

Volume 5, Issue 1 (Continuously Updated 2022)
Func Disabil J 2022, 5(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Riazi M, Moghadam F A, Sahebalzamani M, Riazi A, Sanei S H. A Comparative Study of Social Anxiety of Blind and Visually-impaired People With Sighted People. Func Disabil J 2022; 5 (1) : 59
URL: http://fdj.iums.ac.ir/article-1-191-en.html
URL: http://fdj.iums.ac.ir/article-1-191-en.html
Maryam Riazi1 

 , Farhad Adhami Moghadam2 , Mohammad Sahebalzamani3 , Abbas Riazi *4 , Seyed Hasan Sanei5
, Farhad Adhami Moghadam2 , Mohammad Sahebalzamani3 , Abbas Riazi *4 , Seyed Hasan Sanei5
, Farhad Adhami Moghadam2 , Mohammad Sahebalzamani3 , Abbas Riazi *4 , Seyed Hasan Sanei5
1- Department of Nursing, Faculty of Nursing and Midwifery, Islamic Azad University of Medical Sciences, Tehran, Iran.
2- Department of Ophthalmology, Faculty of Medicine, Islamic Azad University of Medical Sciences, Tehran, Iran.
3- Department of Health Services Management, School of Health and Biomedical Engineering, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran.
4- Department of Optometry, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,abbas.riazi@gmail.com
5- Department of Basic Rehabilitation Sciences, Faculty of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Ophthalmology, Faculty of Medicine, Islamic Azad University of Medical Sciences, Tehran, Iran.
3- Department of Health Services Management, School of Health and Biomedical Engineering, Tehran Medical Sciences, Islamic Azad University, Tehran, Iran.
4- Department of Optometry, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
5- Department of Basic Rehabilitation Sciences, Faculty of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1253 kb]
(905 Downloads)
| Abstract (HTML) (2250 Views)
Full-Text: (1108 Views)
Introduction
Social anxiety disorder (SAD) is the fourth most common psychiatric disorder [1]. Social anxiety, which is defined as an uncomfortable experience in the presence of others, is one of the phenomena that disrupt the process of social growth and development of people and hind
ers the flourishing of talents and proving the existence of people [2]. Researchers concluded that SAD is one of the most common psychiatric diagnoses worldwide, with lifetime prevalence rates ranging from 0.2 to 12.1 across countries [3]. An anxious person has special thoughts and thinks that everyone considers him negatively or thinks that he is rejected by everyone, and this causes discomfort and resentment for himself [4]. People who suffer from SAD have a fear. Severe during many social situations and avoidance of them are identified, the hallmark of SAD is impairment of social functioning [5]. People with SAD experience significant interpersonal impairment. However, little is known about the physiological processes associated with interpersonal dysfunction in this disorder. Determining the level of anxiety is a great help in medical and clinical services [6].
According to World Health Organization (WHO) in 2018, a total of 1.3 billion people worldwide have visual impairments. Of these, 36 million people are blind. South Asia is reported as the region with the highest percentage of blind people in the world, and the lowest amount is related to Australia. It is also predicted that by 2050, 61 million people will be blind, 474 million people will have moderate and severe visual impairment, and 360 million people will have a mild visual impairment [7, 8].
The causes of blindness and low vision are not the same in different countries [9-12]. Low vision is one of the most emotionally devastating physical problems. According to research, the fear of blindness accounts for 42% of cases of fear of disability [13]. It is well known that 90% of human social interactions are related to his vision, so a blind and partially sighted person is definitely having problems in all his social interactions. In the available sources, there have been studies on depression and anxiety disorders [14, 15]. Research has focused primarily on symptoms of depression and anxiety in visually impaired adults using screening questionnaires, showing that approximately one-third of visually impaired adults experience significant clinical symptoms [16]. Agoraphobia and social phobia are the most common anxiety disorders in visually impaired adults. The conclusion of this study shows that depression and anxiety are major public health problems [17].
Depression is more severe in people with significant vision loss. The negative impact of vision loss on quality of life, social interaction, and psychological functioning has been well established [8, 18]. The higher prevalence of depression in visually impaired individuals compared to the general population suggests that this condition in itself increases the risk of depression [19]. Research conducted in Korea among people with anophthalmia (no eye) showed that anxiety disorders occur in about 30% of people, while in Japan such disorders occur in approximately 26% of people with high myopia [16]. In a study conducted in Iran, it was found that the level of anxiety and stress in blind students is significantly higher than normal students [15].
In 2012, Razavi et al. investigated the relationship between personality traits and coping styles with social anxiety in blind and normal students of Fars province universities in the academic year 2006. The obtained results indicated that there is a significant relationship between personality traits and social anxiety in blind students, and there is also a significant relationship between personality traits and social anxiety in normal students [20]. In one study, it was found that deaf students have higher mental health than blind students and the difference in anxiety and depression variables is significant [21].
Unfortunately, no study has been conducted in the field of social anxiety of blind and visually impaired people in Iran. By conducting this research, we can understand the level of this anxiety in Iranian blind and partially sighted people. Although various tools have been developed to measure social anxiety, many of them have neglected to measure the different dimensions of this disorder. Some have compiled the scale of social anxiety and avoidance and some have made the issue of fear a criterion.
Various tools have been developed to measure social anxiety, among which Leibovitz’s social anxiety scale is the only tool that is based on social situations, while other questionnaires in this field have only emphasized symptoms. The studies conducted show that the research gap in this field is quite obvious and it reveals the importance of this research; therefore, by conducting this study, the possible difference between the level of social anxiety in blind people and normal people will be obtained.
