

Volume 3, Issue 1 (Continuously Updated 2020)
Func Disabil J 2020, 3(1): 169-178 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Farahmand B, Mohammadi M, Hassanbeygi B, Mohammadi M, Saeedi H, Bagherzadeh Cham M. Ergonomic Evaluation of Working Conditions in Orthotists and Prosthetists by Rapid Entire Body Assessment (REBA). Func Disabil J 2020; 3 (1) :169-178
URL: http://fdj.iums.ac.ir/article-1-143-en.html
URL: http://fdj.iums.ac.ir/article-1-143-en.html
Behshid Farahmand1 

 , Maryam Mohammadi1 , Babak Hassanbeygi2 , Morteza Mohammadi1 , Hassan Saeedi1 , Masumeh Bagherzadeh Cham *3
, Maryam Mohammadi1 , Babak Hassanbeygi2 , Morteza Mohammadi1 , Hassan Saeedi1 , Masumeh Bagherzadeh Cham *3
, Maryam Mohammadi1 , Babak Hassanbeygi2 , Morteza Mohammadi1 , Hassan Saeedi1 , Masumeh Bagherzadeh Cham *3
1- Department of Orthotics & Prosthetics, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Biomedical Engineering, Hong Kong Polytechnic University, Hong Kong, China.
3- Department of Orthotics & Prosthetics, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,bagherzadehcham.m@iums.ac.ir
2- Department of Biomedical Engineering, Hong Kong Polytechnic University, Hong Kong, China.
3- Department of Orthotics & Prosthetics, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran. ,
Keywords: Musculoskeletal disorders, Nordic musculoskeletal questionnaire, Rapid entire body assessment score, Orthotist, Prosthetist
Full-Text [PDF 1215 kb]
(1168 Downloads)
| Abstract (HTML) (1858 Views)
Full-Text: (1152 Views)
1. Introduction
Occupation-related musculoskeletal injuries are among the most serious occupational problems worldwide. Unfavorable occupational body position is one of the most important factors in these injuries. Based on estimates by the Health and Safety Executive, work-related Musculoskeletal Disorders (MSDs) account for 38% of the work-related disorders [1]. These problems reduced quality in work and production, increased the work time loss, reduced overall work time for every person, and also enforced more prices on the workers and governments [1, 2].
One of the ergonomist’s main goals is to improve musculoskeletal health in the workplace [3]. Intervening programs, standards, and several instructions have been inducted to reduce the occurrence rate of these disorders among the working society. Analyzing the levels of the prevention of the factors leading to these disorders can be the basis of programming and ergonomic interventions in the workplace [1, 4]. Although many factors, such as biomechanical dangers, genetic factors, morphological defects, and psychosocial disease lead to work-related problems, it is only possible to control the biomechanical and psychosocial factors [3].
Body position in the workplace can lead to work-related MSDs. According to studies, to determine the intensity of physical activity, it is necessary to consider body position, the range of motion, force applied, the number of the repetitions of the activity, and the duration of work [3]. Among these, the work motions and positions are important factors that must be included in the professional health analysis. Studies show that people’s position during work is directly tied to their MSDs [3, 5]. Improper, asymmetric, repeated, and continuous working positions pose excessive pressure on the body structure, eventually, this force exceeds the maximum body stress and leads to injuries [3]. Therefore, it can be a good base for decision-making about workplace changes and ergonomic interferences to analyze and determine the danger of bad body position during work and its effect on MSDs [6]. There is a possibility of MSDs among orthotists and prosthetists, because of long-standing work, excessive forces, the use of inappropriate and nonstandard tools and machines, and the lack of awareness of the correct physical position [7]. Therefore, this study aimed to determine the prevalence rate of MSDs and perform the ergonomic evaluation of working conditions in orthotists and prosthetists using the Rapid Entire Body Assessment (REBA).
2. Material and Methods
This cross-sectional study was conducted in 10 active orthotic and prosthetic clinics in Tehran City, Iran. The clinics included the Orthotics and Prosthetics Center of the Rehabilitation Faculty of Iran University of Medical Sciences, the Kosar Orthotics and Prosthetics Center, the Saba Technical Orthopedic Center of University of Welfare and Rehabilitation Sciences, and seven private clinics in Tehran. Also, 40 orthotists and prosthetists, including 16 males and 24 females with at least one year of work experience participated in the study.
