

Volume 6, Issue 1 (Continuously Updated 2023)
Func Disabil J 2023, 6(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fallahian M, Shirazi S A, Vasaghi-Gharamaleki B. Absence of Hearing Loss in Young People With the Forward Head Posture. Func Disabil J 2023; 6 (1) : 231.2
URL: http://fdj.iums.ac.ir/article-1-216-en.html
URL: http://fdj.iums.ac.ir/article-1-216-en.html



1- Rehabilitation Research Center, Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Sciences (IUMS), Tehran, Iran.
2- School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
3- Rehabilitation Research Center, Department of Basic Sciences in Rehabilitation, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,vasaghi.b@iums.ac.ir
2- School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
3- Rehabilitation Research Center, Department of Basic Sciences in Rehabilitation, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 1385 kb]
(582 Downloads)
| Abstract (HTML) (1959 Views)
Full-Text: (702 Views)
Introduction
Today’s industrialized life and non-ergonomic design of various devices in use result in a major problem, namely, the development of injuries and abnormalities in the vertebral column due to the incorrect use of muscles. One such abnormality is the forward head posture (FHP). FHP is defined as the forward displacement of lower cervical vertebrae and over-extension of upper cervical vertebrae that increase the effect of gravitational forces on the head [1]. Continued use of computer and television, playing video games, and even wearing backpacks, place the head in the anterior position and displace one’s line of sight downwards. To correct the line of sight, the person adjusts their body by assuming a head-forward position, which leads to FHP [1, 2].
FHP is one of the most prevalent positional abnormalities of the vertebral column, with a prevalence of 66%, and is classified as a chronic pain syndrome [3]. The side effects of FHP include cervical nervous system problems, temporomandibular joint misalignment and disorders in chewing, increased pressure on blood vessels and reduced vertebral blood flow to the brain, and brain stem [4, 5, 6]. The ear receives its blood supply from several arteries; parts of the inner ear are supplied by a branch of the labyrinthine artery which originates from the anterior inferior and posterior inferior cerebellar arteries. These two arteries are among the branches of the basilar artery, and the basilar artery is formed by joining the two vertebral arteries. Vertebrobasilar artery ischemia, especially obstruction of the anterior inferior cerebellar artery or one of its branches, can result in bilateral hearing loss regardless of age [7, 8, 9].
If the forward head can damage the neck structures, can it also cause hearing loss? To answer this question, this study was designed to examine the effects of the presence of FHP on hearing thresholds in students. It also investigated the effect of FHP severity on hearing thresholds.
Materials and Methods
In this cross-sectional study, 55 students (31 women aged 20-25 years, and 24 men aged 20-31 years) participated voluntarily. The study protocol was supported by the Iran University of Medical Sciences (IUMS) (90-01-125-13152). The study was conducted in the audiology clinic of Iran University of Medical Sciences. All participants provided written informed consent and then completed a questionnaire, including general questions (sex, year of birth, height, weight and…) and specialized questions on hearing risk factors. The exclusion criteria included the presence of compacted or semi-compacted earwax, a history of trauma to the ear, ear pain, a sense of fullness and pressure in the ear, tinnitus, vertigo, a history of taking any ototoxic medications, and a history of prolonged use of hands-free devices at high volume. The only inclusion criterion was verbal and written consent for participation.
To measure FHP, the participants sat on a chair (which was the same for all the participants) and were asked to look forward. Then, the indicator was placed on the spinous process of the seventh cervical vertebra, and six profile photos were taken from a 1.5 m distance by a digital camera (Figure 1).
