

Volume 5, Issue 1 (Continuously Updated 2022)
Func Disabil J 2022, 5(1): 0-0 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Darooifard A, Jalilevand N, Torabinezhad F, Kamali M. Analyzing Acoustic Characteristics of Voice for Children With Cleft Palate With and Without Compensatory Error Compared to Normal Children. Func Disabil J 2022; 5 (1) : 52
URL: http://fdj.iums.ac.ir/article-1-180-en.html
URL: http://fdj.iums.ac.ir/article-1-180-en.html



1- Department of Speech Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,jalilevand.n@iums.ac.ir
3- Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Speech Therapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
3- Department of Rehabilitation Management, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 952 kb]
(780 Downloads)
| Abstract (HTML) (1919 Views)
Full-Text: (742 Views)
1. Introduction
Speech is the result of various muscles’ coordination, including lips, tongue, velopharyngeal system, and vocal folds. Many disorders regarding speech production are because of the structural abnormalities of the speech organs [1]. Accordingly, studies have proved that 20% to 30% of patients with repaired cleft palate show speech production disorders because of Velopharyngeal Insufficiency (VPI) [2]. This is a disorder that results from improper closure of the soft palate against the posterior pharyngeal wall during speech. The inadequacy of the pharyngeal valve allows the air to escape from the nose during speech, which causes hypernasal and unintelligible speech. One of the causes of VPI is the abnormal anatomical structures in the soft palate. The most common cause of VPI is cleft palate or submucosal cleft [3]. Children with cleft lip and or palate repaired may show VPI that results in nasal air emission, nasal or facial grimacing, compensatory errors, obligatory errors, and misarticulation [4].
To evaluate the speech characteristics of individuals with cleft palate, Henningsson et al. introduced various parameters, including hypernasality, hyponasality, nasal air emission, articulation errors, and voice problems [5]. Compensatory errors are one of the speech problems that affect the speech clarity and acceptability of people with cleft palates. The compensatory errors include glottal stops, pharyngeal stops, pharyngeal fricative, pharyngeal affricative, posterior nasal fricative, nasal fricative, and mid-dorsum palatal stops [6].
Boltezar et al. (2006) reported that 9.2% of children with cleft lip and palate had functional voice problems and hoarseness. Boltezar et al. concluded that Ear, Nose, and Throat (ENT) specialists should play an active role in treating cleft palate children [7]. Structural defects, such as cleft palate, affect the vocal cords and changes the quality of sound; therefore, individuals who have oral clefts require voice assessment [8]. People with cleft palate are at risk of voice disorders because of laryngeal hyperactivity, resulting from compensatory error production [9]. For instance, a more laryngeal function is required during glottal stop production; therefore, this leads to damage to the vocal folds and vocal disturbances.
Gonzalez et al. (2015) examined the acoustic characteristics of 14 children with unilateral cleft lip and palate who had VPI compared to normal children. The fundamental frequency (f0) was higher in cleft palate children compared to their normal peers. Moreover, the shimmer was greater in the cleft palate group compared to normal children. Gonzalez et al. (2015) concluded it seems reasonable to offer voice therapy in the speech and language pathologist’s treatment plan for children with VPI [10]. Mojiri et al. (2011) examined the acoustic characteristics of children with VPI at the age of 4 to 8 years and compared them to their normal peers. The results showed no significant differences between the mean f0, jitter, and shimmer in the children with VPI and their normal peers [9]. Dehghan (2019) studied the acoustic characteristics of the voice of 30 children with cleft palate and VPI and their normal peers at the age of 6 to 12 years. He reported no significant difference between the two groups of children in the shimmer [11].
Aydinli et al. studied the effect of the glottal stop on the voice of cleft palate children. The results showed that the acoustic features of children who use glottal stops were significantly different from children who did not use it [12].
The voice assessment of young children with cleft palate with and without compensatory error can help in early detection, prevention, and intervention in treating voice disorders.
The acoustic voice analysis as a clinical document by measuring the frequency, intensity (amplitude), perturbation (jitter and shimmer), and range can provide information about vocal fold movement. Measure, such as f0, amplitude, and signal-to-noise ratio (harmonics-to-noise ratio [HNR]) are the acoustic signs of voice problems [13].
The purpose of this study is to answer the following questions:
Are the acoustic characteristics of the voice of children with cleft palate in the age range of 48 to 60 months different from their normal peers?
