis]. Provo: Brigham Young University; 2010. [Link]
- Zakaria M N. Auditory localization in subjects with central auditory processing disorders [MSc. thesis]. Perth: University of Western Australia; 2007. [Link]
- Wilson RH, Fowler CG. Effects of signal duration on the 500-Hz masking-level difference. Scand Audiol. 1986; 15(4):209-15. [DOI:10.3109/14992028609042145] [PMID]
- Lotfi Y, Dastgerdi ZH, Moossavi A, Mehrkian S, Bakhshi E. [Evaluation of auditory lateralization ability and its development in normal children with 8 to 11 years of age (Persian)]. Aud Vestib Res. 2017; 23(4):60-8. [Link]
- Sattari K, Rahbar N, Ahadi M, Haghani H. Developing a temporal processing-based auditory training program for the senior users of hearing aids: A home PC-based program. Aud Vestib Res. 2021; 30(1):42-49. [DOI:10.18502/avr.v30i1.5310]
- Mahdavi ME. [Development of a dichotic training program with multi-talker babble and its effect on recognition of speech-in-noise in learning-disabled children (Persian)] [PhD thesis]. Tehran: Iran University of Medical Sciences; 2016. [Link]
- Mahdavi ME, Pourbakht A, Parand A, Jalaie S, Rezaeian M, Moradiju E. Auditory recognition of words and digits in multitalker babble in learning-disabled children with dichotic listening deficit. Iran Red Crescent Med J. 2017; 19(4):e42817. [DOI:10.5812/ircmj.42817]
- Lotfi Y, Salim S, Mehrkian S, Ahmadi T, Biglarian A. The Persian version of words-in-noise test for young population: Development and validation. Aud Vestib Res. 2016; 25(4):194-200. [Link]
- Ahadi M. [Detection and analysis of binaural interaction component (BIC) in speech evoked auditory brainstem responses (Persian)] [PhD thesis] Tehran: Iran University of Medical Sciences. 2014. [Link]
- Jalaei B, Azmi MH, Zakaria MN. Gender differences in binaural speech-evoked auditory brainstem response: Are they clinically significant?. Braz J Otorhinolaryngol. 2019; 85:486-93. [DOI:10.1016/j.bjorl.2018.04.005] [PMID]
- Moossavi A, Lotfi Y, Javanbakht M, Faghihzadeh S. Speech-evoked auditory brainstem response; electrophysiological evidence of upper brainstem facilitative role on sound lateralization in noise. Neurol Sci. 2020; 41(3):611-617. [DOI:10.1007/s10072-019-04102-z] [PMID]
- Sanfins MD, Borges LR, Ubiali T, Colella-Santos MF. Speech auditory brainstem response (speech ABR) in the differential diagnosis of scholastic difficulties. Braz J Otorhinolaryngol. 2017; 83(1):112-6. [DOI:10.1016/j.bjorl.2015.05.014] [PMID]
- Mahdavi ME, Pourbakht A, Parand A, Jalaie S. Test-retest reliability and minimal detectable change of randomized dichotic digits in learning-disabled children: Implications for dichotic listening training. J Am Acad Audiol. 2018; 29(03):223-32. [DOI:10.3766/jaaa.16134] [PMID]
- Mahdavi ME, Peyvandi AA. [Persian competing word test: Development and preliminary results in normal children (Persian)]. Audiology. 2007;16(2):1-7. [Link]
- Mahdavi ME, Rezaeian M, Zarrinkoob H, Rezaeian M, Akbarzadeh A. Effect of a dichotic interaural time difference program on dichotic listening deficit of children with learning difficulty. J Am Acad Audiol. 2021; 32(05):295-302. [DOI:10.1055/s-0041-1728753] [PMID]
- Ahmadi Z, Jarollahi F, Ahadi M, Hosseini AF. Normalization and validation of auditory processing domain questionnaire in normal 8-12 year-old children. Aud Vestib Res. 2017; 26(2):93-8. [Link]
- O’Hara B, Mealings K. Developing the auditory processing domains questionnaire (APDQ): A differential screening tool for auditory processing disorder. Int J Audiol. 2018; 57(10):764-75. [DOI:10.1080/14992027.2018.1487087] [PMID]
- Ghasemi M, Hassanzadeh S, Shokoohi YM, Afrooz G, Tahaei AA, Farzad V. The effectiveness of central auditory processing rehabilitation program on speech reception in noise and dichotic listening in dyslexic students. Aud Vest Res. 2016; 25(3):183-93. [Link]
- Kraus N. Auditory pathway encoding and neural plasticity in children with learning problems. Audiol Neurootol. 2001; 6(4):221-7. [DOI:10.1159/000046837] [PMID]
- Malayeri S, Lotfi Y, Moossavi SA, Rostami R, Faghihzadeh S. Brainstem response to speech and non-speech stimuli in children with learning problems. Hear Res. 2014; 313:75-82. [DOI:10.1016/j.heares.2014.04.009] [PMID]
Type of Study: Research |
Subject:
Audiology
Received: 2023/05/18 | Accepted: 2023/08/9 | Published: 2023/02/6
Received: 2023/05/18 | Accepted: 2023/08/9 | Published: 2023/02/6
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.