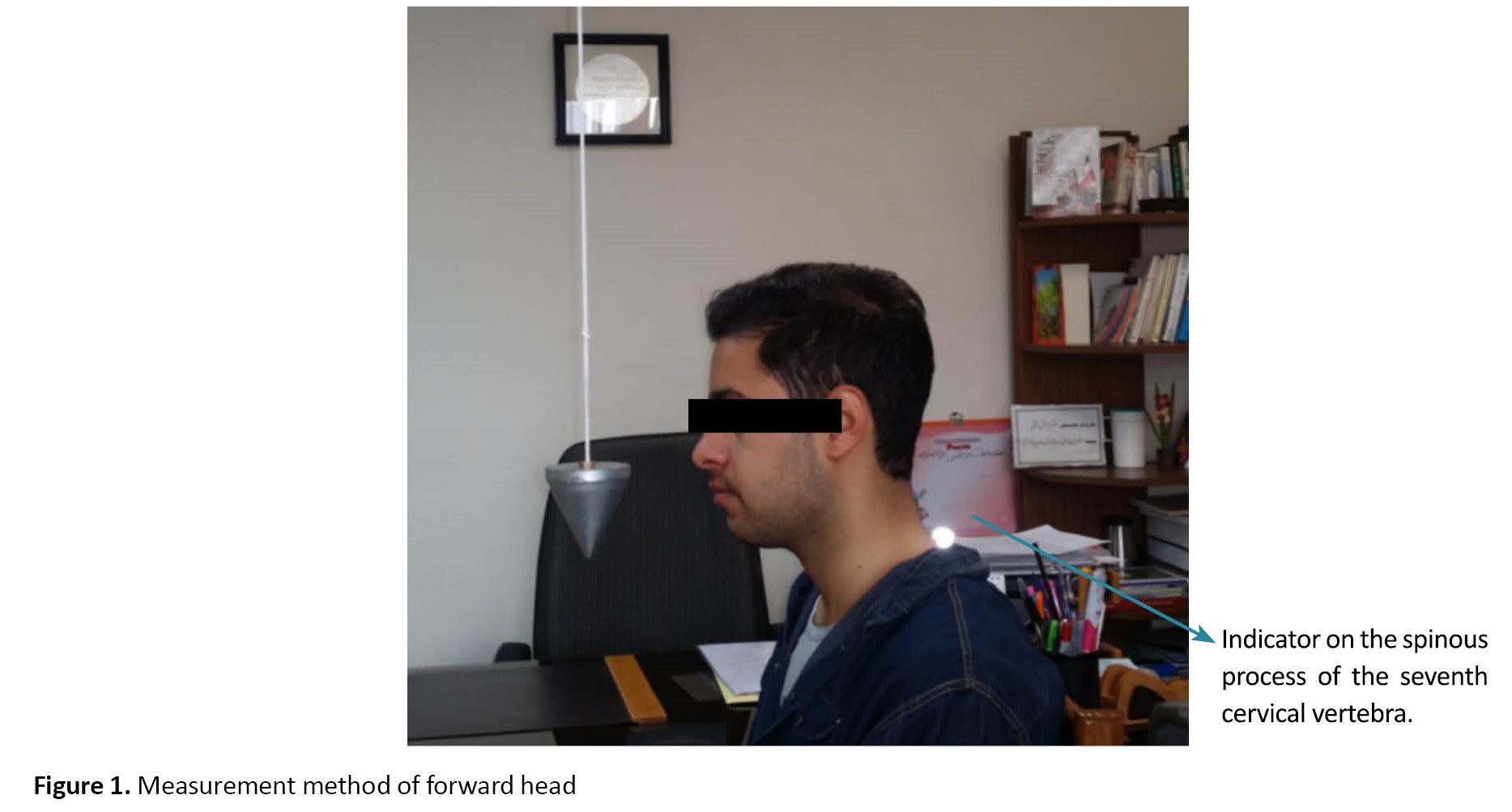 Three photos were selected, and the presence or absence of FHP was determined by the MB Ruler software. In this software, the craniovertebral angle is drawn using the mid-point between the indicator placed on the spinous process of the seventh cervical vertebra and the ear tragus. The average of three measurements was used in the statistical analyses.
Three photos were selected, and the presence or absence of FHP was determined by the MB Ruler software. In this software, the craniovertebral angle is drawn using the mid-point between the indicator placed on the spinous process of the seventh cervical vertebra and the ear tragus. The average of three measurements was used in the statistical analyses.