Are the acoustic characteristics of the voice different in children with cleft palate with and without using compensatory errors?
2. Materials and Methods
Patients
In this descriptive-analytical and cross-sectional study, 38 Persian-speaking children from the age of 48 to 60 months participated in two groups: cleft palate and normal. The cleft palate children were referred to speech therapy centers in Tehran and their peers were in the accessible kindergartens. The inclusion criteria were being monolingual (Persian language), being in the age range of 48 to 60 months, no sensorineural hearing loss, and no obvious voice disorders. The exclusion criteria were a lack of speech intelligibility and a lack of cooperation in speech sample recording.
The parents signed an informed consent form. The speech samples were recorded in a quiet room with noises less than 45 dB [13]. The children’s voices were recorded using the AKG C555 headset microphone, located 10 cm to the left of their mouths [9, 14]. The microphone was connected to an ASUS K43S laptop, which contained the Audacity software, connected to an external sound card [13]. The speech sample was recorded in 2 ways:
Sustained utterance of vowels /a/ and /i/ [14] for 4 to 5 s; repeating the given words and sentences.
The speech analysis of samples was performed in the following procedure:
For the acoustic analysis of the sound, 0.5 s was removed at the beginning of the sustained vowel, and then 3 s was selected. Meanwhile, the acoustic parameters, including f0, jitter and shimmer, and HNR were performed using the Praat software, version 6.0.36.
The second speech samples were recorded to diagnose misarticulation and compensatory error production via the test of repeating the given words and sentences [15] along with the speech intelligibility test [16]. The word and sentence repetition test included 40 single words and 17 sentences that are reported by Amiriyan et al. as an acceptable and reliable test to assess children’s speech [15]. Introduced by Heydari et al. as an acceptable and reliable test for Persian language children, the speech intelligibility test includes 47 pictures [16].
Two experts heard and recorded the speech of children with cleft palate. They diagnosed and separated children into 2 groups: with and without compensatory errors. Subsequently, the cleft palate children were divided into 2 groups: with and without compensatory errors. The grade, roughness, breathiness, asthenia, strain (GRBAS) perceptual auditory assessment scale was used to diagnose voice disorders in children [17]. The data were analyzed using the SPSS software, version 21. The level of significance was considered P<0.05.
3. Results
A total of 38 children in the age range of 48 to 60 months participated in this study. The group of 17 children with repaired cleft palate included 8 boys and 9 girls while the group of 21 normal children included 9 boys and 12 girls. Table 1 demonstrates the two groups of participants in this study.
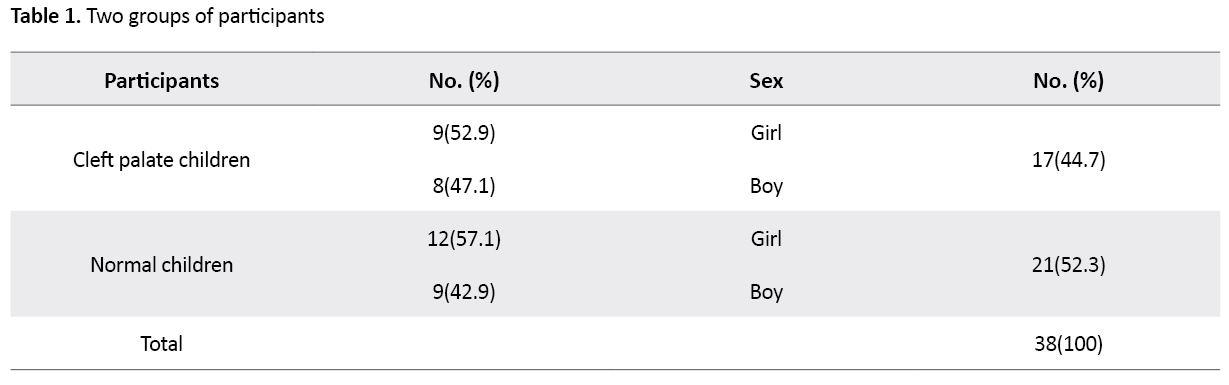
Table 2 summarizes the acoustic characteristics of the voice for two groups of children with cleft palate and normal.

The hypothesis of the non-normal distribution of data was rejected via the Smirnov-Kolmogorov test (P<0.05). Therefore, given the normality of the data, the independent samples t test was used to compare the means of the data.