Materials and Methods
The current research is causal-comparative research in terms of its nature and goals [22]. This study was conducted at the Low Vision Research Center of the School of Rehabilitation Sciences of Iran University of Medical Sciences. In this study, a comparison of averages is desired. The sample size was calculated with a confidence level of 95% and a test power of 80% using the calculation formula, the number of 240 people (120 patients and 120 sighted people). The criteria for entering the study are having blindness and low vision, the age range between 40-20 years, the criterion for diagnosing blindness is the lack of light perception and vision less than 20/200 (Snellen chart), which was determined by an ophthalmologist or an optometrist. Sighted people do not suffer from blindness and low vision. They should have normal vision. The method of data collection is the questionnaire method and the use of Labiotz’s social anxiety questionnaire. Various tools have been developed to measure social anxiety, among which Leibovitz’s social anxiety scale is the only tool that is based on social situations, while other tools in this field have only emphasized the symptoms [23, 24]. Fortunately, the validity, reliability, and general structure of the Persian version of Leibowitz’s social anxiety scale have been investigated [25]. The prevalence of this anxiety has been reported differently in different societies. In a limited study conducted in Iran, the prevalence rate was reported around 10%, and in another study, it was reported at 28.6% [26].
Participants are asked to answer the questions of the data collection tool. Normal subjects are also randomly selected from the normal population who are similar to the patient group in terms of age and sex. The overall score of this questionnaire is between 23 and 92 [26]. Leibowitz’s questionnaire includes situations that we face in our daily life. This tool has two subscales including anxiety, avoidance, or escape subscale. In each situation, each question is answered numerically and based on the following criteria: Subscale 1: the person expresses his opinion as 1- a little - 2 to some extent 3 and strongly 4. Subscale 2: the person expresses his opinion as never 1, sometimes 2, often 3, and always 4. The data were analyzed by SPSS software, versian 18. The average score of the Leibowitz questionnaire was compared between the two groups of blind patients and the normal group, and P>0.05 was considered statistically significant.
Results
A total of 240 people aged between 20 and 40 participated in this study, of which 120 were normal people and the rest had degrees of blindness and low vision (132 women and 108 men). The average age of the participants was 31.38±6.87. Table 1 shows the number of participants according to their vision.
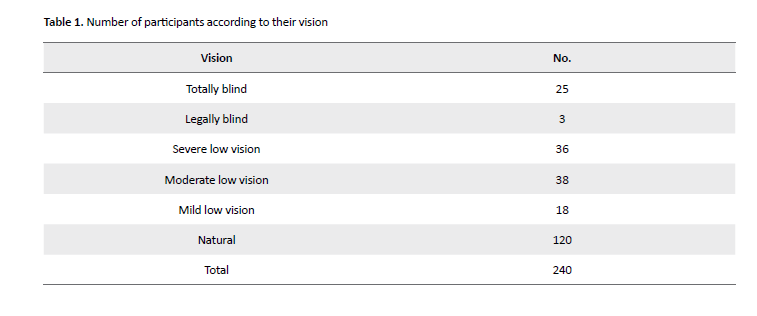
The average score of social anxiety in the blind group is 43.27±14.27 and 44.25±12.32 in the sighted group. The average scores of avoidance in the blind group are (39.83±14.35) and (41.66±12.07) in the sighted group. The of scores obtained in the anxiety section compared to the avoidance or escape are almost equal with no significant difference (P=0.157). In other words, the amount of anxiety and the amount of avoidance is the same in all participants and there is no significant difference between the two, therefore, each amount and each degree of social anxiety is associated with the same amount and amount of avoidance. The amount of social anxiety has a significant difference between the groups (P=0.009), and the amount of avoidance also has a statistically significant difference between the groups (P=0.016) (Table 2).
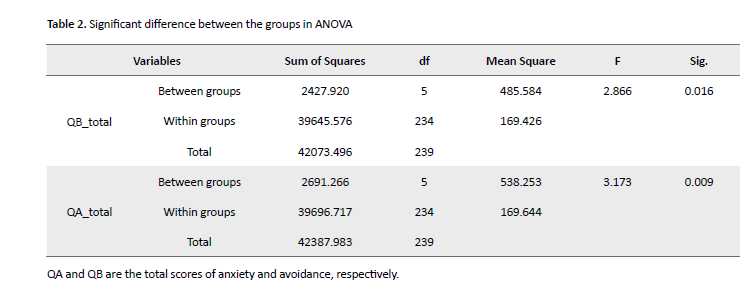
According to Table 2, the level of anxiety in totally blind people is almost significant compared to sighted people (P=0.053). In addition, there is a significant difference in comparing totally blind people with mildly impaired people (P=0.027). Therefore, people with normal vision or mild vision loss experience higher levels of anxiety than totally blind people, and instead, totally blind people have less social anxiety.
People with normal vision or mild vision loss experience higher levels of anxiety than totally blind people, and instead totally blind people have less social anxiety (Figure 1).
.png)
Figure 1. Comparing the level of social anxiety in different groups
People with normal vision or mild vision loss experience higher levels of avoidance than totally blind people, and instead, totally blind people have less avoidance (Figure 2).
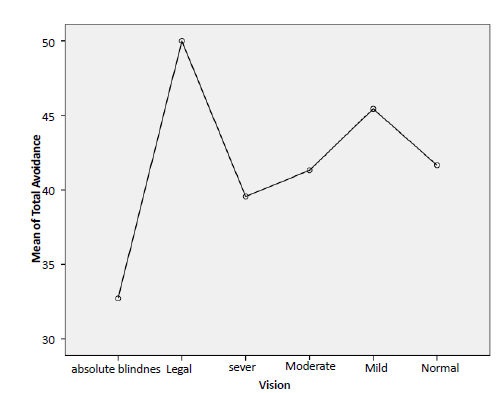
Figure 2. Comparing the level of avoidance in different groups
According to statistical analysis, there is a significant difference in the scores of avoidance between the totally blind and sighted people (P=0.024), and there is a statistical difference between the totally blind and mildly visually impaired people (P=0.022). Therefore, people with normal vision and mild low vision suffer from greater degrees of avoidance, and instead, people with total blindness experience less avoidance.
