

Volume 3, Issue 1 (Continuously Updated 2020)
Func Disabil J 2020, 3(1): 161-168 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asgari S, Ebrahimi Takamjani E, Salehi R, Mansour Sohani S, Abolghasemi G. The Effect of Cognitive Task on Postural Control Dynamic Regularity of Athletes With Chronic Ankle Instability When Standing on an Unstable Surface. Func Disabil J 2020; 3 (1) :161-168
URL: http://fdj.iums.ac.ir/article-1-136-en.html
URL: http://fdj.iums.ac.ir/article-1-136-en.html
Shahab Asgari1 

 , Esmaeel Ebrahimi Takamjani *1 , Reza Salehi2 , Soheil Mansour Sohani1 , Ghadir Abolghasemi1
, Esmaeel Ebrahimi Takamjani *1 , Reza Salehi2 , Soheil Mansour Sohani1 , Ghadir Abolghasemi1
, Esmaeel Ebrahimi Takamjani *1 , Reza Salehi2 , Soheil Mansour Sohani1 , Ghadir Abolghasemi1
1- Department of Physiotherapy, Iranian Center of Excellence in Physiotherapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department Rehabilitation Management, Iranian Centre of Excellence in Physiotherapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
2- Department Rehabilitation Management, Iranian Centre of Excellence in Physiotherapy, School of Rehabilitation Sciences, Iran University of Medical Sciences, Tehran, Iran.
Keywords: Chronic ankle instability, Postural control, Nonlinear dynamic, Dual-task cognitive, Athletes
Full-Text [PDF 1062 kb]
(675 Downloads)
| Abstract (HTML) (1574 Views)
Full-Text: (634 Views)
1. Introduction
One of the most common musculoskeletal injuries is lateral ankle sprains, leading to long-term problems in the ankle and lower limbs in people [1]. Many of these people complain of residual symptoms such as recurrent “giving way” and disability [2]. These complications are commonly known as Chronic Ankle Instability (CAI) and can affect their daily, functional, and athletic activities. Mechanical instability and functional ankle instability are two significant types of CAI [3].
Studies support postural control impairments in people with CAI [4]. Researchers have noticed the loss of sensory input from articular mechanoreceptors, mechanical instability of the ankle joint, lower muscle strength and endurance, and different ankle range of motion as influencing factors in postural control impairment [5, 6].
Postural control may be an automatic process that needs minimal cognitive attention. However, recent evidence suggests that postural control necessities some attention even in healthy individuals [7, 8]. Recent research has categorized postural control from simpler to more complex tasks requiring attention processes [9, 10]. This attentional need varies depending on the type of postural activity, age, balancing abilities, and the type of cognitive task [7, 8].
However, because of the contradictory results, the relationship between postural control and cognition has remained ill-defined. Studies on young adults have reported higher [11, 12], untroubled [8], and lower [13] postural sway during concurrent cognitive tasks.
There are many situations in everyday life where one has to perform multiple tasks simultaneously—for example, walking and talking simultaneously or crossing the street and paying attention to cars crossing the street. Therefore, the evaluation of dual assignments has more external validity. Various investigations of postural control behavior have been investigated from the aspect of nonlinear dynamics and sample entropy analysis of the Center of Pressure (CoP). As an indicator, the irregularity and regularity of the CoP indicate the degree of automaticity of this behavior [14-16]. They attributed the greater irregularity of the CoP to the decrease in the amount of attention devoted to the posture. They suggested that an increase in irregularity might be considered as an increase in the automation or efficiency of posture control [17].
Therefore, examining the dynamic structure of postural sway in terms of the output signal regularity can provide important information about the health status, stability, and adaptability of the postural control system, which is impossible using linear analysis methods. This study aimed to investigate the CoP regularity between athletes with CAI and healthy subjects in unstable postural conditions.