To calculate the prevalence of MSDs, the participants answered the Nordic Musculoskeletal Questionnaire (NMQ) before the observation of the working positions [8]. This questionnaire is a valid and reliable screening tool for detecting MSDs [9]. The NMQ includes 27 items that explore the presence of musculoskeletal symptoms during 12 months and cover nine different parts of the body (neck, shoulders, elbows, wrists/hands, upper back, lower back, hip/thighs, knees, and ankles/feet). The NMQ also includes items on severity grades, which are determined according to functional status and the presence of musculoskeletal symptoms during the last seven days. All answers are given on a dichotomous “yes/no” response scale [8, 9]. Besides, questions, such as work experience and the dominant hand were added to address the study purpose. Postures were evaluated with the scores of the Rapid Entire Body Assessment (REBA), which is a useful tool to analyze whole-body static, dynamic, or unstable modes [10, 11]. This method was developed by Hignett and McAtamney, in 2000. Besides comprehensiveness, REBA is highly sensitive especially to analyze the unpredictable postures of people working in the health care and other service sectors. Analysis indicates that the REBA method has a reasonable inter and intra-rater reliability (ICC=0.925) to analyze working postures [12].
In the REBA method, the body limbs are divided into two groups of A (trunk, neck, legs) with 60 posture combinations and B (shoulders, elbows, and wrists) with 36 posture combinations. In this method, by observing the working postures, each of the limbs in groups A and B is scored based on the angular position. The A and B scores are combined to give a total of 144 possible combinations, and finally, an activity score is added to give the final REBA score. The REBA score resides on a scale from 1 to 15 that shows not only the amount of risk threatening the person’s musculoskeletal system in the analyzed working posture but also the activity levels needed against this risk to treat or not to treat the working posture [10] (Table 1).
.PNG)
Ten working postures were set for each of the orthotists and prosthetists by an expert examiner and consulting with two other persons working on each of the professions. The working postures considered for a prosthetic worker were as follows: casting, positive cast modification, the modification of soft socket by milling machine, pulling the PVA bag and/or prosthesis stocking on a mold, lamination procedure, cutting the negative cast using cast cutter, removing the plaster from the socket using a pneumatic hammer, the modification of socket by milling machine, forming Pedilon or prosthesis foam cover by milling machine, and prosthesis assembling (Figure 1).
.PNG)
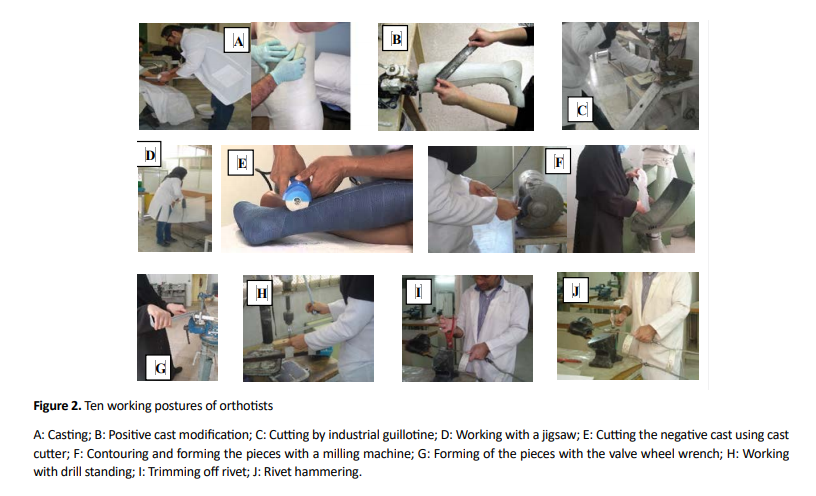
Also, casting, positive cast modification, cutting by industrial guillotine, working with a jigsaw, cutting the negative cast using cast cutter, contouring and forming the pieces with a milling machine, forming of the pieces with the valve wheel wrench, working with drill standing, trimming off rivet, and rivet hammering were considered for an orthotic worker (Figure 2).