Interestingly, the amount of social anxiety changes with a slight slope in different groups, in other words, the amount of social anxiety increases with the increase in vision (Figure 3).
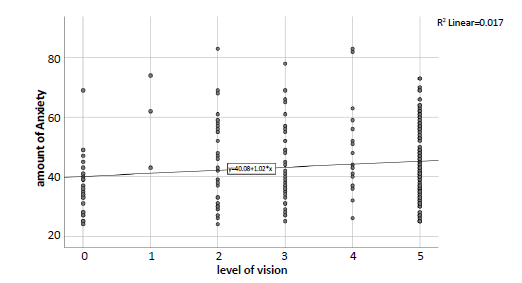
Figure 3. Social anxiety increases in different groups as vision becomes better
It can be seen that the amount of avoidance or escape changes with a gentle slope in different groups, in other words, with the increase in vision, the amount of avoidance or escape increases (Figure 4).
.png)
Figure 4. Avoidance increases in different groups as vision becomes better
4. Discussion
The purpose of this study was to investigate the level of social anxiety in blind and partially sighted people compared to sighted people. The average anxiety score in the blind group was a little lower than in the sighted group. The results indicate that the average scores of avoidance in the blind group were also a little lower than in the sighted group. It can be seen that both the amount of social anxiety and the amount of avoidance are lower in the blind and visually impaired group (Table 1). It is well known that there is some degree of anxiety especially social anxiety in all people of different ages. Stein et al. in 2017 conducted a study at the global level on the prevalence and severity of SAD-related disorders. While differences in the prevalence of SAD were evident across countries, several consistent patterns were found worldwide including early age of onset, persistence, impairment in multiple domains, as well as social relationships and associated psychological characteristics. Researchers concluded that SAD is one of the most common psychiatric diagnoses worldwide, with lifetime prevalence rates ranging from 0.2 to 12.1 across countries [3]. The results of our study are consistent with the results of the above study, and there are some degrees of the prevalence of social anxiety both in the blind and partially sighted community and in the sighted people.
The lowest level of anxiety is related to the totally blind participants, with a score of 36.08, which is less than some sighted participants (44.25). Regarding avoidance, this rule is valid in that the avoidance rate of people with total blindness (32.72) is lower than that of sighted people (44.66). In 2015, Wender et al. examined anxiety disorders (panic disorder, agoraphobia, social phobia, and generalized anxiety disorder) in visually impaired adults and compared these estimates with sighted peers. The results showed that the prevalence of major depressive disorder (4.5%) and anxiety disorders (7.5%), as well as the prevalence of subthreshold depression (32.2%) and subthreshold anxiety (15.6%) in the elderly with poor vision compared to people with normal vision, was significantly higher than peers (P<0.05). Agoraphobia and social phobia were the most common anxiety disorders in visually impaired adults. The conclusion of this study shows that depression and anxiety are the main health problems [17]. It should be noted that the results of the above study are different from the results of the present study. Although in another study, no significant difference was found between the anxiety of blind and sighted people, in the current study the prevalence of anxiety in blind people is lower than that of sighted people. In 2016, Ashuri et al. compared the level of depression, anxiety, and stress in blind people and normal people. The first group was blind students who were selected by sampling method; while the second group was regular students who were selected by a simple random method. The instrument used in this research was the Leviband depression, anxiety, and stress scale. The findings showed that the level of anxiety and stress in blind students was significantly higher than normal students. However, there was no significant difference in the level of depression of both groups [15]. It should be noted that the above study did not measure social anxiety, while the present study measured this factor. Therefore, this difference is not comparable.
There is a significant difference in the amount of social anxiety between blind and visually impaired groups compared to sighted people (P=0.009). Also, the amount of avoidance is statistically significant between these two groups (P=0.016). In 2013, Razavi et al. investigated the relationship between personality traits and coping styles with social anxiety in blind and normal students of Fars province universities in the academic year 2006. There is a difference in social anxiety between blind and normal students considering the inverse relationship between extroversion and cordiality indicators with low social anxiety, the development of a sense of positivity, confidence, and understanding in blind people can reduce their social anxiety [20]. In 2016, Ata Dokht et al. conducted a study on the level of anxiety and stress among blind and deaf people among 50 blind and 50 deaf people. The results of this research showed that the mean scores of psychological disorders of depression, anxiety, and stress in blind students are higher than in deaf students. In other words, deaf students have higher mental health than blind students [21]. Although there is a difference in terms of the type of study and the statistical population, the above results are different from the results of the present study. A general result is that anxiety is more in the blind, while it is less in our study. In 2015, Farshbaf et al. compared social anxiety between deaf and blind teenagers and normal ones in Tehran. From the total number of students, 150 people were selected as the available sampling method. The SPIN questionnaire was used to measure social phobia. The results showed that social anxiety in blind and deaf people is significantly higher than normal people. Nevertheless, no difference was observed between blind and deaf people in social anxiety. Sight and hearing are basic senses in communicating with others. Since blind people are deprived of sight and deaf people are deprived of hearing, the following situations can lead to experiencing anxiety: Conversation, observing social events, fear of confrontation, poor performance in front of others, being in a crowd, and inability to observe other people’s feedback towards their behavior [27]. This finding is differing from the findings of our study.