2. Materials and Methods
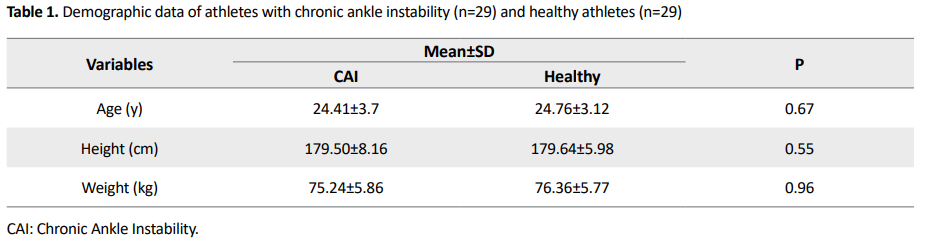
The research and its stages have been approved by the Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.FMD.REC1396.9411452003). A total of 29 subjects with a history of CAI (ages ranging from 18 to 36) and 29 healthy-matched subjects voluntarily participated in this study. All participants signed an informed consent form. We considered recreationally active as partaking in at least 20 minutes of physical activity 3 times per week. The study samples were volleyball and basketball players. Age, body mass index, height, type and duration of physical activity, and lower-limb dominance were the matching variables.
According to the International Ankle Consortium, the inclusion criteria for the people with CAI were as follows: having a history of at least 1 significant ankle sprain, the previously injured ankle joint “giving way”, and or recurrent sprain, and or “feelings of instability”. A general self-reported foot and ankle function questionnaire was used to describe the level of disability of the cohort.
We used a health questionnaire to ensure that participants had no injury or condition that could affect their balance. Individuals for the control group were excluded if they reported a history of ankle sprain or perception of “giving way” in the ankle. The information was gathered by a trained physical therapist using self-report questionnaire and clinical examination.
Postural sway was evaluated by a force plate at 2 different conditions: double-leg standing on the force platform, single-leg standing on the injured limb. All conditions were similar, while a cognitive task was performed concurrently. Subjects stood barefoot with their arms hanging at their sides. Foot placement on the force plate was constant in all tests. They were not allowed to move their limbs or head or talk during the data collection period. The dominant limb was the limb used in at least 2 out of the 3 following tests: stepping up onto a box, recovering balance after a posterior push, and kicking a ball with maximum accuracy through a goal.
Postural task (single task)
The postural task was done as still as possible on the wobble board on the force plate with feet separated and arms hanging loosely at the sides, and eyes fixed on an eye-level target 3 m ahead. During single-leg standing, the subjects were asked to stand as still as possible and to concentrate on a visual target 3 m away in front of them.
Cognitive task
For the cognitive task, the participants were asked to do silent digit backward counting by 7, starting from a random number, for instance, between 400 and 500. They were asked to do correctly as possible. Immediately after the collection of the postural data, the subjects were required to tell the number they had reached.
Three trials with a 1-min rest between each test were performed. To minimize the learning effect, the postural and cognitive tasks were randomized for each participant before starting the measurements. The whole experiment lasted approximately 60 min. CoP data were obtained using a Kistler, 92260 AA6 force platform with a sampling frequency of 100 Hz.
Statistical analysis
The obtained data were analyzed in SPSS version 20. Before the statistical analysis, the normal distribution of the data was evaluated by the Shapiro-Wilk test. The data for each postural stability index were analyzed by a 2-by-2 (group by cognitive difficulty) mixed-model Analysis of Variance (ANOVA). It was used to determine the interactions and main effects of the 2 factors. Comparisons between the 2 groups were made with the Independent t-test.
3. Results
The Independent t test was used to compare the demographic data between groups. There was no significant difference between the two groups (Table 1).
Postural performance for the single-leg standing condition
In both AP and ML directions, there was no main effect of group on entropy (AP: F1=0.02, P>0.05; ML: F1=1, P>0.05). In both AP and ML directions, there was a main effect of condition (AP: F1=0.14, P<0.001; ML: F1=0.91, P<0.001). The group × cognitive interaction, (F=0.41, P>0.05=0.037) was not statistically significant in the ML direction (Figure 1 & 2). Also, in the AP direction, (F1=22.55, P<0.001) the results were not statistically significant (Table 2).