The positions of the body limbs are not constant during each task and they need to be scored carefully. Thus, during each working posture, each subject was filmed for 10 minutes from different angles. In these films, the posture used most was chosen and its data were analyzed via the Kinovea software, based on the REBA employee assessment worksheet [13]. The obtained data were analyzed using SPSS V. 21, also, the significant level was set at P ≤0.05. The chi-squared (test of independence) and the Fisher exact test were used to determine the relationship between the REBA score and specialty, gender, weight, height, and work experience. Also, the chi-squared test was used to evaluate the statistical differences between gender and specialty.
3. Results
Table 2 shows the demographic characteristics of the study population.
.PNG)
Table 3 represents high-risk work-related MSDs in the different body limbs of the orthotists and prosthetists during the last year, based on specialty and gender.
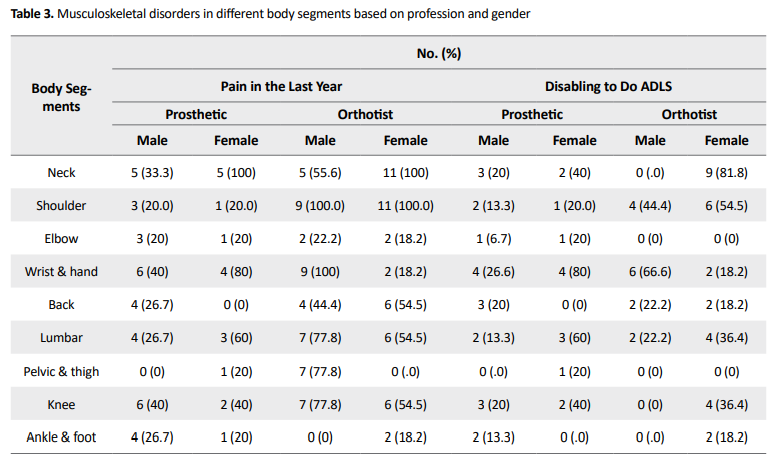
The results showed that all of the female orthotists were complaining of neck and shoulder pain while all of the female prosthetists were suffering from neck disorders. All of the men in the orthotist group had shoulder, wrist, and hand pain, while most of the men in the prosthetist group were suffering from knee, shoulder, wrist, and hand pain.
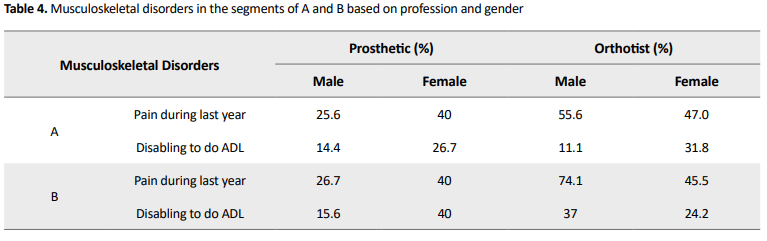
The data of REBA score (Table 4) show that 55.6% of men orthotists suffer pain in the A group. The orthotist women take second place in this table, with 47% during the last year. Such high statistics were not seen in orthotists. Nearly similar results were seen for the B group so that the orthotist men by 74.1% and women by 45.5% suffer from pain in this group.

Moreover, 65% of the orthotist workers were unable to be present in the workplace because of MSDs; most of them (55%) were women. Such high statistics were not seen in the prosthetist workers. Cumulatively, an absence rate of 26.6% was reported because of work-related MSDs. Besides, 50% of the orthotists reported a history of doctor’s visits for MSDs; this rate was 30% in the prosthetist workers. Generally, the workers reported a doctor reference rate of 26.6%.
The statistical test of chi-squared shows a significant relationship between the gender of orthotists and their actions disability during the last year because of disorders in group A (P = 0.013) and also pain and disorder in group B (P = 0.048) in the past year. Table 4 indicates a significant relationship between specialty and the disorder’s prevalence during the last year in group A (P ≤ 0.0005) and group B (P ≤ 0.0005), in men workers. The Fisher test indicated a significant dependence between the weight of men working in the orthotic section and the inability to work during the last year because of pain in group A (P = 0.019). There is no significant relationship between the height, age, and experience of the participants and the musculoskeletal pain and disorder and inability because of MSDs in group A or B.