Table 2 summarizes the Mean±SD f0, jitter, shimmer, and HNR for the two groups. There is a significant difference (P=0.049) between children with cleft palate and their normal peers in the shimmer of the vowel /a/.
Figure 1 shows the shimmer in the vowel /a/ in both groups of children.
.jpg) Table 3 demonstrates the mean±SD f0, jitter, shimmer, and HNR between cleft palate children with and without compensatory errors in the production of the vowels /a/ and /i/.
Table 3 demonstrates the mean±SD f0, jitter, shimmer, and HNR between cleft palate children with and without compensatory errors in the production of the vowels /a/ and /i/.
.jpg)
There is no significant difference in the acoustic parameters of the voice between the two groups of children with cleft palate with and without compensatory errors (P<0.05). The acoustic parameters for girls and boys in the two groups of cleft palate children with and without compensatory were compared as well. There is a significant difference in the average HNR in the production of the vowel /a/ between the boy and girls (P=0.02). Figure 2 shows the average HNR for cleft palate children with and without compensatory errors.
.jpg) The HNR is higher in boys compared to girls.
The HNR is higher in boys compared to girls.
4. Discussion
Children with cleft lip and palate may be at risk of voice disorders; therefore, they need to be assessed by a speech and language pathologist for early voice problems diagnosis and intervention. Most commonly, the acoustic parameters of voice, including the perturbation measures of pitch (jitter), amplitude (shimmer), and HNR are used to evaluate the voice quality [11]. The jitter is the parameter of frequency variation from cycle to cycle and the shimmer is the amplitude during phonation [18]. The acoustic analysis as a clinical document shows perceptual signs of voice problems. Therefore, at least a speech and language pathologist can determine the perceptual signs of voice problems in children with cleft lip and palate immediately by voice sample analysis.
Children with VPI may use pharyngeal or laryngeal production as a place of articulation. Thus, these patients are at risk for voice disorders [19]. Studies show that more subglottic pressure during talking leads to hyperfunction of the larynx [19]. Voice problems in children with cleft palate and VPI were reported [18, 20]. Robinson and Otteson reported a 5.5% prevalence of hoarseness in the cleft palate population. The laryngoscopic findings showed vocal fold nodules and edema, or mucosal thickening of the vocal folds in the children with hoarseness [18].
In the current study, the acoustic characteristics of speech sounds in children at the age of 48 to 60 months were compared to their normal peers. The findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children. The other findings of this study are as follows:
The results showed a significant difference between the two groups of children in the average shimmer of the vowel /a/ (P=0.049). The average shimmer values for the cleft palate children, producing the vowel /a/ (2.79 dB) was lower than their normal peers (3.71dB). In this study, all participants with cleft palate showed hypernasality; therefore, the decrease in the shimmer values for the cleft palate children could be due to hypernasality compared to normal children.
The mean HNR in the vowel /a/ for the girls and boys with cleft palate was significantly different (P=0.02). HNR is a parameter that can be used to measure the relationship between the physiological aspects of sound production and its perceptual characteristics [21]. The HNR will increase with less noise energy in the acoustic speech signal. Thus, the HNR in people without voice problems is more than that in people with voice disorders. Our findings showed that the average HNR in the vowel /a/ for the girls (19.76 dB) was lower than for the boys (22.92 dB). Robinson and Otteson reported that the number of girls with hoarseness was more than boys. Therefore, it can be concluded that girls with cleft palate probably had more harmful behaviors to their vocal cords.
The present study aimed to compare the acoustic characteristics of the voice in cleft palate children with and without compensatory errors. The mean f0, jitter, shimmer, and HNR were not significantly different between the two groups of children. There was no significant difference in the acoustic characteristics between the two groups (with or without compensatory errors). The findings of Aydinli et al. (2015) showed that f0, jitter, and shimmer were significantly different between the individuals with and without glottal stop, used as compensatory errors [12]. In the present study, 35% of children with cleft palate used glottal stop. If children only use the glottal stop, the acoustic characteristics of their voice will be more affected.
Villafuerte-Gonzalez et al. reported that f0 was higher in cleft palate boys compared to their peers. Meanwhile, the shimmer was greater in the cleft palate group than in normal children [10]. The current study findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children.
Mojiri et al. reported no significant differences between the mean f0, jitter, and shimmer in the children with VPI and their normal peers [9].
