

Volume 5, Issue 1 (Continuously Updated 2022)
Func Disabil J 2022, 5(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ebadi E, Jarollahi F, Ahadi M, Tahaie A, Hosseini A. Identification of Auditory Processing Disorder Based on the Persian Version of Multiple Auditory Processing Assessment in School-aged Children in Arak City, Iran. Func Disabil J 2022; 5 (1) : 75
URL: http://fdj.iums.ac.ir/article-1-213-en.html
URL: http://fdj.iums.ac.ir/article-1-213-en.html



1- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,f@iums.ac.ir
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Audiology, Rehabilitation Research Center, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
3- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Central auditory processing disorder, Central auditory nervous system, School aged children, Multiple auditory processing assessment (MAPA)
Full-Text [PDF 1177 kb]
(159 Downloads)
| Abstract (HTML) (278 Views)
Full-Text: (106 Views)
Introduction
Central auditory processing disorder (CAPD) can be one of the reasons for children’s behavioral-functional problems, which harms learning, language development, communication, and crucial functions related to processing, listening, and understanding spoken language, especially in challenging listening environments, such as the presence of background noise causing a lot of problems [1-4]. The most specific symptoms in children with APD appear when they enter school, which include poor listening skills, difficulty understanding speech in noisy environments, frequent requests to repeat material, difficulty processing rapid speech, and responding inappropriately or late. Rapid distraction with environmental stimuli is common in these children and they have difficulty in tasks, such as following sequential orders, spelling, reading, pronunciation, and learning, accompanied by the inability to focus on auditory events and feeling tired after listening to speech, causing severe educational problems for these children in school [1, 5]. These children have normal hearing thresholds despite listening and learning problems related to incomplete processing of auditory information; therefore, they cannot be recognized by the peripheral hearing screening program and need special evaluations. Also, due to the complex nature of this disorder, to evaluate and diagnose it, a test battery should be used that is capable of evaluating multiple auditory processes and mechanisms at different levels of the central auditory nervous system. In addition to being practical and efficient, these tests should have a high correlation and facilitate differential diagnosis. Therefore, a single test will not have enough sensitivity to diagnose this disorder [6-10].
Using a comprehensive test battery approach to evaluate all auditory processes helps the therapist identify the strengths and weaknesses of the individual’s AP. In this way, the audiologist should choose valid tests which can find a perspective on the existing APD while examining different processes and behaviors in the central auditory nervous system in different levels. So far, two standard test batteries have been introduced under the titles of The screening test for auditory processing disorders in children (SCAN-C) [11] and multiple auditory processing assessment (MAPA) [7] for APD screening in children. Studies have shown that APD originates from three domains of auditory processing, i.e. monaural hearing, binaural hearing, and temporal processing, and the MAPA model has shown more valid results than the SCAN-C model [6, 8, 9]. In the present study, the standard Persian version of MAPA (MAPA-P) [12] was used. The set of MAPA-P tests includes a monaural-selective auditory attention test (MSAAT) [13], TAP test, pitch pattern test, dichotic digits test, and competing sentences test.
Although the prevalence of APD in children is high [14, 15], according to the age of the samples, the type of used tests, and different methodologies, these results are very different so that Schow et al. have estimated the percentage of APD 1%-2% and mentioned that if more accurate tests are used, its amount may increase [7]. In other sources, APD’s prevalence rate was 2% to 5% [9]. Or another researcher considered the best approximation of the prevalence of APD in the population of school-aged children to be around 20% [10].
Using the APD questionnaire (APDQ), Jarollahi et al obtained this rate to be 4.6% in school-aged children in Tehran City, Iran [16]. Therefore, considering the high prevalence of APD in children and the importance of learning, especially in elementary school, which takes place through the ears to a significant extent [16-22], currently, the diagnosis and treatment of APD, especially in children, is one of the priorities of audiology research in the world. Therefore, it is necessary to identify children with a kind of APD by adopting a suitable process so that the possibility of early rehabilitation intervention can be provided to ultimately lead to solving their learning and academic problems in educational settings [23, 24]. Considering the influence of demographic characteristics and the availability of the valid Persian version of the MAPA test battery, a study was conducted to determine the frequency of APD in children aged 9 to 12 years in Arak City, Iran.