Tables 5 and 6 show the REBA score of orthotists and prosthetists during the specified activities, respectively. The Fisher test showed no significant dependence between the REBA score achieved during each of the mentioned tasks and the worker’s gender and weight. Among the men prosthetists, significant relations were observed between the REBA score achieved during the “modification of socket by milling machine” and the age (P = 0.046) and experience (P = 0.029). Also in the orthotist workers, a significant dependence was found between the REBA score achieved during the “contouring and forming the pieces with a milling machine” and the height (P = 0.024). However, the Fisher test did not show any significant statistical dependence during the performance of the duties defined for prosthesis specialists and the MSDs in their B part of the body.
The chi-squared statistical test showed a significant relationship between the disorders in the A group of men prosthesis specialists in the past year and the REBA score achieved during the “lamination procedure” (P = 0.040). Also, the t test did not show significant statistical differences in the REBA score in both men and women workers in orthotists and prosthetists (P>0.05).
4. Discussion
The results of the current study indicated that most of the orthotist men (55.6%) and women (47%) suffered from pain and disorder in their A part of the body, during the past year. Previous studies have also shown that most of the A part of the body (trunk, neck, and legs) is involved in MSDs [14-16]. Also, 65% of orthotists were forced to be absent at work, owing to MSD during the last year. However, these results were not observed among the prosthetists; the reason could be prolonged and repetitive work with hand tools and vibrating devices in the orthotist group. The REBA scores of more than 60% of orthotists and prosthetists were in the range of “4 to 7” and then in the range of “8 to 10”. Only when “removing the plaster from the socket with a pneumatic hammer”, the prosthetist specialists had a score range of “11 to 15”. The score range achieved during this task started from “4 to 7” and the score achieved by 75% of these participants is from “8 to 10”. While among orthotists, the “forming of the pieces with the valve wheel wrench” and “casting” had a score range of “11 to 15” (Table 1). The score range achieved during this duty was started from “4 to 7” and the scores of 70% of the orthotists were in the range of “8 to 10”.
The present study indicated the same levels of risk for men and women in the analysis of different participant’s work postures using the REBA method. Therefore, the average REBA scores acquired from the tasks in the orthotic section did not significantly differ between men and women. These findings are contradicting the research findings about the ergonomic analysis of work postures and the work-related MSDs of hairdressers [15], nurses [14], emergency department personnel [6], and dentists [5], because in these results the rate of injuries was higher in women than in men.
In both orthotists and prosthetists, the highest prevalence of MSD was observed in the neck and shoulders as well as the wrists and hands. Also, among the tasks analyzed, the highest risk of injury/injuries confrontation belonged to the working postures of “casting,” “forming of the pieces with the valve wheel wrench,” and “removing the plaster from the socket using a pneumatic hammer”.
Based on the present findings, important factors that caused MSDs in orthotists and prosthetists were as follows: the poor design of tools and machines, improper workshop design in orthosis and prosthesis clinics, working in standing position for several hours, the lifting and manual handling of heavy objects (mold) without coworker, working with vibrating devices (milling machine, drill, etc), and repetitive tasks.
To improve the situation and reduce the risk of injury, it is recommended to adjust the height and angle of the work surface, reduce longtime standing and repetitive work, provide adjustable tools and machines, and utilize a coworker. Also, it is better to add an ergonomics course, service training, and refresher courses to increase the participants’ knowledge about the profession and the use of tools and devices designed or reformed/modified based on ergonomic principles to decrease the risk of MSDs [17].
This study only investigated 10 repetitive situations for each specialist, while working in the field of orthoses and prostheses is complex. Also, the results may not be generalizable because the type of equipments, the manner of arrangement, and the style of working are different in orthotic and prosthetic clinics.
5. Conclusion
Based on the findings, the rate of MSDs is high in the orthotist and prosthetist, especially in the orthotists. Thus, to reduce the MSDs, it is recommended to provide more educational and preventive strategies, such as adding an ergonomics course, service training, and refresher courses to increase the participants’ knowledge. Also, it is suggested to modify the tools based on the principles of ergonomics.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors declared no conflicts of interest
Acknowledgments
All author would link to thank Staff working in the Orthotics and Prosthetics Rehabilitation Center of the Red Crescent, the Rehabilitation Faculty of Tehran University of Medical Sciences, Kosar Orthotics and Prosthetics Center, Saba Technical Orthopedic Center (related to the University of Welfare and Rehabilitation Sciences), and the private clinics in Tehran.