The results of the present study showed a significant difference between the two groups of children with cleft palate and their normal peers in the average shimmer of the vowel /a/. Dehghan reported no significant difference between the two groups of children in the shimmer [11].
5. Conclusion
The findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children in the age range of 48 to 60 months. These findings could be the cause that no children complain about voice problems. One of the most important limitations of this study was related to the COVID-19 pandemic, as the most important factor for the lack of access to children in the selected age range (48 to 60 months). Accordingly, more populations with cleft lip and palate are needed in future studies.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Iran University of Medical Sciences approved the study (Code: IR.IUMS.REC.1398.519).
Funding
This study was a part of an MSc. thesis of the first author supported by the Iran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are grateful for the support of the Vice Chancellor for Research of Iran University of Medical Sciences. We express our gratitude to the parents of children and the officials of participating centers.
References
Speech is the result of various muscles’ coordination, including lips, tongue, velopharyngeal system, and vocal folds. Many disorders regarding speech production are because of the structural abnormalities of the speech organs [1]. Accordingly, studies have proved that 20% to 30% of patients with repaired cleft palate show speech production disorders because of Velopharyngeal Insufficiency (VPI) [2]. This is a disorder that results from improper closure of the soft palate against the posterior pharyngeal wall during speech. The inadequacy of the pharyngeal valve allows the air to escape from the nose during speech, which causes hypernasal and unintelligible speech. One of the causes of VPI is the abnormal anatomical structures in the soft palate. The most common cause of VPI is cleft palate or submucosal cleft [3]. Children with cleft lip and or palate repaired may show VPI that results in nasal air emission, nasal or facial grimacing, compensatory errors, obligatory errors, and misarticulation [4].
To evaluate the speech characteristics of individuals with cleft palate, Henningsson et al. introduced various parameters, including hypernasality, hyponasality, nasal air emission, articulation errors, and voice problems [5]. Compensatory errors are one of the speech problems that affect the speech clarity and acceptability of people with cleft palates. The compensatory errors include glottal stops, pharyngeal stops, pharyngeal fricative, pharyngeal affricative, posterior nasal fricative, nasal fricative, and mid-dorsum palatal stops [6].
Boltezar et al. (2006) reported that 9.2% of children with cleft lip and palate had functional voice problems and hoarseness. Boltezar et al. concluded that Ear, Nose, and Throat (ENT) specialists should play an active role in treating cleft palate children [7]. Structural defects, such as cleft palate, affect the vocal cords and changes the quality of sound; therefore, individuals who have oral clefts require voice assessment [8]. People with cleft palate are at risk of voice disorders because of laryngeal hyperactivity, resulting from compensatory error production [9]. For instance, a more laryngeal function is required during glottal stop production; therefore, this leads to damage to the vocal folds and vocal disturbances.
Gonzalez et al. (2015) examined the acoustic characteristics of 14 children with unilateral cleft lip and palate who had VPI compared to normal children. The fundamental frequency (f0) was higher in cleft palate children compared to their normal peers. Moreover, the shimmer was greater in the cleft palate group compared to normal children. Gonzalez et al. (2015) concluded it seems reasonable to offer voice therapy in the speech and language pathologist’s treatment plan for children with VPI [10]. Mojiri et al. (2011) examined the acoustic characteristics of children with VPI at the age of 4 to 8 years and compared them to their normal peers. The results showed no significant differences between the mean f0, jitter, and shimmer in the children with VPI and their normal peers [9]. Dehghan (2019) studied the acoustic characteristics of the voice of 30 children with cleft palate and VPI and their normal peers at the age of 6 to 12 years. He reported no significant difference between the two groups of children in the shimmer [11].
Aydinli et al. studied the effect of the glottal stop on the voice of cleft palate children. The results showed that the acoustic features of children who use glottal stops were significantly different from children who did not use it [12].
The voice assessment of young children with cleft palate with and without compensatory error can help in early detection, prevention, and intervention in treating voice disorders.
The acoustic voice analysis as a clinical document by measuring the frequency, intensity (amplitude), perturbation (jitter and shimmer), and range can provide information about vocal fold movement. Measure, such as f0, amplitude, and signal-to-noise ratio (harmonics-to-noise ratio [HNR]) are the acoustic signs of voice problems [13].
The purpose of this study is to answer the following questions:
Are the acoustic characteristics of the voice of children with cleft palate in the age range of 48 to 60 months different from their normal peers?