The results show that the level of anxiety in totally blind people is almost significant (P=0.053). Another important point is that the above-mentioned difference between totally blind and mildly impaired people is also seen. There is also a significant difference between totally blind and mildly impaired people (P=0.027). Therefore, people with normal vision or mildly impaired vision experience more anxiety than totally blind people, and totally blind people experience less anxiety. The numerous studies that have been conducted in the field of social anxiety in the blind, all talk about the higher level of anxiety in the blind and partially sighted groups. Of course, these studies have only examined anxiety and social anxiety is a controversial issue. The above finding is not consistent with the results of other studies, which is obviously due to the different conditions of the study; for example, in a study conducted by Wender on the elderly, he reported more anxiety in the visually impaired, but not social anxiety [8]. Other studies in the field of anxiety have shown that anxiety is more in blind and partially sighted people than in sighted people, but none of them have addressed the issue of social anxiety [15, 17, 20, 28]. Social anxiety has been investigated in limited studies; for example, social anxiety between blind and sighted students showed that social anxiety is more prevalent in blind students [20]. This study was conducted on 35 people and only students, and another questionnaire was used. Social anxiety has been reported in primary school students more than sighted people [29]. It has been shown in only one study that blind people who had more self-efficacy beliefs had lower levels of social anxiety, and this result can be consistent with the present study [21].
The amount of avoidance between the totally blind and sighted people has a significant difference, and there is a statistical difference between the totally blind and mildly impaired people. Therefore, people with normal vision and mild low vision suffer from greater degrees of avoidance, and instead, people with total blindness experience less avoidance. Unfortunately, there are not many studies in the field of social avoidance to be compared with the results of the present study.
The amount of social anxiety and avoidance changes with a mild slope in different groups. In other words, with the increase in vision, the amount of social anxiety and avoidance increases. Although this slope is quite gentle and changes with very little numerical value, it shows a continuous difference. The changes indicate that lower vision is associated with less social anxiety and avoidance. The findings show that the amount of vision can be inversely related to the amount of social anxiety and avoidance. Here the amount of vision of a totally blind person who is unable to perceive even light is considered as compared to a person with normal vision. The results show this relationship with a very gentle slope; as the condition of vision improves and moves towards sighted people, the amount of social anxiety and avoidance increases.
Why a blind person has less social anxiety can have several reasons. One of these reasons may be the information inputs designed for humans occur through the eyes, ears, touching, smelling, and other senses that a person uses to access information from the surrounding environment. Therefore, because there is no vision, it is possible that in this field, when this information is analyzed, emotional reactions and the effects of social anxiety and avoidance are less. For example, when we are in front of a person, by looking at the person’s face and facial expressions, we can understand that the person feels relaxed or may feel bad about our words. The face may be confused. He may smile and these reactions make us give different reactions. It may sometimes cause social anxiety for us or force us to avoid or run away from these conditions. Therefore, in the case of a person who is blind, these conditions may not be experienced because he cannot see the facial expressions of a person. Therefore, not receiving visual inputs can be one of the reasons why social anxiety is probably lower in blind and partially sighted people than in sighted people. This issue is also true for people with mild visual impairment with similar results. This means that a person with mild visual impairment experiences greater degrees of social anxiety and avoidance than a person with complete blindness. A person with mild visual impairment has many visual inputs and can act like a sighted person; therefore, the level of social anxiety and avoidance in this group of people is the same as that of sighted people.
5. Conclusion
People with normal vision or mild vision loss experience higher levels of social anxiety than totally blind people, and instead, totally blind people have less social anxiety. Also, people with normal vision and mild vision loss report higher levels of avoidance. Conversely, people with total blindness experience lower levels of avoidance.
Ethical Considerations
Compliance with ethical guidelines
Letter of introduction and obtaining permission to conduct research from the Research Vice-Chancellor of the Faculty of Nursing, Islamic Azad University, Tehran Medical Sciences, with Ethical ID number IR. IAU.TMU.REC.1401.140 was obtained.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision : Maryam Riazi; Methodology: Maryam Riazi and Abbas Riazi; Writing, reviewing and editing: All authors; Statistic analysis: Sayed Hassan Sanei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are thankful to all the participants in this study. We are grateful to the management of the Visual Impairment Research Center of School of Rehabilitation Sciences of Iran University of Medical Sciences. We sincerely thank the RP community.
References
Social anxiety disorder (SAD) is the fourth most common psychiatric disorder [1]. Social anxiety, which is defined as an uncomfortable experience in the presence of others, is one of the phenomena that disrupt the process of social growth and development of people and hind
ers the flourishing of talents and proving the existence of people [2]. Researchers concluded that SAD is one of the most common psychiatric diagnoses worldwide, with lifetime prevalence rates ranging from 0.2 to 12.1 across countries [3]. An anxious person has special thoughts and thinks that everyone considers him negatively or thinks that he is rejected by everyone, and this causes discomfort and resentment for himself [4]. People who suffer from SAD have a fear. Severe during many social situations and avoidance of them are identified, the hallmark of SAD is impairment of social functioning [5]. People with SAD experience significant interpersonal impairment. However, little is known about the physiological processes associated with interpersonal dysfunction in this disorder. Determining the level of anxiety is a great help in medical and clinical services [6].
According to World Health Organization (WHO) in 2018, a total of 1.3 billion people worldwide have visual impairments. Of these, 36 million people are blind. South Asia is reported as the region with the highest percentage of blind people in the world, and the lowest amount is related to Australia. It is also predicted that by 2050, 61 million people will be blind, 474 million people will have moderate and severe visual impairment, and 360 million people will have a mild visual impairment [7, 8].