If the presence of FHP was diagnosed and confirmed, the participants were referred to the audiology clinic of the School of Rehabilitation, and audiometry and tympanometry were performed. The normal hearing standard in all the studied patients was the pure-tone hearing threshold equal to or higher than 25 dB HL at octave frequencies in the range of 250-8000 Hz in both ears. The hearing loss was classified as follows, mild hearing loss: 25-40 dB HL, moderate hearing loss: 41-55 dB HL, moderate-to-severe hearing loss: 56-70 dB HL, severe hearing loss: 71-90 dB HL, and profound hearing loss: 91 dB HL or above.
The results are presented as mean and standard deviation. The data were analyzed using SPSS software, version 18. The statistical methods included analysis of variance (ANOVA), independent t-test, and the chi-square test, at a significance level of α≤0.05.
Results
Table 1 presents the demographic characteristics of the participants.
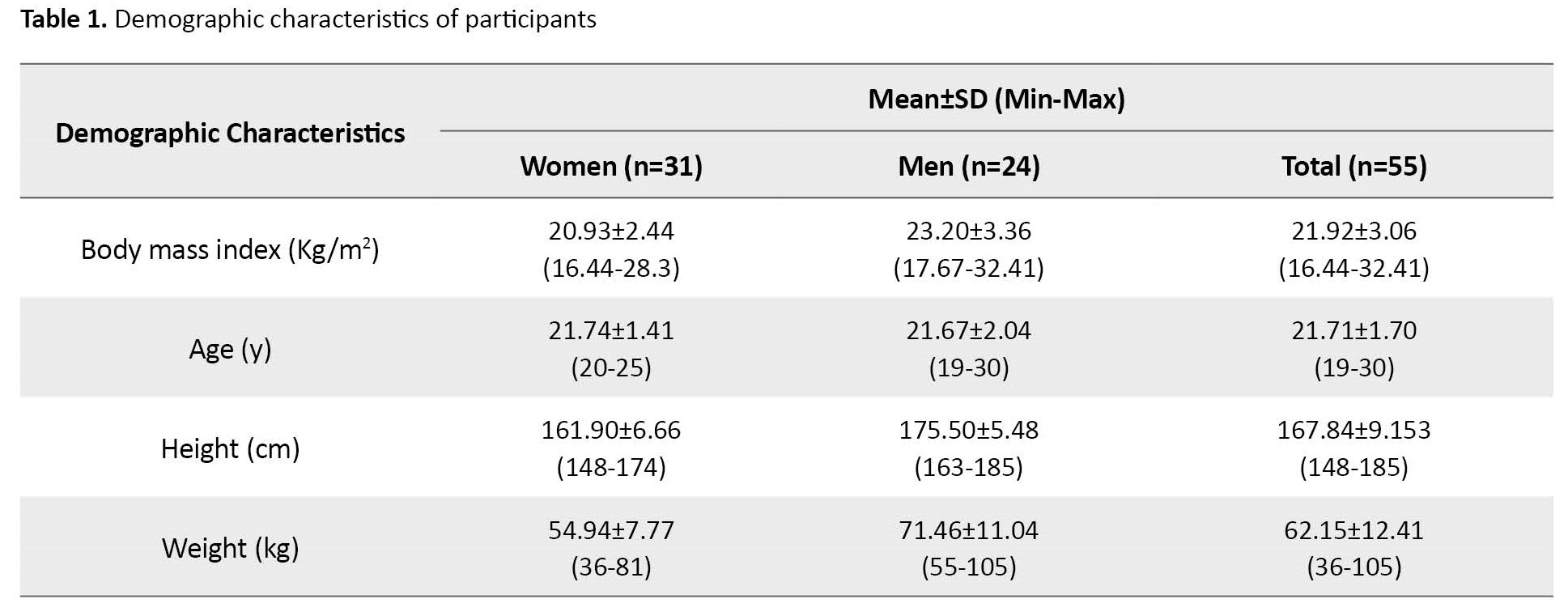
In this study, 31 women (56.4%) with a mean age of 21.74±1.41 years, and 24 men (43.6%) with a mean age of 21.67±2.04 years participated. FHP was observed in 24 women (77.42% of women) and 21 men (87.5% of men).