Materials and Methods
The current study was carried out using a cross-sectional descriptive-analytical method. After attending school and settling in a suitable place in terms of the absence of auditory and visual distractions, a class was selected completely randomly to evaluate students. Before their assessment, the informed consent form was read and signed by the parents. A person’s left-handed or right-handedness was also determined by the Edinburgh questionnaire. After conducting a short interview to obtain the child’s consent and prepare him/her to participate in the tests, first, otoscopy examinations were done using the Welch Allyn otoscope to check the condition of the external auditory canal and tympanic membrane. Then tympanoscopy was performed using the HAND TYMP device brand REXTON, made in Denmark, to check the middle ear as well as using the Pejvak Ava device SA78B model for screening audiometry, to check the peripheral hearing status of these people. A total of 324 students aged 9 to 12 from 7 primary schools in Arak City, Iran were included in the study. Twenty-four students were excluded from the study due to not meeting the inclusion criteria. The inclusion criteria included obtaining normal results in the peripheral hearing screening test (PTA) at the intensity level of 20dBHL in frequencies from 500 to 4000 Hz and type A typmanogram -50<TPP1<+50 (daPa) and 0.3<Ytm2 <1.6 (mmho) in both ears [17], having fluent speech without stuttering and declaring cooperation and not being tired by the child to do the tests.
In the next step, the MAPA-P test battery was used for central auditory evaluations with the implementation instructions and practice materials that were available in the form of a compiled set on a CD [12]. Before performing each test, its instruction was explained to the individual, and by using practice items, it was ensured