Are the acoustic characteristics of the voice different in children with cleft palate with and without using compensatory errors?
2. Materials and Methods
Patients
In this descriptive-analytical and cross-sectional study, 38 Persian-speaking children from the age of 48 to 60 months participated in two groups: cleft palate and normal. The cleft palate children were referred to speech therapy centers in Tehran and their peers were in the accessible kindergartens. The inclusion criteria were being monolingual (Persian language), being in the age range of 48 to 60 months, no sensorineural hearing loss, and no obvious voice disorders. The exclusion criteria were a lack of speech intelligibility and a lack of cooperation in speech sample recording.
The parents signed an informed consent form. The speech samples were recorded in a quiet room with noises less than 45 dB [13]. The children’s voices were recorded using the AKG C555 headset microphone, located 10 cm to the left of their mouths [9, 14]. The microphone was connected to an ASUS K43S laptop, which contained the Audacity software, connected to an external sound card [13]. The speech sample was recorded in 2 ways:
Sustained utterance of vowels /a/ and /i/ [14] for 4 to 5 s; repeating the given words and sentences.
The speech analysis of samples was performed in the following procedure:
For the acoustic analysis of the sound, 0.5 s was removed at the beginning of the sustained vowel, and then 3 s was selected. Meanwhile, the acoustic parameters, including f0, jitter and shimmer, and HNR were performed using the Praat software, version 6.0.36.
The second speech samples were recorded to diagnose misarticulation and compensatory error production via the test of repeating the given words and sentences [15] along with the speech intelligibility test [16]. The word and sentence repetition test included 40 single words and 17 sentences that are reported by Amiriyan et al. as an acceptable and reliable test to assess children’s speech [15]. Introduced by Heydari et al. as an acceptable and reliable test for Persian language children, the speech intelligibility test includes 47 pictures [16].
Two experts heard and recorded the speech of children with cleft palate. They diagnosed and separated children into 2 groups: with and without compensatory errors. Subsequently, the cleft palate children were divided into 2 groups: with and without compensatory errors. The grade, roughness, breathiness, asthenia, strain (GRBAS) perceptual auditory assessment scale was used to diagnose voice disorders in children [17]. The data were analyzed using the SPSS software, version 21. The level of significance was considered P<0.05.
3. Results
A total of 38 children in the age range of 48 to 60 months participated in this study. The group of 17 children with repaired cleft palate included 8 boys and 9 girls while the group of 21 normal children included 9 boys and 12 girls. Table 1 demonstrates the two groups of participants in this study.
.jpg)
Table 2 summarizes the acoustic characteristics of the voice for two groups of children with cleft palate and normal.
.jpg)
The hypothesis of the non-normal distribution of data was rejected via the Smirnov-Kolmogorov test (P<0.05). Therefore, given the normality of the data, the independent samples t test was used to compare the means of the data.
Table 2 summarizes the Mean±SD f0, jitter, shimmer, and HNR for the two groups. There is a significant difference (P=0.049) between children with cleft palate and their normal peers in the shimmer of the vowel /a/.
Figure 1 shows the shimmer in the vowel /a/ in both groups of children.
There is no significant difference in the acoustic parameters of the voice between the two groups of children with cleft palate with and without compensatory errors (P<0.05). The acoustic parameters for girls and boys in the two groups of cleft palate children with and without compensatory were compared as well. There is a significant difference in the average HNR in the production of the vowel /a/ between the boy and girls (P=0.02). Figure 2 shows the average HNR for cleft palate children with and without compensatory errors.
4. Discussion
Children with cleft lip and palate may be at risk of voice disorders; therefore, they need to be assessed by a speech and language pathologist for early voice problems diagnosis and intervention. Most commonly, the acoustic parameters of voice, including the perturbation measures of pitch (jitter), amplitude (shimmer), and HNR are used to evaluate the voice quality [11]. The jitter is the parameter of frequency variation from cycle to cycle and the shimmer is the amplitude during phonation [18]. The acoustic analysis as a clinical document shows perceptual signs of voice problems. Therefore, at least a speech and language pathologist can determine the perceptual signs of voice problems in children with cleft lip and palate immediately by voice sample analysis.