References
Occupation-related musculoskeletal injuries are among the most serious occupational problems worldwide. Unfavorable occupational body position is one of the most important factors in these injuries. Based on estimates by the Health and Safety Executive, work-related Musculoskeletal Disorders (MSDs) account for 38% of the work-related disorders [1]. These problems reduced quality in work and production, increased the work time loss, reduced overall work time for every person, and also enforced more prices on the workers and governments [1, 2].
One of the ergonomist’s main goals is to improve musculoskeletal health in the workplace [3]. Intervening programs, standards, and several instructions have been inducted to reduce the occurrence rate of these disorders among the working society. Analyzing the levels of the prevention of the factors leading to these disorders can be the basis of programming and ergonomic interventions in the workplace [1, 4]. Although many factors, such as biomechanical dangers, genetic factors, morphological defects, and psychosocial disease lead to work-related problems, it is only possible to control the biomechanical and psychosocial factors [3].
Body position in the workplace can lead to work-related MSDs. According to studies, to determine the intensity of physical activity, it is necessary to consider body position, the range of motion, force applied, the number of the repetitions of the activity, and the duration of work [3]. Among these, the work motions and positions are important factors that must be included in the professional health analysis. Studies show that people’s position during work is directly tied to their MSDs [3, 5]. Improper, asymmetric, repeated, and continuous working positions pose excessive pressure on the body structure, eventually, this force exceeds the maximum body stress and leads to injuries [3]. Therefore, it can be a good base for decision-making about workplace changes and ergonomic interferences to analyze and determine the danger of bad body position during work and its effect on MSDs [6]. There is a possibility of MSDs among orthotists and prosthetists, because of long-standing work, excessive forces, the use of inappropriate and nonstandard tools and machines, and the lack of awareness of the correct physical position [7]. Therefore, this study aimed to determine the prevalence rate of MSDs and perform the ergonomic evaluation of working conditions in orthotists and prosthetists using the Rapid Entire Body Assessment (REBA).
2. Material and Methods
This cross-sectional study was conducted in 10 active orthotic and prosthetic clinics in Tehran City, Iran. The clinics included the Orthotics and Prosthetics Center of the Rehabilitation Faculty of Iran University of Medical Sciences, the Kosar Orthotics and Prosthetics Center, the Saba Technical Orthopedic Center of University of Welfare and Rehabilitation Sciences, and seven private clinics in Tehran. Also, 40 orthotists and prosthetists, including 16 males and 24 females with at least one year of work experience participated in the study.
To calculate the prevalence of MSDs, the participants answered the Nordic Musculoskeletal Questionnaire (NMQ) before the observation of the working positions [8]. This questionnaire is a valid and reliable screening tool for detecting MSDs [9]. The NMQ includes 27 items that explore the presence of musculoskeletal symptoms during 12 months and cover nine different parts of the body (neck, shoulders, elbows, wrists/hands, upper back, lower back, hip/thighs, knees, and ankles/feet). The NMQ also includes items on severity grades, which are determined according to functional status and the presence of musculoskeletal symptoms during the last seven days. All answers are given on a dichotomous “yes/no” response scale [8, 9]. Besides, questions, such as work experience and the dominant hand were added to address the study purpose. Postures were evaluated with the scores of the Rapid Entire Body Assessment (REBA), which is a useful tool to analyze whole-body static, dynamic, or unstable modes [10, 11]. This method was developed by Hignett and McAtamney, in 2000. Besides comprehensiveness, REBA is highly sensitive especially to analyze the unpredictable postures of people working in the health care and other service sectors. Analysis indicates that the REBA method has a reasonable inter and intra-rater reliability (ICC=0.925) to analyze working postures [12].
In the REBA method, the body limbs are divided into two groups of A (trunk, neck, legs) with 60 posture combinations and B (shoulders, elbows, and wrists) with 36 posture combinations. In this method, by observing the working postures, each of the limbs in groups A and B is scored based on the angular position. The A and B scores are combined to give a total of 144 possible combinations, and finally, an activity score is added to give the final REBA score. The REBA score resides on a scale from 1 to 15 that shows not only the amount of risk threatening the person’s musculoskeletal system in the analyzed working posture but also the activity levels needed against this risk to treat or not to treat the working posture [10] (Table 1).