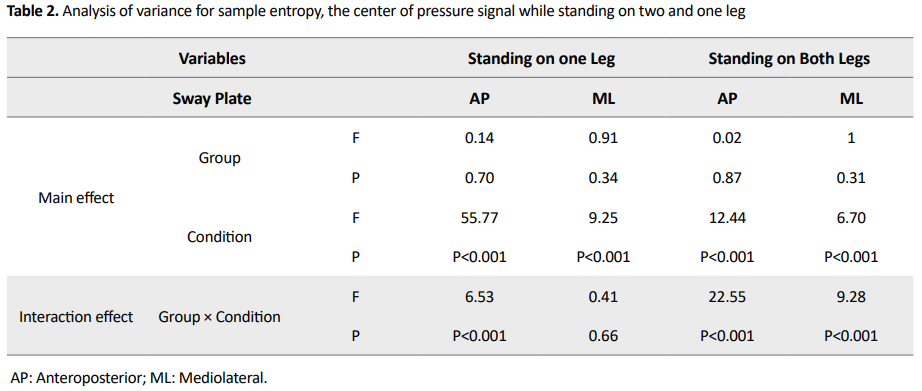

According to Table 2 and comparison between the two groups, there was a significant difference between the two groups in the cognitive task and the single task in the anterior-posterior direction while standing on both legs.
Postural performance for the double standing condition
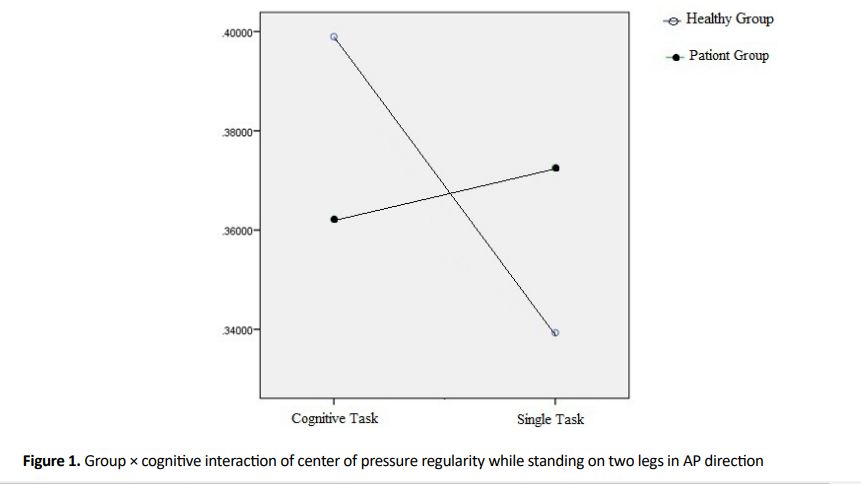
In both AP and ML directions, there was no main effect of group on entropy (AP: F1=0.02, P>0.05; ML: F1=1, P>0.05). In both AP and ML directions, there was a main effect of condition (AP: F1=12.44, P<0.001; ML: F1=6.70, P<0.001). The group × cognitive interaction, (AP: F1=22.55, P<0.001; ML: F1=6.53, P<0.001), was statistically significant in both AP and ML directions (Table 2).
4. Discussion
The present study investigated the effect of dual cognitive task on postural control behavior based on the CoP signal regularity while standing on an unstable surface in athletes with CAI. The purpose of the present study was to determine whether adding a dual cognitive task to the postural task while standing on an unstable surface could cause changes in the pressure center signal irregularity.