that the individual fully understood and correctly performed the test. The above tests were performed using a laptop and supra-aural headphones, a4TECH HS_800 model. At the beginning of each session, the volume of the laptop in headphones was controlled at a comfortable hearing level. Simultaneously with the person’s answer, the answers are registered in the “MAPA answer registration form”.
1. TPP: Tympanometric peak pressure
2. Ytm: Admittance at the tympanic membrane
In this study, the mean and standard deviation of each age group were used to analyze the descriptive data. Then, the normality of the variables was checked using the Kolmogorov-Smirnov statistical test, after that, an independent t-test was used to compare the different scores between the two genders. The analysis of variance (ANOVA) was used to compare the results in different age groups. Data were analyzed using SPSS software, version 22.
Results
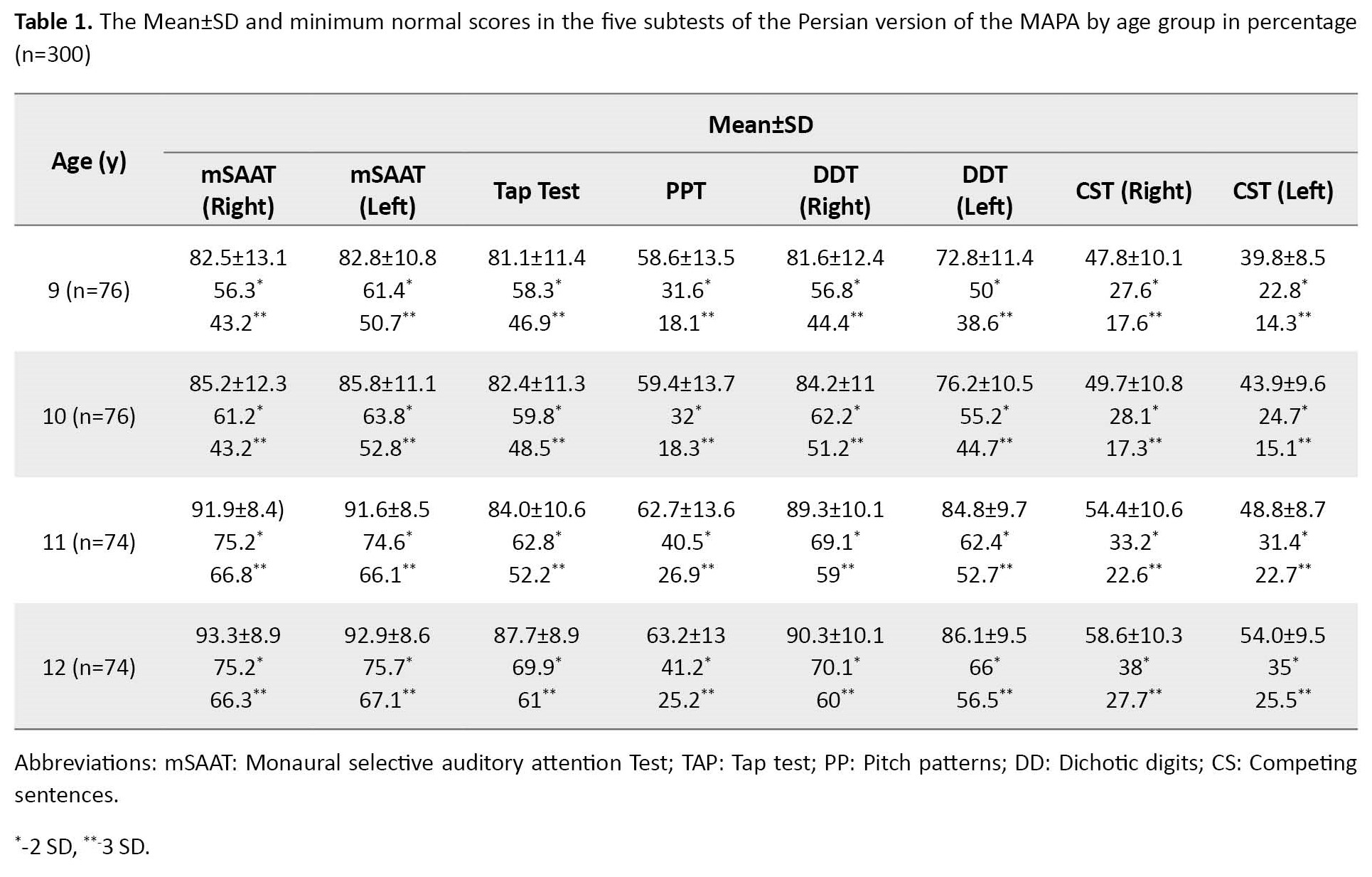
In this study, 300 students with a Mean±SD of age of 10.48±1.11 years were examined. Seventy-six children (25.3%) were 9 years old, 76 children (25.3%) were 10 years old, 74 children (24.7%) were 11 years old, and 74 children (24.7%) were 12 years old. A total of 150 children (50%) were girls and the others were boys; 289 children (96.3%) were right-handed and the others were left-handed. The results of one-way analysis of variance (ANOVA) showed that the mean scores in all five tests had statistically significant differences at different ages. The results of the post hoc Games-Howell test showed that the mean scores increase with age (P<0.0001), Table 1 presents the results of this part.
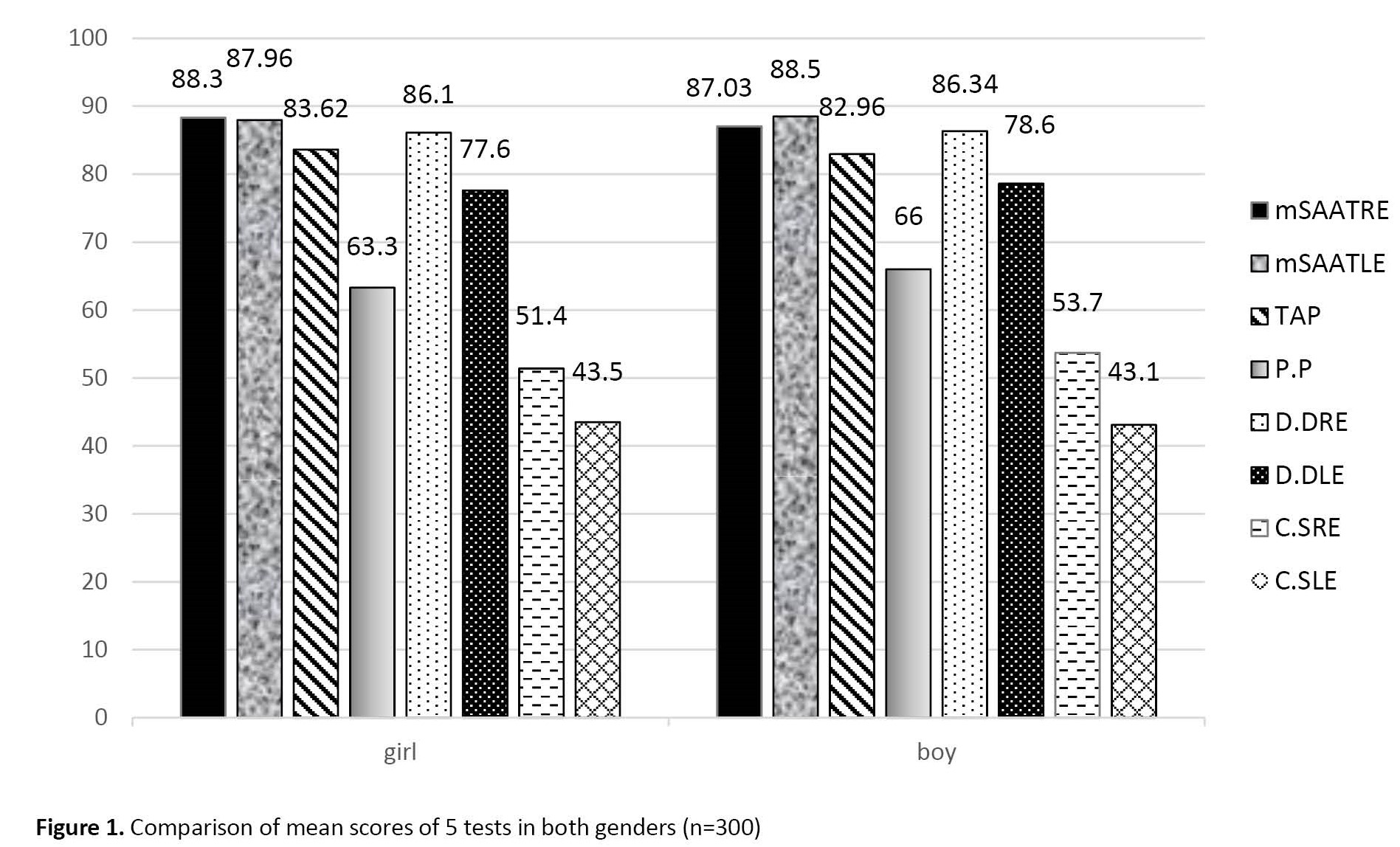
Also, the results of the independent t-test showed no statistically significant difference in the mean scores in any of the five tests in both genders (P>0.05) (Figure 1).