Table 2 presents the distribution of FHP based on sex and FHP severity.
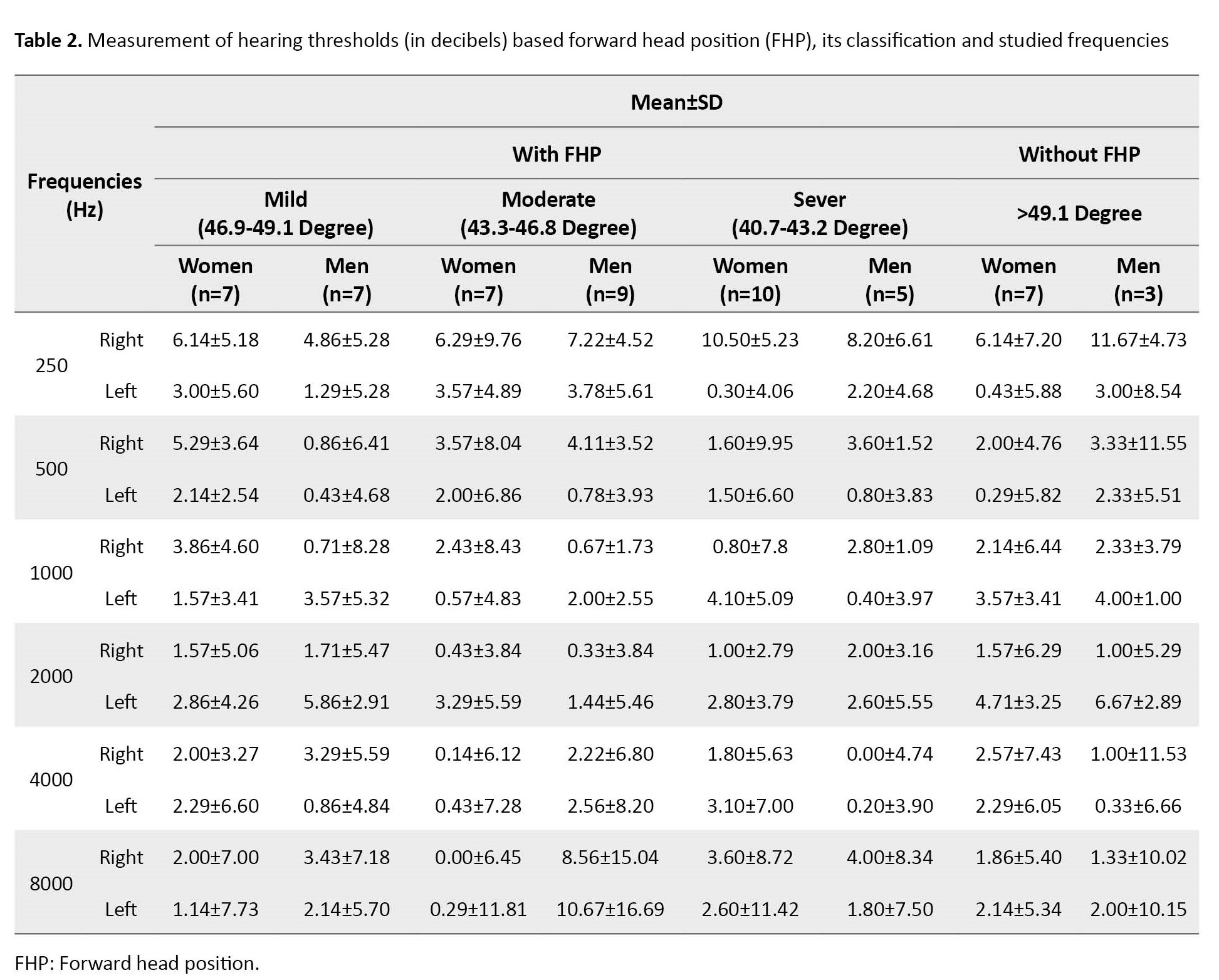
In this study, the craniovertebral angle (whose value indicates FHP) was classified into three groups, mild FHP range: 46.9-49.1 degrees, moderate FHP range: 43.3-46.8 degrees, and severe FHP range: 40.7-43.2 degrees. Using the chi-square test, no statistically significant difference was observed between men and women with FHP alone and according to its classification. In this study, no statistically significant difference was observed between FHP and its classification with hearing thresholds (P<0.05)
In women, the number of severe FHP cases was twice that of men (Table 2). At most frequencies, the left ear showed more sensitivity to pure tone than the right ear.