Ten working postures were set for each of the orthotists and prosthetists by an expert examiner and consulting with two other persons working on each of the professions. The working postures considered for a prosthetic worker were as follows: casting, positive cast modification, the modification of soft socket by milling machine, pulling the PVA bag and/or prosthesis stocking on a mold, lamination procedure, cutting the negative cast using cast cutter, removing the plaster from the socket using a pneumatic hammer, the modification of socket by milling machine, forming Pedilon or prosthesis foam cover by milling machine, and prosthesis assembling (Figure 1).
Also, casting, positive cast modification, cutting by industrial guillotine, working with a jigsaw, cutting the negative cast using cast cutter, contouring and forming the pieces with a milling machine, forming of the pieces with the valve wheel wrench, working with drill standing, trimming off rivet, and rivet hammering were considered for an orthotic worker (Figure 2).
The positions of the body limbs are not constant during each task and they need to be scored carefully. Thus, during each working posture, each subject was filmed for 10 minutes from different angles. In these films, the posture used most was chosen and its data were analyzed via the Kinovea software, based on the REBA employee assessment worksheet [13]. The obtained data were analyzed using SPSS V. 21, also, the significant level was set at P ≤0.05. The chi-squared (test of independence) and the Fisher exact test were used to determine the relationship between the REBA score and specialty, gender, weight, height, and work experience. Also, the chi-squared test was used to evaluate the statistical differences between gender and specialty.
3. Results
Table 2 shows the demographic characteristics of the study population.
Table 3 represents high-risk work-related MSDs in the different body limbs of the orthotists and prosthetists during the last year, based on specialty and gender.
The results showed that all of the female orthotists were complaining of neck and shoulder pain while all of the female prosthetists were suffering from neck disorders. All of the men in the orthotist group had shoulder, wrist, and hand pain, while most of the men in the prosthetist group were suffering from knee, shoulder, wrist, and hand pain.
The data of REBA score (Table 4) show that 55.6% of men orthotists suffer pain in the A group. The orthotist women take second place in this table, with 47% during the last year. Such high statistics were not seen in orthotists. Nearly similar results were seen for the B group so that the orthotist men by 74.1% and women by 45.5% suffer from pain in this group.
Moreover, 65% of the orthotist workers were unable to be present in the workplace because of MSDs; most of them (55%) were women. Such high statistics were not seen in the prosthetist workers. Cumulatively, an absence rate of 26.6% was reported because of work-related MSDs. Besides, 50% of the orthotists reported a history of doctor’s visits for MSDs; this rate was 30% in the prosthetist workers. Generally, the workers reported a doctor reference rate of 26.6%.
The statistical test of chi-squared shows a significant relationship between the gender of orthotists and their actions disability during the last year because of disorders in group A (P = 0.013) and also pain and disorder in group B (P = 0.048) in the past year. Table 4 indicates a significant relationship between specialty and the disorder’s prevalence during the last year in group A (P ≤ 0.0005) and group B (P ≤ 0.0005), in men workers. The Fisher test indicated a significant dependence between the weight of men working in the orthotic section and the inability to work during the last year because of pain in group A (P = 0.019). There is no significant relationship between the height, age, and experience of the participants and the musculoskeletal pain and disorder and inability because of MSDs in group A or B.
Tables 5 and 6 show the REBA score of orthotists and prosthetists during the specified activities, respectively. The Fisher test showed no significant dependence between the REBA score achieved during each of the mentioned tasks and the worker’s gender and weight. Among the men prosthetists, significant relations were observed between the REBA score achieved during the “modification of socket by milling machine” and the age (P = 0.046) and experience (P = 0.029). Also in the orthotist workers, a significant dependence was found between the REBA score achieved during the “contouring and forming the pieces with a milling machine” and the height (P = 0.024). However, the Fisher test did not show any significant statistical dependence during the performance of the duties defined for prosthesis specialists and the MSDs in their B part of the body.
The chi-squared statistical test showed a significant relationship between the disorders in the A group of men prosthesis specialists in the past year and the REBA score achieved during the “lamination procedure” (P = 0.040). Also, the t test did not show significant statistical differences in the REBA score in both men and women workers in orthotists and prosthetists (P>0.05).