 After calculating the mean scores for the tests in each age group, according to the statement of ASHA (2005) for the necessity of having a cut-off point, based on the cut-off point of all five tests in different age groups, the frequency of APD was determined. The range of norm values for the percentage of correct answers of five tests of the Persian version of the “MAPA” collection, by considering two standard deviations below the mean (lower limit of 95% confidence limits) for two tests and 3 standard deviations below the mean (lower limit of 99% confidence limits) for one test was calculated. To interpret the results of the tests and identify children suspected of having a central auditory processing disorder, according to the statement of ASHA (2005), considering at least 3 standard deviations below the mean for one test and at least 2 standard deviations below the mean for two tests can be used.
After calculating the mean scores for the tests in each age group, according to the statement of ASHA (2005) for the necessity of having a cut-off point, based on the cut-off point of all five tests in different age groups, the frequency of APD was determined. The range of norm values for the percentage of correct answers of five tests of the Persian version of the “MAPA” collection, by considering two standard deviations below the mean (lower limit of 95% confidence limits) for two tests and 3 standard deviations below the mean (lower limit of 99% confidence limits) for one test was calculated. To interpret the results of the tests and identify children suspected of having a central auditory processing disorder, according to the statement of ASHA (2005), considering at least 3 standard deviations below the mean for one test and at least 2 standard deviations below the mean for two tests can be used.
The results showed that among 300 children, 15 people were suspected of APD. This number made up 5% of the sample size, which included six 9-year-old children, four 10-year-old children, three 11-year-old children, and two 12-year-old children. Table 2 presents the results.

Discussion
The present study was conducted to identify children suspected of APD in the school population aged 9-12 years using the Persian version of the MAPA. According to the results obtained, in all five tests, the mean scores in different age groups had a significant difference and increased with increasing age (P=0.0001). Also, no significant difference was observed between the mean scores of the two genders.
In research using the MAPA tests on 8-11-year-old school children, it was shown that by increasing age, the mean scores in all tests and both genders increased [6], which is consistent with the findings of the present study. Conlin also used the MAPA tests to evaluate children aged 9-13 years. The results of this study also showed that the mean scores increased with increasing age [21], which was consistent with the results of the present study.
According to Table 1, the mean scores in all 5 tests in both genders increased with age. These results were not far from expected, because with the maturation of the auditory system and the development of the cerebral hemispheres and interhemispheric pathways along with the growth of the child, as well as the improvement of auditory attention and memory with age, the auditory processing functions of people will improve. This improvement with age leads to an increase in test scores [22].
In the current study, after calculating the mean scores of the tests in each age group, according to the statement of ASHA (2005), the cut-off point was determined for all five tests and in different age groups. According to the results, among the 300 children, 15 children were suspected of APD. This number makes up 5% of the total sample size. According to the American Speech-Language-Hearing Association (ASHA) statement (2005), criteria of at least 3 standard deviations below the mean for one test and 2 standard deviations below the mean for two tests were used to diagnose APD [1].
The minimum prevalence of APD in school-age children was 2%-3%, and it has been emphasized that if more accurate tests are used, this amount may increase [7]. In some texts, the prevalence of this disorder in school-age children is mentioned to be 5% [19, 20]. Also, some studies have mentioned the real value of this disorder as 7% [9]. According to Katz et al, the best estimate of the prevalence of central auditory processing disorder in school-age children is about 20% [20]. The prevalence of the current study was consistent with most studies [7, 20].