Children with VPI may use pharyngeal or laryngeal production as a place of articulation. Thus, these patients are at risk for voice disorders [19]. Studies show that more subglottic pressure during talking leads to hyperfunction of the larynx [19]. Voice problems in children with cleft palate and VPI were reported [18, 20]. Robinson and Otteson reported a 5.5% prevalence of hoarseness in the cleft palate population. The laryngoscopic findings showed vocal fold nodules and edema, or mucosal thickening of the vocal folds in the children with hoarseness [18].
In the current study, the acoustic characteristics of speech sounds in children at the age of 48 to 60 months were compared to their normal peers. The findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children. The other findings of this study are as follows:
The results showed a significant difference between the two groups of children in the average shimmer of the vowel /a/ (P=0.049). The average shimmer values for the cleft palate children, producing the vowel /a/ (2.79 dB) was lower than their normal peers (3.71dB). In this study, all participants with cleft palate showed hypernasality; therefore, the decrease in the shimmer values for the cleft palate children could be due to hypernasality compared to normal children.
The mean HNR in the vowel /a/ for the girls and boys with cleft palate was significantly different (P=0.02). HNR is a parameter that can be used to measure the relationship between the physiological aspects of sound production and its perceptual characteristics [21]. The HNR will increase with less noise energy in the acoustic speech signal. Thus, the HNR in people without voice problems is more than that in people with voice disorders. Our findings showed that the average HNR in the vowel /a/ for the girls (19.76 dB) was lower than for the boys (22.92 dB). Robinson and Otteson reported that the number of girls with hoarseness was more than boys. Therefore, it can be concluded that girls with cleft palate probably had more harmful behaviors to their vocal cords.
The present study aimed to compare the acoustic characteristics of the voice in cleft palate children with and without compensatory errors. The mean f0, jitter, shimmer, and HNR were not significantly different between the two groups of children. There was no significant difference in the acoustic characteristics between the two groups (with or without compensatory errors). The findings of Aydinli et al. (2015) showed that f0, jitter, and shimmer were significantly different between the individuals with and without glottal stop, used as compensatory errors [12]. In the present study, 35% of children with cleft palate used glottal stop. If children only use the glottal stop, the acoustic characteristics of their voice will be more affected.
Villafuerte-Gonzalez et al. reported that f0 was higher in cleft palate boys compared to their peers. Meanwhile, the shimmer was greater in the cleft palate group than in normal children [10]. The current study findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children.
Mojiri et al. reported no significant differences between the mean f0, jitter, and shimmer in the children with VPI and their normal peers [9].
The results of the present study showed a significant difference between the two groups of children with cleft palate and their normal peers in the average shimmer of the vowel /a/. Dehghan reported no significant difference between the two groups of children in the shimmer [11].
5. Conclusion
The findings showed no significant difference in the acoustic characteristics of the mean f0, jitter, and HNR between the two groups of children in the age range of 48 to 60 months. These findings could be the cause that no children complain about voice problems. One of the most important limitations of this study was related to the COVID-19 pandemic, as the most important factor for the lack of access to children in the selected age range (48 to 60 months). Accordingly, more populations with cleft lip and palate are needed in future studies.
Ethical Considerations
Compliance with ethical guidelines
The Ethics Committee of Iran University of Medical Sciences approved the study (Code: IR.IUMS.REC.1398.519).
Funding
This study was a part of an MSc. thesis of the first author supported by the Iran University of Medical Sciences.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are grateful for the support of the Vice Chancellor for Research of Iran University of Medical Sciences. We express our gratitude to the parents of children and the officials of participating centers.