The causes of blindness and low vision are not the same in different countries [9-12]. Low vision is one of the most emotionally devastating physical problems. According to research, the fear of blindness accounts for 42% of cases of fear of disability [13]. It is well known that 90% of human social interactions are related to his vision, so a blind and partially sighted person is definitely having problems in all his social interactions. In the available sources, there have been studies on depression and anxiety disorders [14, 15]. Research has focused primarily on symptoms of depression and anxiety in visually impaired adults using screening questionnaires, showing that approximately one-third of visually impaired adults experience significant clinical symptoms [16]. Agoraphobia and social phobia are the most common anxiety disorders in visually impaired adults. The conclusion of this study shows that depression and anxiety are major public health problems [17].
Depression is more severe in people with significant vision loss. The negative impact of vision loss on quality of life, social interaction, and psychological functioning has been well established [8, 18]. The higher prevalence of depression in visually impaired individuals compared to the general population suggests that this condition in itself increases the risk of depression [19]. Research conducted in Korea among people with anophthalmia (no eye) showed that anxiety disorders occur in about 30% of people, while in Japan such disorders occur in approximately 26% of people with high myopia [16]. In a study conducted in Iran, it was found that the level of anxiety and stress in blind students is significantly higher than normal students [15].
In 2012, Razavi et al. investigated the relationship between personality traits and coping styles with social anxiety in blind and normal students of Fars province universities in the academic year 2006. The obtained results indicated that there is a significant relationship between personality traits and social anxiety in blind students, and there is also a significant relationship between personality traits and social anxiety in normal students [20]. In one study, it was found that deaf students have higher mental health than blind students and the difference in anxiety and depression variables is significant [21].
Unfortunately, no study has been conducted in the field of social anxiety of blind and visually impaired people in Iran. By conducting this research, we can understand the level of this anxiety in Iranian blind and partially sighted people. Although various tools have been developed to measure social anxiety, many of them have neglected to measure the different dimensions of this disorder. Some have compiled the scale of social anxiety and avoidance and some have made the issue of fear a criterion.
Various tools have been developed to measure social anxiety, among which Leibovitz’s social anxiety scale is the only tool that is based on social situations, while other questionnaires in this field have only emphasized symptoms. The studies conducted show that the research gap in this field is quite obvious and it reveals the importance of this research; therefore, by conducting this study, the possible difference between the level of social anxiety in blind people and normal people will be obtained.
Materials and Methods
The current research is causal-comparative research in terms of its nature and goals [22]. This study was conducted at the Low Vision Research Center of the School of Rehabilitation Sciences of Iran University of Medical Sciences. In this study, a comparison of averages is desired. The sample size was calculated with a confidence level of 95% and a test power of 80% using the calculation formula, the number of 240 people (120 patients and 120 sighted people). The criteria for entering the study are having blindness and low vision, the age range between 40-20 years, the criterion for diagnosing blindness is the lack of light perception and vision less than 20/200 (Snellen chart), which was determined by an ophthalmologist or an optometrist. Sighted people do not suffer from blindness and low vision. They should have normal vision. The method of data collection is the questionnaire method and the use of Labiotz’s social anxiety questionnaire. Various tools have been developed to measure social anxiety, among which Leibovitz’s social anxiety scale is the only tool that is based on social situations, while other tools in this field have only emphasized the symptoms [23, 24]. Fortunately, the validity, reliability, and general structure of the Persian version of Leibowitz’s social anxiety scale have been investigated [25]. The prevalence of this anxiety has been reported differently in different societies. In a limited study conducted in Iran, the prevalence rate was reported around 10%, and in another study, it was reported at 28.6% [26].
Participants are asked to answer the questions of the data collection tool. Normal subjects are also randomly selected from the normal population who are similar to the patient group in terms of age and sex. The overall score of this questionnaire is between 23 and 92 [26]. Leibowitz’s questionnaire includes situations that we face in our daily life. This tool has two subscales including anxiety, avoidance, or escape subscale. In each situation, each question is answered numerically and based on the following criteria: Subscale 1: the person expresses his opinion as 1- a little - 2 to some extent 3 and strongly 4. Subscale 2: the person expresses his opinion as never 1, sometimes 2, often 3, and always 4. The data were analyzed by SPSS software, versian 18. The average score of the Leibowitz questionnaire was compared between the two groups of blind patients and the normal group, and P>0.05 was considered statistically significant.
Results
A total of 240 people aged between 20 and 40 participated in this study, of which 120 were normal people and the rest had degrees of blindness and low vision (132 women and 108 men). The average age of the participants was 31.38±6.87. Table 1 shows the number of participants according to their vision.
The average score of social anxiety in the blind group is 43.27±14.27 and 44.25±12.32 in the sighted group. The average scores of avoidance in the blind group are (39.83±14.35) and (41.66±12.07) in the sighted group. The of scores obtained in the anxiety section compared to the avoidance or escape are almost equal with no significant difference (P=0.157). In other words, the amount of anxiety and the amount of avoidance is the same in all participants and there is no significant difference between the two, therefore, each amount and each degree of social anxiety is associated with the same amount and amount of avoidance. The amount of social anxiety has a significant difference between the groups (P=0.009), and the amount of avoidance also has a statistically significant difference between the groups (P=0.016) (Table 2).
According to Table 2, the level of anxiety in totally blind people is almost significant compared to sighted people (P=0.053). In addition, there is a significant difference in comparing totally blind people with mildly impaired people (P=0.027). Therefore, people with normal vision or mild vision loss experience higher levels of anxiety than totally blind people, and instead, totally blind people have less social anxiety.
People with normal vision or mild vision loss experience higher levels of anxiety than totally blind people, and instead totally blind people have less social anxiety (Figure 1).