In the examination of the educational histories of 15 children suspected of APD, it was found that 11 of them had a history of learning disorder and were under special training for this disorder. In other words, 73.3% of the children suspected of APD were children whose learning disorders were reported. Also, the examination of the central processing monitoring questionnaire that was completed by the parents of these children showed that the academic performance of these children was reported to be poor. In other studies, the prevalence of APD in children with learning disabilities has been reported to be 30%-50% in studies [17, 23-25], and Tillery reported it to be 80% [26]. The results of the present study also showed that the frequency of children suspected of APD is higher in children with learning disabilities, which is consistent with Tillery’s results [26].
Conclusion
Based on the findings of the present study, the clinical capability of the Persian version of MAPA, including 5 subtests in three main domains of central auditory processing, can be used as a valid model to evaluate the central auditory system in 9-12-year-old school-aged children in both boys and girls. In addition, its non-invasiveness and low cost facilitate the clinical application of this test battery. The frequency of APD in the population of school children aged 9-12 years in Arak City was 5%. To further validate MAPA-P, it is suggested to conduct similar studies in other age groups, different cities, and also in other disorders, such as children with learning disability, autism spectrum disorder, etc.
Ethical Considerations
Compliance with ethical guidelines
This article is the result of a research project that approved by Ethics Committee of the Research Vice-Chancellor of Iran University of Medical Sciences (Code: 93/340/1757).
Funding
The paper was extracted from the MSc thesis of Ensieh Ebadi, approved by Department of Audiology, Iran University of Medical Sciences.
Authors' contributions
Preparation, data collection, interpretation and analysis of results and writing: Ensieh Ebadi; Plan design, article editing: Farnoush Jarollahi; Test construction: Mohsen Ahadi; Test construction: Aliakbar Tahaie; Statistical analysis: Aghafatemeh Hosseini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all the children and families who participated in this research.
References
Central auditory processing disorder (CAPD) can be one of the reasons for children’s behavioral-functional problems, which harms learning, language development, communication, and crucial functions related to processing, listening, and understanding spoken language, especially in challenging listening environments, such as the presence of background noise causing a lot of problems [1-4]. The most specific symptoms in children with APD appear when they enter school, which include poor listening skills, difficulty understanding speech in noisy environments, frequent requests to repeat material, difficulty processing rapid speech, and responding inappropriately or late. Rapid distraction with environmental stimuli is common in these children and they have difficulty in tasks, such as following sequential orders, spelling, reading, pronunciation, and learning, accompanied by the inability to focus on auditory events and feeling tired after listening to speech, causing severe educational problems for these children in school [1, 5]. These children have normal hearing thresholds despite listening and learning problems related to incomplete processing of auditory information; therefore, they cannot be recognized by the peripheral hearing screening program and need special evaluations. Also, due to the complex nature of this disorder, to evaluate and diagnose it, a test battery should be used that is capable of evaluating multiple auditory processes and mechanisms at different levels of the central auditory nervous system. In addition to being practical and efficient, these tests should have a high correlation and facilitate differential diagnosis. Therefore, a single test will not have enough sensitivity to diagnose this disorder [6-10].
Using a comprehensive test battery approach to evaluate all auditory processes helps the therapist identify the strengths and weaknesses of the individual’s AP. In this way, the audiologist should choose valid tests which can find a perspective on the existing APD while examining different processes and behaviors in the central auditory nervous system in different levels. So far, two standard test batteries have been introduced under the titles of The screening test for auditory processing disorders in children (SCAN-C) [11] and multiple auditory processing assessment (MAPA) [7] for APD screening in children. Studies have shown that APD originates from three domains of auditory processing, i.e. monaural hearing, binaural hearing, and temporal processing, and the MAPA model has shown more valid results than the SCAN-C model [6, 8, 9]. In the present study, the standard Persian version of MAPA (MAPA-P) [12] was used. The set of MAPA-P tests includes a monaural-selective auditory attention test (MSAAT) [13], TAP test, pitch pattern test, dichotic digits test, and competing sentences test.
Although the prevalence of APD in children is high [14, 15], according to the age of the samples, the type of used tests, and different methodologies, these results are very different so that Schow et al. have estimated the percentage of APD 1%-2% and mentioned that if more accurate tests are used, its amount may increase [7]. In other sources, APD’s prevalence rate was 2% to 5% [9]. Or another researcher considered the best approximation of the prevalence of APD in the population of school-aged children to be around 20% [10].
Using the APD questionnaire (APDQ), Jarollahi et al obtained this rate to be 4.6% in school-aged children in Tehran City, Iran [16]. Therefore, considering the high prevalence of APD in children and the importance of learning, especially in elementary school, which takes place through the ears to a significant extent [16-22], currently, the diagnosis and treatment of APD, especially in children, is one of the priorities of audiology research in the world. Therefore, it is necessary to identify children with a kind of APD by adopting a suitable process so that the possibility of early rehabilitation intervention can be provided to ultimately lead to solving their learning and academic problems in educational settings [23, 24]. Considering the influence of demographic characteristics and the availability of the valid Persian version of the MAPA test battery, a study was conducted to determine the frequency of APD in children aged 9 to 12 years in Arak City, Iran.