References
- Kord Zaferanloo Kamboozia A, Seyyedzade Aghdam M, Aghagolzade F. [Study of language family and effect of disorder articulation in cleft palate persons after surgery (Persin)]. Lnguage Stud. 2013; 3(5):53-70. [Link]
- Hosseinabad HH, Derakhshandeh F, Mostaajeran F, Abdali H, Davari HA, Hassanzadeh A, et al. Incidence of velopharyngeal insufficiency and oronasal fistulae after cleft palate repair: A retrospective study of children referred to Isfahan Cleft Care Team between 2005 and 2009. Int J Pediatr Otorhinolaryngol. 2015; 79(10):1722-6. [PMID]
- Bhuskute A, Skirko JR, Roth C, Bayoumi A, Durbin-Johnson B, Tollefson TT. Association of velopharyngeal insufficiency with quality of life and patient-reported outcomes after speech surgery. JAMA Facial Plast Surg. 2017; 19(5):406-12. [PMID]
- Kummer AW. Cleft palate and craniofacial anomalies: The effects on speech and resonance. San Francisco: Singular; 2001. [Link]
- Henningsson G, Kuehn DP, Sell D, Sweeney T, Trost-Cardamone JE, Whitehill TL, et al. Universal parameters for reporting speech outcomes in individuals with cleft palate. Cleft Palate Craniofac J. 2008; 45(1):1-17. [PMID]
- Peterson-Falzone SJ, Trost-Cardamon JE, Karnell Mp, Hardin-Jones MA. The clinician’s guide to treating cleft palate speech. United States of America: Mosby Elsevier; 2006. [Link]
- Hocevar-Boltezar I, Jarc A, Kozelj V. Ear, nose and voice problems in children with orofacial clefts. J Laryngol Otol. 2006; 120(4):276-81. [PMID]
- Hamming KK, Finkelstein M, Sidman JD. Hoarseness in children with cleft palate. Otolaryngol Head Neck Surg. 2009; 140(6):902-6. [PMID]
- Mojiri F, Moazeni A, Derakhshandeh F, Nouri N, Hoseini SM. [Compare acoustic analysis in children with VPI and normal (Persian)]. J Res Rehabil Sci. 2012; 7(4):540-8. [Link]
- Villafuerte-Gonzalez R, Valadez-Jimenez VM, Hernandez-Lopez X, Ysunza PA. Acoustic analysis of voice in children with cleft palate and velopharyngeal insufficiency. Int J Pediatr Otorhinolaryngol. 2015; 79(7):1073-6. [PMID]
- Dehqan A. [Acoustic analysis of voice in children with cleft palate and velopharyngeal insufficiency (Persian)]. Jundishapur Sci Med J. 2019; 18(3):215-23. [DOI:10.22118/ JSMJ.2019.189201.1691]
- Aydınlı FE, Özcebe E, Kulak Kayıkçı ME, Yılmaz T, Özgür FF. Investigating the effects of glottal stop productions on voice in children with cleft palate using multidimensional voice assessment methods. J Voice. 2016; 30(6):763.e9-763.e15. [PMID]
- Stevens K, Bressmann T, Gong SG, Tompson BD. Impact of a rapid palatal expander on speech articulation. Am J Orthod Dentofacial Orthop. 2011; 140(2):e67-75. [PMID]
- Safaiean A, Jalilevand N, Ebrahimipour M, Asleshirin E, Hiradfar M. Speech intelligibility after repair of cleft lip and palate. Med J Islam Repub Iran. 2017; 31:85. [DOI:10.14196/ mjiri.31.85] [PMID]
- Amiryan A, Derakhshandeh F, Salehi A, Soleimani B. [Evaluating intra- and inter-rater reliability forcleft palate speech assessment test based on universal parameters system- in Persian (Persian)]. J Res Rehabil Sci. 2011; 7(4):470-6. [Link]
- Heydari S, Torbinezhad F, Agharasuli F, Hoseyni F. [Development of speech intelligibility measurement test for 3 to 5 years old normal children (Persian)]. Audiol. 2011; 20(1):47-53. [Link]
- Karnell MP, Melton SD, Childes JM, Coleman TC, Dailey SA, Hoffman HT. Reliability of clinician-based (GRBAS and CAPE-V) and patient-based (V-RQOL and IPVI) documentation of voice disorders. J Voice. 2007; 21(5):576-90. [PMID]
- Colton RH,. Casper JK, Leonard R. Understanding voice problems: A physiological perspective for diagnosis and treatment. Philadelphia: Lippincott Williams & Wilkins; 2006. [Link]
- Sinko K, Gruber M, Jagsch R, Roesner I, Baumann A, Wutzl A, et al. Assessment of nasalance and nasality in patients with a repaired cleft palate. Eur Arch Otorhinolaryngol. 2017; 274(7):2845-54. [PMID]
- Nikhila KG, Prasad H. A study on patterns of compensatory articulation errors with reference to age of surgery in children with repaired cleft lip and palate. Glob J Oto. 2017; 7(2):555706. [DOI:10.19080/ GJO.2017.07.555706]
Type of Study: Research |
Subject:
Speech Therapy
Received: 2022/05/4 | Accepted: 2022/08/9 | Published: 2022/11/8
Received: 2022/05/4 | Accepted: 2022/08/9 | Published: 2022/11/8
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.