Figure 1. Comparing the level of social anxiety in different groups
People with normal vision or mild vision loss experience higher levels of avoidance than totally blind people, and instead, totally blind people have less avoidance (Figure 2).
Figure 2. Comparing the level of avoidance in different groups
According to statistical analysis, there is a significant difference in the scores of avoidance between the totally blind and sighted people (P=0.024), and there is a statistical difference between the totally blind and mildly visually impaired people (P=0.022). Therefore, people with normal vision and mild low vision suffer from greater degrees of avoidance, and instead, people with total blindness experience less avoidance.
Interestingly, the amount of social anxiety changes with a slight slope in different groups, in other words, the amount of social anxiety increases with the increase in vision (Figure 3).
Figure 3. Social anxiety increases in different groups as vision becomes better
It can be seen that the amount of avoidance or escape changes with a gentle slope in different groups, in other words, with the increase in vision, the amount of avoidance or escape increases (Figure 4).
Figure 4. Avoidance increases in different groups as vision becomes better
4. Discussion
The purpose of this study was to investigate the level of social anxiety in blind and partially sighted people compared to sighted people. The average anxiety score in the blind group was a little lower than in the sighted group. The results indicate that the average scores of avoidance in the blind group were also a little lower than in the sighted group. It can be seen that both the amount of social anxiety and the amount of avoidance are lower in the blind and visually impaired group (Table 1). It is well known that there is some degree of anxiety especially social anxiety in all people of different ages. Stein et al. in 2017 conducted a study at the global level on the prevalence and severity of SAD-related disorders. While differences in the prevalence of SAD were evident across countries, several consistent patterns were found worldwide including early age of onset, persistence, impairment in multiple domains, as well as social relationships and associated psychological characteristics. Researchers concluded that SAD is one of the most common psychiatric diagnoses worldwide, with lifetime prevalence rates ranging from 0.2 to 12.1 across countries [3]. The results of our study are consistent with the results of the above study, and there are some degrees of the prevalence of social anxiety both in the blind and partially sighted community and in the sighted people.
The lowest level of anxiety is related to the totally blind participants, with a score of 36.08, which is less than some sighted participants (44.25). Regarding avoidance, this rule is valid in that the avoidance rate of people with total blindness (32.72) is lower than that of sighted people (44.66). In 2015, Wender et al. examined anxiety disorders (panic disorder, agoraphobia, social phobia, and generalized anxiety disorder) in visually impaired adults and compared these estimates with sighted peers. The results showed that the prevalence of major depressive disorder (4.5%) and anxiety disorders (7.5%), as well as the prevalence of subthreshold depression (32.2%) and subthreshold anxiety (15.6%) in the elderly with poor vision compared to people with normal vision, was significantly higher than peers (P<0.05). Agoraphobia and social phobia were the most common anxiety disorders in visually impaired adults. The conclusion of this study shows that depression and anxiety are the main health problems [17]. It should be noted that the results of the above study are different from the results of the present study. Although in another study, no significant difference was found between the anxiety of blind and sighted people, in the current study the prevalence of anxiety in blind people is lower than that of sighted people. In 2016, Ashuri et al. compared the level of depression, anxiety, and stress in blind people and normal people. The first group was blind students who were selected by sampling method; while the second group was regular students who were selected by a simple random method. The instrument used in this research was the Leviband depression, anxiety, and stress scale. The findings showed that the level of anxiety and stress in blind students was significantly higher than normal students. However, there was no significant difference in the level of depression of both groups [15]. It should be noted that the above study did not measure social anxiety, while the present study measured this factor. Therefore, this difference is not comparable.
There is a significant difference in the amount of social anxiety between blind and visually impaired groups compared to sighted people (P=0.009). Also, the amount of avoidance is statistically significant between these two groups (P=0.016). In 2013, Razavi et al. investigated the relationship between personality traits and coping styles with social anxiety in blind and normal students of Fars province universities in the academic year 2006. There is a difference in social anxiety between blind and normal students considering the inverse relationship between extroversion and cordiality indicators with low social anxiety, the development of a sense of positivity, confidence, and understanding in blind people can reduce their social anxiety [20]. In 2016, Ata Dokht et al. conducted a study on the level of anxiety and stress among blind and deaf people among 50 blind and 50 deaf people. The results of this research showed that the mean scores of psychological disorders of depression, anxiety, and stress in blind students are higher than in deaf students. In other words, deaf students have higher mental health than blind students [21]. Although there is a difference in terms of the type of study and the statistical population, the above results are different from the results of the present study. A general result is that anxiety is more in the blind, while it is less in our study. In 2015, Farshbaf et al. compared social anxiety between deaf and blind teenagers and normal ones in Tehran. From the total number of students, 150 people were selected as the available sampling method. The SPIN questionnaire was used to measure social phobia. The results showed that social anxiety in blind and deaf people is significantly higher than normal people. Nevertheless, no difference was observed between blind and deaf people in social anxiety. Sight and hearing are basic senses in communicating with others. Since blind people are deprived of sight and deaf people are deprived of hearing, the following situations can lead to experiencing anxiety: Conversation, observing social events, fear of confrontation, poor performance in front of others, being in a crowd, and inability to observe other people’s feedback towards their behavior [27]. This finding is differing from the findings of our study.