The results of the present study showed that when standing on the wobble board while performing postural and cognitive dual tasks in the healthy group, the CoP irregularity was significantly higher than the patient group. In other words, when adding cognitive task to postural task, healthy subjects will show less predict postural control behavior. Donker et al. suggested increasing regularity signal order implies that postural control behaviors become rigid and attitudinal dependency is attenuated [17]. From the linear dynamics of postural control behavior in the present study, it was observed that CoP displacement in dual cognitive tasks was significantly increased in patients with a chronic ankle sprain. Therefore, in healthy subjects, with increasing irregularity and decreasing CoP displacement, healthy subjects have used more effective postural exploratory behavior in unstable postural conditions than those with CAI. However, the inability to use postural exploratory behavior in subjects with CAI results in increased postural sway in this unstable postural condition [18]. In this state, since insufficient information is provided, the postural control will be conscious of the postural stability [19].
According to Roerdink et al., a decrease in the CoP signal regularity result in distraction attention from postural control, leading to more automatic postural control behavior [18]. Polskaia et al. showed that distracting attention from postural control when performing dual tasks ensued by less interference with the automated motor control process and, consequently, better individual performance [20]. Increasing the CoP signal irregularity indicates more complexity of the system, which results in more automatic postural control. More complexity in postural control will lead to greater adaptation to postural perturbation environmental changes [17].
Terada et al. concluded that while standing on a stable surface, individuals with chronic ankle sprains are less entropic than healthy individuals. They correlated the decrease in CoP signal irregularity with greater postural control rigidity and reduced adaptability in the affected group [1].
Since the subjects should not be talking during the dual postural and cognitive task, the examiner could not check the consistency and accuracy of the counting-backward during the test. Therefore, it is recommended that future studies use the cognitive task that can be used to evaluate its continuity during dual-task. As one of the causes of falls in the elderly is a decrease in postural adaptability, it is recommended that future studies consider the elderly group and other postural disorder groups.
5. Conclusion
In unstable postural conditions, the center of the pressure signal regularity increases in subjects with CAI compared to the healthy group, indicating attentional-dependent behavior and decreased postural control adaptability. Dual tasks in healthy individuals increase the irregularity in the CoP signal and lead to automatic control. This pattern is not seen in individuals with CAI.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
References
One of the most common musculoskeletal injuries is lateral ankle sprains, leading to long-term problems in the ankle and lower limbs in people [1]. Many of these people complain of residual symptoms such as recurrent “giving way” and disability [2]. These complications are commonly known as Chronic Ankle Instability (CAI) and can affect their daily, functional, and athletic activities. Mechanical instability and functional ankle instability are two significant types of CAI [3].
Studies support postural control impairments in people with CAI [4]. Researchers have noticed the loss of sensory input from articular mechanoreceptors, mechanical instability of the ankle joint, lower muscle strength and endurance, and different ankle range of motion as influencing factors in postural control impairment [5, 6].
Postural control may be an automatic process that needs minimal cognitive attention. However, recent evidence suggests that postural control necessities some attention even in healthy individuals [7, 8]. Recent research has categorized postural control from simpler to more complex tasks requiring attention processes [9, 10]. This attentional need varies depending on the type of postural activity, age, balancing abilities, and the type of cognitive task [7, 8].
However, because of the contradictory results, the relationship between postural control and cognition has remained ill-defined. Studies on young adults have reported higher [11, 12], untroubled [8], and lower [13] postural sway during concurrent cognitive tasks.
There are many situations in everyday life where one has to perform multiple tasks simultaneously—for example, walking and talking simultaneously or crossing the street and paying attention to cars crossing the street. Therefore, the evaluation of dual assignments has more external validity. Various investigations of postural control behavior have been investigated from the aspect of nonlinear dynamics and sample entropy analysis of the Center of Pressure (CoP). As an indicator, the irregularity and regularity of the CoP indicate the degree of automaticity of this behavior [14-16]. They attributed the greater irregularity of the CoP to the decrease in the amount of attention devoted to the posture. They suggested that an increase in irregularity might be considered as an increase in the automation or efficiency of posture control [17].
Therefore, examining the dynamic structure of postural sway in terms of the output signal regularity can provide important information about the health status, stability, and adaptability of the postural control system, which is impossible using linear analysis methods. This study aimed to investigate the CoP regularity between athletes with CAI and healthy subjects in unstable postural conditions.