Materials and Methods
The current study was carried out using a cross-sectional descriptive-analytical method. After attending school and settling in a suitable place in terms of the absence of auditory and visual distractions, a class was selected completely randomly to evaluate students. Before their assessment, the informed consent form was read and signed by the parents. A person’s left-handed or right-handedness was also determined by the Edinburgh questionnaire. After conducting a short interview to obtain the child’s consent and prepare him/her to participate in the tests, first, otoscopy examinations were done using the Welch Allyn otoscope to check the condition of the external auditory canal and tympanic membrane. Then tympanoscopy was performed using the HAND TYMP device brand REXTON, made in Denmark, to check the middle ear as well as using the Pejvak Ava device SA78B model for screening audiometry, to check the peripheral hearing status of these people. A total of 324 students aged 9 to 12 from 7 primary schools in Arak City, Iran were included in the study. Twenty-four students were excluded from the study due to not meeting the inclusion criteria. The inclusion criteria included obtaining normal results in the peripheral hearing screening test (PTA) at the intensity level of 20dBHL in frequencies from 500 to 4000 Hz and type A typmanogram -50<TPP1<+50 (daPa) and 0.3<Ytm2 <1.6 (mmho) in both ears [17], having fluent speech without stuttering and declaring cooperation and not being tired by the child to do the tests.
In the next step, the MAPA-P test battery was used for central auditory evaluations with the implementation instructions and practice materials that were available in the form of a compiled set on a CD [12]. Before performing each test, its instruction was explained to the individual, and by using practice items, it was ensured that the individual fully understood and correctly performed the test. The above tests were performed using a laptop and supra-aural headphones, a4TECH HS_800 model. At the beginning of each session, the volume of the laptop in headphones was controlled at a comfortable hearing level. Simultaneously with the person’s answer, the answers are registered in the “MAPA answer registration form”.
1. TPP: Tympanometric peak pressure
2. Ytm: Admittance at the tympanic membrane
In this study, the mean and standard deviation of each age group were used to analyze the descriptive data. Then, the normality of the variables was checked using the Kolmogorov-Smirnov statistical test, after that, an independent t-test was used to compare the different scores between the two genders. The analysis of variance (ANOVA) was used to compare the results in different age groups. Data were analyzed using SPSS software, version 22.
Results
In this study, 300 students with a Mean±SD of age of 10.48±1.11 years were examined. Seventy-six children (25.3%) were 9 years old, 76 children (25.3%) were 10 years old, 74 children (24.7%) were 11 years old, and 74 children (24.7%) were 12 years old. A total of 150 children (50%) were girls and the others were boys; 289 children (96.3%) were right-handed and the others were left-handed. The results of one-way analysis of variance (ANOVA) showed that the mean scores in all five tests had statistically significant differences at different ages. The results of the post hoc Games-Howell test showed that the mean scores increase with age (P<0.0001), Table 1 presents the results of this part.
Also, the results of the independent t-test showed no statistically significant difference in the mean scores in any of the five tests in both genders (P>0.05) (Figure 1).
The results showed that among 300 children, 15 people were suspected of APD. This number made up 5% of the sample size, which included six 9-year-old children, four 10-year-old children, three 11-year-old children, and two 12-year-old children. Table 2 presents the results.
Discussion
The present study was conducted to identify children suspected of APD in the school population aged 9-12 years using the Persian version of the MAPA. According to the results obtained, in all five tests, the mean scores in different age groups had a significant difference and increased with increasing age (P=0.0001). Also, no significant difference was observed between the mean scores of the two genders.
In research using the MAPA tests on 8-11-year-old school children, it was shown that by increasing age, the mean scores in all tests and both genders increased [6], which is consistent with the findings of the present study. Conlin also used the MAPA tests to evaluate children aged 9-13 years. The results of this study also showed that the mean scores increased with increasing age [21], which was consistent with the results of the present study.
According to Table 1, the mean scores in all 5 tests in both genders increased with age. These results were not far from expected, because with the maturation of the auditory system and the development of the cerebral hemispheres and interhemispheric pathways along with the growth of the child, as well as the improvement of auditory attention and memory with age, the auditory processing functions of people will improve. This improvement with age leads to an increase in test scores [22].