Discussion
Based on the results, no significant relationship was observed between FHP and hearing loss at different frequencies used in routine hearing tests, and no significant difference was observed between men and women in terms of having FHP based on its classification.
In the study conducted by Melo et al. [10], in adolescents with sensory/neural hearing loss, more changes to the head posture were observed compared to adolescents with normal hearing. In their study, over half of the participants with hearing loss had FHP. Based on the results of the present study, given the absence of hearing loss at different frequencies in people with different severities of FHP, and the results of Melo et al., it can be concluded that hearing loss leads to changes in the head position resulting in FHP. Therefore, it can be suggested that the healthcare team pay more attention to the head position and prevent FHP during the examination and treatment of hearing loss and it is recommended to maintain the proper head position.
In the present study, FHP had a relatively high prevalence among the participants. Various causes have been suggested for the incidence of FHP, including continued use of computers, watching the television, playing video games, and even wearing backpacks [1]. In this study, the participants were students and had a high degree of exposure to factors affecting the occurrence of FHP; therefore the high incidence of this position in them is not surprising. It can be concluded that this problem occurs in most students due to wrong positions in sitting, reading, and sleeping. According to Rajabi et al.’s study, a high incidence of FHP was observed among the different educational levels of students and they concluded that “increasing forward head posture angle in students after undergraduate and in postgraduate level may be due to educational background, longer study time, extended laptop work, carrying heavy backpacks (with books and laptop), and reduced physical activity due to heavier educational demands” [11].
In this study, no hearing loss was observed at the mean of any frequency despite the presence of FHP. However, at two frequencies of 4000 and 8000 Hz, the mean hearing thresholds in moderate FHP were higher than in mild and severe FHP, and at the frequency of 8000 Hz, the mean hearing thresholds in the right ear in men were higher than in women in all types of FHP. In most frequencies, the left ear showed more sensitivity to pure tone than the right ear, and this could be because most participants were right-handed and, therefore used the right ear more.
Neck rotation movement occurs mostly in the upper part of the neck, and its limitation highly affects the arteries and nerves involved in hearing. Most motor limitations of the cervical vertebral column, including its rotation, occur at ages over 35 years and are caused by various factors [12], and may lead to hearing loss [13]. Given the age of the participants in this study and that hearing loss in neck injuries occurs at older ages, and based on the study conducted by Melo et al. [10], it appears that FHP occurs after hearing loss, and FHP alone does not cause hearing loss at younger ages. Since the participants were young, more studies with a wider age range should be conducted on this topic.
Conclusion
Since the volunteers are students and are faced with factors affecting the occurrence of FHP, a large number of them (81.8%) suffer from FHP. Based on the results of the present study, given the absence of hearing loss at different frequencies (in different severities of FHP), it can be concluded that hearing loss leads to changes in the head position resulting in FHP.
One of the limitations of the present study was that neck health was determined only based on the participant’s self-report about the absence of any problem in the neck, and radiographic images were not used for this purpose.
It is recommended to repeat this study on a larger sample and at different age ranges and compare students with non-students.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by Iran University of Medical Sciences (Code: 90-01-125-13152).
Funding
The paper was extracted from a research project of Behnoosh Vasaghi-Gharamaleki, Department of Basic Sciences in Rehabilitation, Iran University of Medical Sciences.