The results show that the level of anxiety in totally blind people is almost significant (P=0.053). Another important point is that the above-mentioned difference between totally blind and mildly impaired people is also seen. There is also a significant difference between totally blind and mildly impaired people (P=0.027). Therefore, people with normal vision or mildly impaired vision experience more anxiety than totally blind people, and totally blind people experience less anxiety. The numerous studies that have been conducted in the field of social anxiety in the blind, all talk about the higher level of anxiety in the blind and partially sighted groups. Of course, these studies have only examined anxiety and social anxiety is a controversial issue. The above finding is not consistent with the results of other studies, which is obviously due to the different conditions of the study; for example, in a study conducted by Wender on the elderly, he reported more anxiety in the visually impaired, but not social anxiety [8]. Other studies in the field of anxiety have shown that anxiety is more in blind and partially sighted people than in sighted people, but none of them have addressed the issue of social anxiety [15, 17, 20, 28]. Social anxiety has been investigated in limited studies; for example, social anxiety between blind and sighted students showed that social anxiety is more prevalent in blind students [20]. This study was conducted on 35 people and only students, and another questionnaire was used. Social anxiety has been reported in primary school students more than sighted people [29]. It has been shown in only one study that blind people who had more self-efficacy beliefs had lower levels of social anxiety, and this result can be consistent with the present study [21].
The amount of avoidance between the totally blind and sighted people has a significant difference, and there is a statistical difference between the totally blind and mildly impaired people. Therefore, people with normal vision and mild low vision suffer from greater degrees of avoidance, and instead, people with total blindness experience less avoidance. Unfortunately, there are not many studies in the field of social avoidance to be compared with the results of the present study.
The amount of social anxiety and avoidance changes with a mild slope in different groups. In other words, with the increase in vision, the amount of social anxiety and avoidance increases. Although this slope is quite gentle and changes with very little numerical value, it shows a continuous difference. The changes indicate that lower vision is associated with less social anxiety and avoidance. The findings show that the amount of vision can be inversely related to the amount of social anxiety and avoidance. Here the amount of vision of a totally blind person who is unable to perceive even light is considered as compared to a person with normal vision. The results show this relationship with a very gentle slope; as the condition of vision improves and moves towards sighted people, the amount of social anxiety and avoidance increases.
Why a blind person has less social anxiety can have several reasons. One of these reasons may be the information inputs designed for humans occur through the eyes, ears, touching, smelling, and other senses that a person uses to access information from the surrounding environment. Therefore, because there is no vision, it is possible that in this field, when this information is analyzed, emotional reactions and the effects of social anxiety and avoidance are less. For example, when we are in front of a person, by looking at the person’s face and facial expressions, we can understand that the person feels relaxed or may feel bad about our words. The face may be confused. He may smile and these reactions make us give different reactions. It may sometimes cause social anxiety for us or force us to avoid or run away from these conditions. Therefore, in the case of a person who is blind, these conditions may not be experienced because he cannot see the facial expressions of a person. Therefore, not receiving visual inputs can be one of the reasons why social anxiety is probably lower in blind and partially sighted people than in sighted people. This issue is also true for people with mild visual impairment with similar results. This means that a person with mild visual impairment experiences greater degrees of social anxiety and avoidance than a person with complete blindness. A person with mild visual impairment has many visual inputs and can act like a sighted person; therefore, the level of social anxiety and avoidance in this group of people is the same as that of sighted people.
5. Conclusion
People with normal vision or mild vision loss experience higher levels of social anxiety than totally blind people, and instead, totally blind people have less social anxiety. Also, people with normal vision and mild vision loss report higher levels of avoidance. Conversely, people with total blindness experience lower levels of avoidance.
Ethical Considerations
Compliance with ethical guidelines
Letter of introduction and obtaining permission to conduct research from the Research Vice-Chancellor of the Faculty of Nursing, Islamic Azad University, Tehran Medical Sciences, with Ethical ID number IR. IAU.TMU.REC.1401.140 was obtained.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and supervision : Maryam Riazi; Methodology: Maryam Riazi and Abbas Riazi; Writing, reviewing and editing: All authors; Statistic analysis: Sayed Hassan Sanei.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are thankful to all the participants in this study. We are grateful to the management of the Visual Impairment Research Center of School of Rehabilitation Sciences of Iran University of Medical Sciences. We sincerely thank the RP community.