In the current study, after calculating the mean scores of the tests in each age group, according to the statement of ASHA (2005), the cut-off point was determined for all five tests and in different age groups. According to the results, among the 300 children, 15 children were suspected of APD. This number makes up 5% of the total sample size. According to the American Speech-Language-Hearing Association (ASHA) statement (2005), criteria of at least 3 standard deviations below the mean for one test and 2 standard deviations below the mean for two tests were used to diagnose APD [1].
The minimum prevalence of APD in school-age children was 2%-3%, and it has been emphasized that if more accurate tests are used, this amount may increase [7]. In some texts, the prevalence of this disorder in school-age children is mentioned to be 5% [19, 20]. Also, some studies have mentioned the real value of this disorder as 7% [9]. According to Katz et al, the best estimate of the prevalence of central auditory processing disorder in school-age children is about 20% [20]. The prevalence of the current study was consistent with most studies [7, 20].
In the examination of the educational histories of 15 children suspected of APD, it was found that 11 of them had a history of learning disorder and were under special training for this disorder. In other words, 73.3% of the children suspected of APD were children whose learning disorders were reported. Also, the examination of the central processing monitoring questionnaire that was completed by the parents of these children showed that the academic performance of these children was reported to be poor. In other studies, the prevalence of APD in children with learning disabilities has been reported to be 30%-50% in studies [17, 23-25], and Tillery reported it to be 80% [26]. The results of the present study also showed that the frequency of children suspected of APD is higher in children with learning disabilities, which is consistent with Tillery’s results [26].
Conclusion
Based on the findings of the present study, the clinical capability of the Persian version of MAPA, including 5 subtests in three main domains of central auditory processing, can be used as a valid model to evaluate the central auditory system in 9-12-year-old school-aged children in both boys and girls. In addition, its non-invasiveness and low cost facilitate the clinical application of this test battery. The frequency of APD in the population of school children aged 9-12 years in Arak City was 5%. To further validate MAPA-P, it is suggested to conduct similar studies in other age groups, different cities, and also in other disorders, such as children with learning disability, autism spectrum disorder, etc.
Ethical Considerations
Compliance with ethical guidelines
This article is the result of a research project that approved by Ethics Committee of the Research Vice-Chancellor of Iran University of Medical Sciences (Code: 93/340/1757).
Funding
The paper was extracted from the MSc thesis of Ensieh Ebadi, approved by Department of Audiology, Iran University of Medical Sciences.
Authors' contributions
Preparation, data collection, interpretation and analysis of results and writing: Ensieh Ebadi; Plan design, article editing: Farnoush Jarollahi; Test construction: Mohsen Ahadi; Test construction: Aliakbar Tahaie; Statistical analysis: Aghafatemeh Hosseini.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank all the children and families who participated in this research.
References
- American Speech-Language-Hearing Association. (Central) auditory processing disorders - The role of the audiologist. Maryland: American Speech-Language-Hearing Association; 2005. [Link]
- Yalçinkaya F, Muluk NB, Sahin S. Effects of listening ability on speaking, writing and reading skills of children who were suspected of auditory processing difficulty. International Journal of Pediatric Otorhinolaryngology. 2009; 73(8):1137-42. [DOI:10.1016/j.ijporl.2009.04.022] [PMID]
- Rosen S, Cohen M, Vanniasegaram I. Auditory and cognitive abilities of children suspected of auditory processing disorder (APD). International Journal of Pediatric Otorhinolaryngology. 2010; 74(6):594- 600. [DOI:10.1016/j.ijporl.2010.02.021] [PMID]
- Jerger J, Musiek F. Report of the consensus conference on the diagnosis of auditory processing disorders in school-aged children.Journal of the American Academy of Audiology. 2000; 11(9):467-74. [DOI:10.1055/s-0042-1748136] [PMID]
- Bamiou DE, Musiek FE, Luxon LM. Aetiology and clinical presentations of auditory processing disorders--a review. Archives of Disease in Childhood. 2001; 85(5):361-5. [DOI:10.1136/adc.85.5.361] [PMID] [PMCID]
- Domitz DM, Schow RL. A new CAPD battery--multiple auditory processing assessment: Factor analysis and comparisons with SCAN. American Journal of Audiology. 2000; 9(2):101-11. [DOI:10.1044/1059-0889(2000/012)] [PMID]
- Schow RL, Seikel JA, Chermak GD, Berent M. Central auditory processes and test measures ASHA 1996 Revisited. American Journal of Audiology. 2000; 9(2):63-8. [DOI:10.1044/1059-0889(2000/013)] [PMID]
- Lampe B. Are currently available pre-packaged behavioural test batteries (SCAN and MAPA) effective for use in the assessment and or diagnosis of auditory processing disorder (APD) in children assuming the American speech-language hearing association (ASHA) definition of APD? Ontario: University of Western Ontario; 2011. [Link]
- Cacace AT, McFarland DJ. Central auditory processing disorder in school-aged children: A critical review. Journal of Speech, Language, and Hearing Research. 1998; 41(2):355-73. [DOI:10.1044/jslhr.4102.355] [PMID]
- Geffner D, Ross-Swain D. Auditory processing disorders: Assessment, management and treatment. California: Plural Publishing; 2012. [Link]
- Keith RW. Scan: A screening test auditory processing disorders. San Diego: Harcourt Brace Jovanovich; 1986.