Authors' contributions
Conceptualisation and study design: Mahbobeh Fallahian and Behnoosh Vasaghi-Gharamaleki; Data collection, Drafting the manuscript: Mahbobeh Fallahian; Data analysis, critical revision of the article and final approval: Behnoosh Vasaghi-Gharamalek; Data interpretation: Syeed Ali-Asghar Shirazi and Behnoosh Vasaghi-Gharamalek; Revision of the article: Syeed Ali-Asghar Shirazi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the participants.
References
Today’s industrialized life and non-ergonomic design of various devices in use result in a major problem, namely, the development of injuries and abnormalities in the vertebral column due to the incorrect use of muscles. One such abnormality is the forward head posture (FHP). FHP is defined as the forward displacement of lower cervical vertebrae and over-extension of upper cervical vertebrae that increase the effect of gravitational forces on the head [1]. Continued use of computer and television, playing video games, and even wearing backpacks, place the head in the anterior position and displace one’s line of sight downwards. To correct the line of sight, the person adjusts their body by assuming a head-forward position, which leads to FHP [1, 2].
FHP is one of the most prevalent positional abnormalities of the vertebral column, with a prevalence of 66%, and is classified as a chronic pain syndrome [3]. The side effects of FHP include cervical nervous system problems, temporomandibular joint misalignment and disorders in chewing, increased pressure on blood vessels and reduced vertebral blood flow to the brain, and brain stem [4, 5, 6]. The ear receives its blood supply from several arteries; parts of the inner ear are supplied by a branch of the labyrinthine artery which originates from the anterior inferior and posterior inferior cerebellar arteries. These two arteries are among the branches of the basilar artery, and the basilar artery is formed by joining the two vertebral arteries. Vertebrobasilar artery ischemia, especially obstruction of the anterior inferior cerebellar artery or one of its branches, can result in bilateral hearing loss regardless of age [7, 8, 9].
If the forward head can damage the neck structures, can it also cause hearing loss? To answer this question, this study was designed to examine the effects of the presence of FHP on hearing thresholds in students. It also investigated the effect of FHP severity on hearing thresholds.
Materials and Methods
In this cross-sectional study, 55 students (31 women aged 20-25 years, and 24 men aged 20-31 years) participated voluntarily. The study protocol was supported by the Iran University of Medical Sciences (IUMS) (90-01-125-13152). The study was conducted in the audiology clinic of Iran University of Medical Sciences. All participants provided written informed consent and then completed a questionnaire, including general questions (sex, year of birth, height, weight and…) and specialized questions on hearing risk factors. The exclusion criteria included the presence of compacted or semi-compacted earwax, a history of trauma to the ear, ear pain, a sense of fullness and pressure in the ear, tinnitus, vertigo, a history of taking any ototoxic medications, and a history of prolonged use of hands-free devices at high volume. The only inclusion criterion was verbal and written consent for participation.
To measure FHP, the participants sat on a chair (which was the same for all the participants) and were asked to look forward. Then, the indicator was placed on the spinous process of the seventh cervical vertebra, and six profile photos were taken from a 1.5 m distance by a digital camera (Figure 1).
If the presence of FHP was diagnosed and confirmed, the participants were referred to the audiology clinic of the School of Rehabilitation, and audiometry and tympanometry were performed. The normal hearing standard in all the studied patients was the pure-tone hearing threshold equal to or higher than 25 dB HL at octave frequencies in the range of 250-8000 Hz in both ears. The hearing loss was classified as follows, mild hearing loss: 25-40 dB HL, moderate hearing loss: 41-55 dB HL, moderate-to-severe hearing loss: 56-70 dB HL, severe hearing loss: 71-90 dB HL, and profound hearing loss: 91 dB HL or above.
The results are presented as mean and standard deviation. The data were analyzed using SPSS software, version 18. The statistical methods included analysis of variance (ANOVA), independent t-test, and the chi-square test, at a significance level of α≤0.05.
Results
Table 1 presents the demographic characteristics of the participants.
In this study, 31 women (56.4%) with a mean age of 21.74±1.41 years, and 24 men (43.6%) with a mean age of 21.67±2.04 years participated. FHP was observed in 24 women (77.42% of women) and 21 men (87.5% of men).
Table 2 presents the distribution of FHP based on sex and FHP severity.