4. Discussion
The results of the current study indicated that most of the orthotist men (55.6%) and women (47%) suffered from pain and disorder in their A part of the body, during the past year. Previous studies have also shown that most of the A part of the body (trunk, neck, and legs) is involved in MSDs [14-16]. Also, 65% of orthotists were forced to be absent at work, owing to MSD during the last year. However, these results were not observed among the prosthetists; the reason could be prolonged and repetitive work with hand tools and vibrating devices in the orthotist group. The REBA scores of more than 60% of orthotists and prosthetists were in the range of “4 to 7” and then in the range of “8 to 10”. Only when “removing the plaster from the socket with a pneumatic hammer”, the prosthetist specialists had a score range of “11 to 15”. The score range achieved during this task started from “4 to 7” and the score achieved by 75% of these participants is from “8 to 10”. While among orthotists, the “forming of the pieces with the valve wheel wrench” and “casting” had a score range of “11 to 15” (Table 1). The score range achieved during this duty was started from “4 to 7” and the scores of 70% of the orthotists were in the range of “8 to 10”.
The present study indicated the same levels of risk for men and women in the analysis of different participant’s work postures using the REBA method. Therefore, the average REBA scores acquired from the tasks in the orthotic section did not significantly differ between men and women. These findings are contradicting the research findings about the ergonomic analysis of work postures and the work-related MSDs of hairdressers [15], nurses [14], emergency department personnel [6], and dentists [5], because in these results the rate of injuries was higher in women than in men.
In both orthotists and prosthetists, the highest prevalence of MSD was observed in the neck and shoulders as well as the wrists and hands. Also, among the tasks analyzed, the highest risk of injury/injuries confrontation belonged to the working postures of “casting,” “forming of the pieces with the valve wheel wrench,” and “removing the plaster from the socket using a pneumatic hammer”.
Based on the present findings, important factors that caused MSDs in orthotists and prosthetists were as follows: the poor design of tools and machines, improper workshop design in orthosis and prosthesis clinics, working in standing position for several hours, the lifting and manual handling of heavy objects (mold) without coworker, working with vibrating devices (milling machine, drill, etc), and repetitive tasks.
To improve the situation and reduce the risk of injury, it is recommended to adjust the height and angle of the work surface, reduce longtime standing and repetitive work, provide adjustable tools and machines, and utilize a coworker. Also, it is better to add an ergonomics course, service training, and refresher courses to increase the participants’ knowledge about the profession and the use of tools and devices designed or reformed/modified based on ergonomic principles to decrease the risk of MSDs [17].
This study only investigated 10 repetitive situations for each specialist, while working in the field of orthoses and prostheses is complex. Also, the results may not be generalizable because the type of equipments, the manner of arrangement, and the style of working are different in orthotic and prosthetic clinics.
5. Conclusion
Based on the findings, the rate of MSDs is high in the orthotist and prosthetist, especially in the orthotists. Thus, to reduce the MSDs, it is recommended to provide more educational and preventive strategies, such as adding an ergonomics course, service training, and refresher courses to increase the participants’ knowledge. Also, it is suggested to modify the tools based on the principles of ergonomics.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors
Authors' contributions
All authors contributed equally in preparing all parts of the research.
Conflict of interest
The authors declared no conflicts of interest
Acknowledgments
All author would link to thank Staff working in the Orthotics and Prosthetics Rehabilitation Center of the Red Crescent, the Rehabilitation Faculty of Tehran University of Medical Sciences, Kosar Orthotics and Prosthetics Center, Saba Technical Orthopedic Center (related to the University of Welfare and Rehabilitation Sciences), and the private clinics in Tehran.