- Ebadi E, Jarollahi F, Tahaei AA, Ahadi M, Hosseini AF. Development and evaluation of the Persian version of the multiple auditory processing assessment. Auditory and Vestibular Research. 2016; 25(2):75-81. [Link]
- Aarabi S, Jarollahi F, Jalaie S. Development and determination of the validity of Persian version of monaural selective auditory attention test in learning disabled children. Auditory and Vestibular Research. 2016; 25(1):49-54. [Link]
- Musiek FE, Chermak GD. Handbook of central auditory processing disorder, volume I: Auditory neuroscience and diagnosis. California: Plural Publishing; 2013. [Link]
- Vanniasegaram I, Cohen M, Rosen S. Evaluation of selected auditory tests in school-age children suspected of auditory processing disorders. Ear and Hearing. 2004; 25(6):586-97. [DOI:10.1097/01.aud.0000151575.58269.19] [PMID]
- Jarollahi F, Pourbakht A, Jalaie Sh, Oruie M. Screening of auditory processing disorders in school- aged children in Tehran, Iran using the auditory processing domain questionnaire. Auditory and Vestibular Research Journal. 2022; 31(1):17-22. [DOI:10.18502/avr.v31i1.8130]
- Ahmadi Z, Jarollahi F, Ahadi M, Hosseini F, Khamisabadi S. Screening of auditory processing disorder in children with learning disabilities using the Persian version of the auditory processing domains questionnaire. Auditory and Vestibular Research. 2020; 29(3):156-4. [DOI:10.18502/avr.v29i3.3848]
- Jarollahi F, Jalaie S, Ahadi M, Ahmadi Z, Khamisabadi S. Clinical Application of the Persian Version of Buffalo Model Questionnaire by examining Its correlation with the Buffalo Model Test Battery. Auditory and Vestibular Research. 2023; 32(1):70-80. [DOI:10.18502/avr.v32i1.11325]
- Jerger J, Musiek F. Report of the consensus conference on the diagnosis of auditory processing disorders in school-aged children. Journal of the American Academy of Audiology. 2000; 11(9):467-74. [PMID]
- Katz J, Chasin M, English KM, Hood LJ, Tillery K. Handbook of clinical audiology. Philadelphia: Wolters Kluwer Health; 2015. [Link]
- Conlin, L. Form equivalency on the Beta III version of Multiple Auditory Processing Assessment (MAPA) [MS thesis]. Idaho: Idaho State University, Pocatello; 2003. [Link]
- Stollman M. Auditory processing in children: A study of the effects of age, hearing impairment and language impairment on auditory abilities in children [PhD dissertation]. Nijmegen: Universiteit Nijmegen; 2003. [Link]
- Iliadou V, Bamiou DE, Kaprinis S, Kandylis D, Kaprinis G. Auditory processing disorders in children suspected of learning disabilities- A need for screening? International Journal of Pediatric Otorhinolaryngology. 2009; 73(7):1029-34. [DOI:10.1016/j.ijporl.2009.04.004] [PMID]
- Rosen S, Cohen M, Vanniasegaram I. Auditory and cognitive abilities of children suspected of auditory processing disorder (APD). International Journal of Pediatric Otorhinolaryngology. 2010; 74(6):594-600. [DOI:10.1016/j.ijporl.2010.02.021] [PMID]
- Rocha-Muniz CN, Zachi EC, Teixeira RA, Ventura DF, Befi-Lopes DM, Schochat E. Association between language development and auditory processing disorders. Brazilian Journal of Otorhinolaryngology. 2014; 80(3):231-6. [DOI:10.1016/j.bjorl.2014.01.002] [PMID] [PMCID]
- Tillery KL. Central auditory processing evaluation: A test battery approach. In: Katz J, Medwetsky L, Robert B, Hood LJ, editors. Handbook of clinical audiology. Baltimore: Williams & Wilkins; 2009. [Link]
Type of Study: Research |
Subject:
Audiology
Received: 2023/02/17 | Accepted: 2023/06/14 | Published: 2022/02/6
Received: 2023/02/17 | Accepted: 2023/06/14 | Published: 2022/02/6
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.