In this study, the craniovertebral angle (whose value indicates FHP) was classified into three groups, mild FHP range: 46.9-49.1 degrees, moderate FHP range: 43.3-46.8 degrees, and severe FHP range: 40.7-43.2 degrees. Using the chi-square test, no statistically significant difference was observed between men and women with FHP alone and according to its classification. In this study, no statistically significant difference was observed between FHP and its classification with hearing thresholds (P<0.05)
In women, the number of severe FHP cases was twice that of men (Table 2). At most frequencies, the left ear showed more sensitivity to pure tone than the right ear.
Discussion
Based on the results, no significant relationship was observed between FHP and hearing loss at different frequencies used in routine hearing tests, and no significant difference was observed between men and women in terms of having FHP based on its classification.
In the study conducted by Melo et al. [10], in adolescents with sensory/neural hearing loss, more changes to the head posture were observed compared to adolescents with normal hearing. In their study, over half of the participants with hearing loss had FHP. Based on the results of the present study, given the absence of hearing loss at different frequencies in people with different severities of FHP, and the results of Melo et al., it can be concluded that hearing loss leads to changes in the head position resulting in FHP. Therefore, it can be suggested that the healthcare team pay more attention to the head position and prevent FHP during the examination and treatment of hearing loss and it is recommended to maintain the proper head position.
In the present study, FHP had a relatively high prevalence among the participants. Various causes have been suggested for the incidence of FHP, including continued use of computers, watching the television, playing video games, and even wearing backpacks [1]. In this study, the participants were students and had a high degree of exposure to factors affecting the occurrence of FHP; therefore the high incidence of this position in them is not surprising. It can be concluded that this problem occurs in most students due to wrong positions in sitting, reading, and sleeping. According to Rajabi et al.’s study, a high incidence of FHP was observed among the different educational levels of students and they concluded that “increasing forward head posture angle in students after undergraduate and in postgraduate level may be due to educational background, longer study time, extended laptop work, carrying heavy backpacks (with books and laptop), and reduced physical activity due to heavier educational demands” [11].
In this study, no hearing loss was observed at the mean of any frequency despite the presence of FHP. However, at two frequencies of 4000 and 8000 Hz, the mean hearing thresholds in moderate FHP were higher than in mild and severe FHP, and at the frequency of 8000 Hz, the mean hearing thresholds in the right ear in men were higher than in women in all types of FHP. In most frequencies, the left ear showed more sensitivity to pure tone than the right ear, and this could be because most participants were right-handed and, therefore used the right ear more.
Neck rotation movement occurs mostly in the upper part of the neck, and its limitation highly affects the arteries and nerves involved in hearing. Most motor limitations of the cervical vertebral column, including its rotation, occur at ages over 35 years and are caused by various factors [12], and may lead to hearing loss [13]. Given the age of the participants in this study and that hearing loss in neck injuries occurs at older ages, and based on the study conducted by Melo et al. [10], it appears that FHP occurs after hearing loss, and FHP alone does not cause hearing loss at younger ages. Since the participants were young, more studies with a wider age range should be conducted on this topic.
Conclusion
Since the volunteers are students and are faced with factors affecting the occurrence of FHP, a large number of them (81.8%) suffer from FHP. Based on the results of the present study, given the absence of hearing loss at different frequencies (in different severities of FHP), it can be concluded that hearing loss leads to changes in the head position resulting in FHP.
One of the limitations of the present study was that neck health was determined only based on the participant’s self-report about the absence of any problem in the neck, and radiographic images were not used for this purpose.
It is recommended to repeat this study on a larger sample and at different age ranges and compare students with non-students.
Ethical Considerations
Compliance with ethical guidelines
The study protocol was approved by Iran University of Medical Sciences (Code: 90-01-125-13152).
Funding
The paper was extracted from a research project of Behnoosh Vasaghi-Gharamaleki, Department of Basic Sciences in Rehabilitation, Iran University of Medical Sciences.