References
- von Glischinski M, Willutzki U, Stangier U, Hiller W, Hoyer J, Leibing E, et al. Liebowitz social anxiety scale (lsas): optimal cut points for remission and response in a german sample. Clin psychology Psychother. 2018; 25(3):465-73. [DOI:10.1002/cpp.2179] [PMID]
- Yousefi Kalekhane, Z., Hashemi Nosratabad, T., Mahmoud Alilu, M. The role of brain-behavioral systems and stressful experiences in symptoms of social. Thought Behav Clin Psychol. 2017; 12(44):77-86. [Link]
- Stein DJ, Lim CCW, Roest AM, de Jonge P, Aguilar-Gaxiola S, Al-Hamzawi A, et al. The cross-national epidemiology of social anxiety disorder: Data from the World Mental Health Survey Initiative. BMC Med. 2017; 15(1):143. [DOI:10.1186/s12916-017-0889-2] [PMID] [PMCID]
- Sorrell JM. Diagnostic and Statistical Manual of Mental Disorders-5: Implications for older adults and their families. J Psychosoc Nurs Ment Health Serv. 2013; 51(3):19-22. [DOI:10.3928/02793695-20130207-01]
- Morrison AS, Mateen MA, Brozovich FA, Zaki J, Goldin PR, Heimberg RG, et al. Empathy for positive and negative emotions in social anxiety disorder. Behav Res Ther. 2016; 87:232-42. [DOI:10.1016/j.brat.2016.10.005] [PMID] [PMCID]
- Hoffman SG, Otto M. Cognitive behavioral therapy for social anxiety disorder: Evidence-based and disorder-specific treatment techniques. [M. Khanzadeh, S. Soltani, M. Saidian Persian trans]. Tehran: Avai Noor Publications; 2008. [Link]
- Bourne R, Steinmetz JD, Flaxman S, Briant PS, Taylor HR, Resnikoff S, et al. Trends in prevalence of blindness and distance and near vision impairment over 30 years: An analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021; 9(2):e130-43. [DOI:10.1016/S2214-109X(20)30425-3] [PMID] [PMCID] [Link]
- Horowitz A. The prevalence and consequences of vision impairment in later life. Top Geriatr Rehabil. 2004; 20(3):185-95. [DOI:10.1097/00013614-200407000-00006]
- World Health Organisation (WHO). Blindness and vision impairment. Geneva: World Health Organisation; 2022. [Link]
- World Health Organisation (WHO). Magnitude and causes of visual impairment. World Health Organization, [Link]
- Brilliant RL. Essentials of low vision practice. Boston: Butterworth Heinemann Publication; 1999. [Link]
- Bourne RRA, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB. Vision Loss Expert Group. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis Lancet Glob Health. 2017; 5(9):e888-97. [PMID] [DOI:10.1016/S2214-109X(17)30293-0]
- Hahm BJ, Shin YW, Shim EJ, Jeon HJ, Seo JM, Chung H, et al. Depression and the vision-related quality of life in patients with retinitis pigmentosa. Br J Ophthalmol 2008; 92(5):650-4. [DOI:10.1136/bjo.2007.127092] [PMID]
- van der Aa HP, Krijnen-de Bruin E, van Rens GH, Twisk JW, van Nispen RM. Watchful waiting for subthreshold depression and anxiety in visually impaired older adults. Qual Life Res. 2015; 24(12):2885-93. [DOI:10.1007/s11136-015-1032-5] [PMID] [PMCID]
- Ashuri A, Shojaei S, Fatahian, F. [A comparative study of depression, anxiety and stress in blind and normal people (Persian)]. J Empowering Except Child. 2016; 8(4):71-80. [DOI:10.22034/CECIRANJ.2017.70925]
- Binder KW, Wrzesińska MA, Kocur J. Anxiety in persons with visual impairment. Psychiatria Polska. 2020; 54(2):279-88. [DOI:10.12740/PP/OnlineFirst/85408] [PMID]
- van der Aa HP, Comijs HC, Penninx BW, van Rens GH, van Nispen RM. Major depressive and anxiety disorders in visually impaired older adults. Invest Ophthalmol Vis Sci. 2015; 56(2):849-54. [DOI:10.1167/iovs.14-15848] [PMID]
- Stelmack JA, Tang XC, Wei Y, Massof RW. The effectiveness of low-vision rehabilitation in 2 cohorts derived from the veterans affairs Low-Vision Intervention Trial. Arch Ophthalmol. 2012; 130(9):1162-8. [DOI:10.1001/archophthalmol.2012.1820] [PMID]
- Bruijning JE, van Rens G, Fick M, Knol DL, van Nispen R. Longitudinal observation, evaluation and interpretation of coping with mental (emotional) health in low vision rehabilitation using the Dutch ICF Activity Inventory. Health Qual Life Outcomes. 2014; 12:182. [DOI:10.1186/s12955-014-0182-4] [PMID] [PMCID]
- Razavi A, Kazemi S. [Relationship between personality traits, coping style and social anxiety among blind and normal sighted students in universities of Fars province (Persian)]. Psychol Except Individ. 2012; 1(4):109-34. [Link]
- Atadokht A, Jafari I, Hayati M, Kamarzarin H, Mehri S. [The Role of body image and self-concept in predicting psychological disorders among blind and deaf students (Persian)]. J Except Child. 2017; 17(2):13-24. [Link]
- Hijazi S. Familiarity with research in medical and health sciences. Tehran: Heydari. 2014. [Link]
- Baker SL, Heinrichs N, Kim HJ, Hofmann SG. The liebowitz social anxiety scale as a self-report instrument: A preliminary psychometric analysis. Behav Res Ther. 2002; 40(6):701-15. [DOI:10.1016/S0005-7967(01)00060-2] [PMID]
- Heimberg RG, Horner KJ, Juster HR, Safren SA, Brown EJ, Schneier FR, et al. Psychometric properties of the Liebowitz Social Anxiety Scale. Psychol Med. 1999; 29(1):199-212. [DOI:10.1017/S0033291798007879] [PMID]
- Hasani J ; Fayazi M, Akbari E. [Reliability, Validity, and Confirmatory Factor Structure of Persian Version of Liebowitz Social Anxiety Scale (LSAS) (Persian)]. Soc Psychol Res. 2016; 6(24):35-52. [Link]
- Momeni M. [Prevalence rate and factors related to social phobia in nursing and midwifery students (Persian)]. Health Care Mag. 2014; 17(2):137-45. [Link]
- Farshbaf T. [Comparison of social phobia in deaf, blind and normal teenagers in Tehran (Persian)] [MA thesis]. Islamic Azad University, Shahrood Branch; 2015.
- Evans JR, Fletcher AE, Wormald RP. Depression and anxiety in visually impaired older people. Ophthalmol. 2007;114(2):283-8. [DOI:10.1016/j.ophtha.2006.10.006] [PMID]
- Tahan M, Kalantari M. Determine the effectiveness of dare training on social disorders of the students of the blind, Rooyesh-e-Ravanshenasi J. 2019; 8(2):125-32. [Link]
Type of Study: Research |
Subject:
Optometry
Received: 2022/12/11 | Accepted: 2023/02/5 | Published: 2022/02/3
Received: 2022/12/11 | Accepted: 2023/02/5 | Published: 2022/02/3
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.