2. Materials and Methods
The research and its stages have been approved by the Ethics Committee of Iran University of Medical Sciences (Code: IR.IUMS.FMD.REC1396.9411452003). A total of 29 subjects with a history of CAI (ages ranging from 18 to 36) and 29 healthy-matched subjects voluntarily participated in this study. All participants signed an informed consent form. We considered recreationally active as partaking in at least 20 minutes of physical activity 3 times per week. The study samples were volleyball and basketball players. Age, body mass index, height, type and duration of physical activity, and lower-limb dominance were the matching variables.
According to the International Ankle Consortium, the inclusion criteria for the people with CAI were as follows: having a history of at least 1 significant ankle sprain, the previously injured ankle joint “giving way”, and or recurrent sprain, and or “feelings of instability”. A general self-reported foot and ankle function questionnaire was used to describe the level of disability of the cohort.
We used a health questionnaire to ensure that participants had no injury or condition that could affect their balance. Individuals for the control group were excluded if they reported a history of ankle sprain or perception of “giving way” in the ankle. The information was gathered by a trained physical therapist using self-report questionnaire and clinical examination.
Postural sway was evaluated by a force plate at 2 different conditions: double-leg standing on the force platform, single-leg standing on the injured limb. All conditions were similar, while a cognitive task was performed concurrently. Subjects stood barefoot with their arms hanging at their sides. Foot placement on the force plate was constant in all tests. They were not allowed to move their limbs or head or talk during the data collection period. The dominant limb was the limb used in at least 2 out of the 3 following tests: stepping up onto a box, recovering balance after a posterior push, and kicking a ball with maximum accuracy through a goal.
Postural task (single task)
The postural task was done as still as possible on the wobble board on the force plate with feet separated and arms hanging loosely at the sides, and eyes fixed on an eye-level target 3 m ahead. During single-leg standing, the subjects were asked to stand as still as possible and to concentrate on a visual target 3 m away in front of them.
Cognitive task
For the cognitive task, the participants were asked to do silent digit backward counting by 7, starting from a random number, for instance, between 400 and 500. They were asked to do correctly as possible. Immediately after the collection of the postural data, the subjects were required to tell the number they had reached.
Three trials with a 1-min rest between each test were performed. To minimize the learning effect, the postural and cognitive tasks were randomized for each participant before starting the measurements. The whole experiment lasted approximately 60 min. CoP data were obtained using a Kistler, 92260 AA6 force platform with a sampling frequency of 100 Hz.
Statistical analysis
The obtained data were analyzed in SPSS version 20. Before the statistical analysis, the normal distribution of the data was evaluated by the Shapiro-Wilk test. The data for each postural stability index were analyzed by a 2-by-2 (group by cognitive difficulty) mixed-model Analysis of Variance (ANOVA). It was used to determine the interactions and main effects of the 2 factors. Comparisons between the 2 groups were made with the Independent t-test.
3. Results
The Independent t test was used to compare the demographic data between groups. There was no significant difference between the two groups (Table 1).
Postural performance for the single-leg standing condition
In both AP and ML directions, there was no main effect of group on entropy (AP: F1=0.02, P>0.05; ML: F1=1, P>0.05). In both AP and ML directions, there was a main effect of condition (AP: F1=0.14, P<0.001; ML: F1=0.91, P<0.001). The group × cognitive interaction, (F=0.41, P>0.05=0.037) was not statistically significant in the ML direction (Figure 1 & 2). Also, in the AP direction, (F1=22.55, P<0.001) the results were not statistically significant (Table 2).
According to Table 2 and comparison between the two groups, there was a significant difference between the two groups in the cognitive task and the single task in the anterior-posterior direction while standing on both legs.
Postural performance for the double standing condition
In both AP and ML directions, there was no main effect of group on entropy (AP: F1=0.02, P>0.05; ML: F1=1, P>0.05). In both AP and ML directions, there was a main effect of condition (AP: F1=12.44, P<0.001; ML: F1=6.70, P<0.001). The group × cognitive interaction, (AP: F1=22.55, P<0.001; ML: F1=6.53, P<0.001), was statistically significant in both AP and ML directions (Table 2).