References
- Saraji J, Hosseini M, Shahtaheri S, Golbabaei F, Ghasemkhani M. [Evaluation of ergonomic postures of dental professions by Rapid Entire Body Assessment (REBA), in Birjand, Iran (Persian)]. J Dent Med. 2005; 18(1):61-7. https://jdm.tums.ac.ir/browse.php?a_code=A-10-25-335&slc_lang=en&sid=1
- Vieira ER, Kumar S. Working postures: A literature review. J Occup Rehabil. 2004; 14(2):143-59. [DOI:10.1023/B:JOOR.0000018330.46029.05] [PMID]
- Gyi DE, Punchihewa HK. Development of a QFD based collaborative design approach to reduce work-related musculoskeletal disorders (MSDs). Des Princ Pract: An Int J. 2009; 3(6):209-24. [DOI:10.18848/1833-1874/CGP/v03i06/37789]
- Singh LP. Work posture assessment in forging industry: An exploratory study in India. Int J Adv Eng Technol. 2010; 1(3):358-66. https://www.technicaljournalsonline.com/ijeat/VOL%20I/IJAET%20VOL%20I%20ISSUE%20III%20OCTBER%20DECEMBER%202010/IJAET%20OCT-DEC,2010%20ARTICLE%2035.pdf
- Yaghobee S, Esmaeili V. [Evaluation of the effect of the ergonomic principles’ instructions on the dental students’ postures an ergonomic assessment (Persian)]. J Dent Med. 2010; 23(2):121-7. http://jdm.tums.ac.ir/article-1-104-en.html
- Hosseini M, Varmazyar S, Safari A. [A study of the physical status of emergency wards’ personnel in hospitals affiliated to Qazvin University of Medical Sciences through REBA (Rapid Entire Body Assessment) method and its relation with muscular and skeletal disorders in Qazvin, Iran (Persian)]. Qom Univ Med Sci J. 2009; 3(4):32-9. http://journal.muq.ac.ir/article-1-47-en.html
- Salmani Nodooshan H, Koohi Booshehri S, Daneshmandi H, Choobineh AR. Ergonomic workplace assessment in orthotic and prosthetic workshops. Work. 2016; 55(2):463-70. [DOI:10.3233/WOR-162401] [PMID]
- Crawford JO. The Nordic Musculoskeletal questionnaire. Occup Med. 2007; 57(4):300-1. [DOI:10.1093/occmed/kqm036]
- Namnik N, Negahban H, Salehi R, Shafizadeh R, Tabib MS. Validity and reliability of Persian version of the Specific Nordic questionnaire in Iranian industrial workers. Work. 2016; 54(1):35-41. [DOI:10.3233/WOR-162268] [PMID]
- Hignett S, McAtamney L. Rapid Entire Body Assessment (REBA). Appl Ergon. 2000; 31(2):201-5. [DOI:10.1016/S0003-6870(99)00039-3]
- Hita-Gutiérrez M, Gómez-Galán M, Díaz-Pérez M, Callejón-Ferre ÁJ. An overview of REBA method applications in the world. Int J Environ Res Public Health. 2020; 17(8):2635. [DOI:10.3390/ijerph17082635] [PMID] [PMCID]
- Schwartz AH, Albin TJ, Gerberich SG. Intra-rater and inter-rater reliability of the Rapid Entire Body Assessment (REBA) tool. Int J Ind Ergon. 2019; 71:111-6. [DOI:10.1016/j.ergon.2019.02.010]
- Madani D, Dababneh A. Rapid entire body assessment: A literature review. Am J Eng Appl Sci. 2016; 9(1):107-18. [DOI:10.3844/ajeassp.2016.107.118]
- Nakhaei M, Farag Zadeh Z, Tabiei S, Saadatjoo S, Mahmoodi Rad G, Hoseini M. [Evaluation of ergonomic position during work in nurses of medical and surgical wards in Birjand University of Medical Sciences Hospitals (Persian)]. Birjand Univ Med Sci. 2006; 13(2):9-15. http://journal.bums.ac.ir/article-1-93-en.html
- Hokmabadi R, Esmailzade Kavaki M, Mahdinia M. Evaluation of ergonomic postures of hairdressers by rapid entire body assessment. J North Khorasan Univ Med Sci. 2012; 3(4):49-54. [DOI:10.29252/jnkums.3.4.49]
- Kahyani Z, Karimi M, Amiri M, Mosharaf S, Rouhi Boroujeni H. Determination of risk factors for musculoskeletal disorders and corrective priorities to perform the work in dental careers by posture analysis using REBA in Shahrekord. Int J Epidemiol Res. 2019; 6. [DOI:10.15171/ijer.2019.17]
- Habibi E, Poorabdian S, Ahmadinejad P, Hassanzadeh A. [Ergonomic risk assessment by REBA method (Persian)]. Iran Occup Health J. 2007; 4(3-4):35-43. http://ioh.iums.ac.ir/article-1-107-en.html
Type of Study: Research |
Subject:
Prosthetics and Orthotics
Received: 2020/10/10 | Accepted: 2020/11/17 | Published: 2020/12/30
Received: 2020/10/10 | Accepted: 2020/11/17 | Published: 2020/12/30
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.