Authors' contributions
Conceptualisation and study design: Mahbobeh Fallahian and Behnoosh Vasaghi-Gharamaleki; Data collection, Drafting the manuscript: Mahbobeh Fallahian; Data analysis, critical revision of the article and final approval: Behnoosh Vasaghi-Gharamalek; Data interpretation: Syeed Ali-Asghar Shirazi and Behnoosh Vasaghi-Gharamalek; Revision of the article: Syeed Ali-Asghar Shirazi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the participants.
References
- Sahrmann S. Movement system impairment syndromes of the extremities, cervical and thoracic spines. Amsterdam: Elsevier Health Sciences; 2010. [Link]
- Nejati P, Lotfian S, Moezy A, Nejati M. The study of correlation between forward head posture and neck pain in Iranian office workers. Int J Occup Med Environ Health. 2015; 28(2):295-303. [DOI:10.13075/ijomeh.1896.00352] [PMID]
- Griegel-Morris P, Larson K, Mueller-Klaus K, Oatis CA. Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Phys Ther. 1992, 72;6(1):425-31. [DOI:10.1093/ptj/72.6.425] [PMID]
- Norkin CC, Levangie PK. Joint structure and function: A comprehensive analysis. Philadelphia: F.A. Davis. 2005. [Link]
- Ohmure H, Miyawaki S, Nagata J, Ikeda K, Yamasaki K, Al-Kalaly A. Influence of forward head posture on condylar position. J Oral Rehabil. 2008, 35(11):795-800. [DOI:10.1111/j.1365-2842.2007.01834.x] [PMID]
- Omran NG, Yousef AM, Hamada HA, Matar AG, Osman D. Effect of forward head posture on temporomandibular joint proprioception in post pubertal females: An observational study. Fizjoterapia Polska. 2019; 19(2):142-6. [Link]
- Amarenco P, Hauw JJ. Cerebellar infarction in the territory of the anterior and inferior cerebellar artery. A clinicopathological study of 20 cases. Brain. 1990; 113(Pt 1):139-55. [DOI:10.1093/brain/113.1.139] [PMID]
- Yamasoba T, Kikuchi S, Higo R. Deafness associated with vertebrobasilar insufficiency. J Neurol Sci. 2001; 187(1-2):69-75. [DOI:10.1016/S0022-510X(01)00525-1] [PMID]
- Kumral E, Kisabay A, Ataç C. Lesion patterns and etiology of ischemia in the anterior inferior cerebellar artery territory involvement: A clinical - diffusion weighted - MRI study. Eur J Neurol. 2006; 13(4):395-401. [DOI:10.1111/j.1468-1331.2006.01255.x] [PMID]
- Melo Rde S, Amorim da Silva PW, Souza RA, Raposo MC, Ferraz KM. Head position comparison between students with normal hearing and students with sensorineural hearing loss. Int Arch Otorhinolaryngol. 2013; 17(4):363-9. [DOI:10.1055/s-0033-1351685] [PMID] [PMCID]
- Rajabi R, Karimizadeh Ardakani M, Minoonejad H, Abshenas E, Naderi Beni M. Comparison of the average forward head angle of male and female students in three educational levels. J Rehabil Sci Rese. 2020; 7(4):184-8. [Link]
- Hasler RM, Exadaktylos AK, Bouamra O, Benneker LM, Clancy M, Sieber R, et al. Epidemiology and predictors of cervical spine injury in adult major trauma patients: A multicenter cohort study. J Trauma Acute Care Surg. 2012; 72(4):975-81. [DOI:10.1097/TA.0b013e31823f5e8e] [PMID]
- Vasaghi-Gharamaleki B, Naser Z. Predicting the risk of hearing impairment following the cervical spine diseases by measuring the cervical range of movements: A pilot study. Basic Clin Neurosci. 2017; 8(5):413-8. [DOI:10.18869/nirp.bcn.8.5.413] [PMID] [PMCID]
Type of Study: Research |
Subject:
Audiology
Received: 2023/04/10 | Accepted: 2023/07/2 | Published: 2023/02/6
Received: 2023/04/10 | Accepted: 2023/07/2 | Published: 2023/02/6
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.