4. Discussion
The present study investigated the effect of dual cognitive task on postural control behavior based on the CoP signal regularity while standing on an unstable surface in athletes with CAI. The purpose of the present study was to determine whether adding a dual cognitive task to the postural task while standing on an unstable surface could cause changes in the pressure center signal irregularity.
The results of the present study showed that when standing on the wobble board while performing postural and cognitive dual tasks in the healthy group, the CoP irregularity was significantly higher than the patient group. In other words, when adding cognitive task to postural task, healthy subjects will show less predict postural control behavior. Donker et al. suggested increasing regularity signal order implies that postural control behaviors become rigid and attitudinal dependency is attenuated [17]. From the linear dynamics of postural control behavior in the present study, it was observed that CoP displacement in dual cognitive tasks was significantly increased in patients with a chronic ankle sprain. Therefore, in healthy subjects, with increasing irregularity and decreasing CoP displacement, healthy subjects have used more effective postural exploratory behavior in unstable postural conditions than those with CAI. However, the inability to use postural exploratory behavior in subjects with CAI results in increased postural sway in this unstable postural condition [18]. In this state, since insufficient information is provided, the postural control will be conscious of the postural stability [19].
According to Roerdink et al., a decrease in the CoP signal regularity result in distraction attention from postural control, leading to more automatic postural control behavior [18]. Polskaia et al. showed that distracting attention from postural control when performing dual tasks ensued by less interference with the automated motor control process and, consequently, better individual performance [20]. Increasing the CoP signal irregularity indicates more complexity of the system, which results in more automatic postural control. More complexity in postural control will lead to greater adaptation to postural perturbation environmental changes [17].
Terada et al. concluded that while standing on a stable surface, individuals with chronic ankle sprains are less entropic than healthy individuals. They correlated the decrease in CoP signal irregularity with greater postural control rigidity and reduced adaptability in the affected group [1].
Since the subjects should not be talking during the dual postural and cognitive task, the examiner could not check the consistency and accuracy of the counting-backward during the test. Therefore, it is recommended that future studies use the cognitive task that can be used to evaluate its continuity during dual-task. As one of the causes of falls in the elderly is a decrease in postural adaptability, it is recommended that future studies consider the elderly group and other postural disorder groups.
5. Conclusion
In unstable postural conditions, the center of the pressure signal regularity increases in subjects with CAI compared to the healthy group, indicating attentional-dependent behavior and decreased postural control adaptability. Dual tasks in healthy individuals increase the irregularity in the CoP signal and lead to automatic control. This pattern is not seen in individuals with CAI.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
References
- Terada M, Beard M, Carey S, Pfile K, Pietrosimone B, Rullestad E, et al. Nonlinear dynamic measures for evaluating postural control in individuals with and without chronic ankle instability. Motor Control. 2019; 23(2):243-61. [DOI:10.1123/mc.2017-0001] [PMID]
- Anandacoomarasamy A, Barnsley L. Long term outcomes of inversion ankle injuries. Br J Sports Med. 2005; 39(3):e14. [DOI:10.1136/bjsm.2004.011676] [PMID] [PMCID]
- Gribble PA, Delahunt E, Bleakley C, Caulfield B, Docherty C, Fourchet F, et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J Orthop Sports Phys Ther. 2013; 43(8):585-91. [DOI:10.1136/bjsports-2013-093175] [PMID]
- de Noronha M, Refshauge KM, Herbert RD, Kilbreath SL. Do voluntary strength, proprioception, range of motion, or postural sway predict occurrence of lateral ankle sprain? Br J Sports Med. 2006; 40(10):824-8. [DOI:10.1136/bjsm.2006.029645] [PMID] [PMCID]
- Freeman, M. Instability of the foot affer injuries to the lateral ligament of the ankle. Bone Joint J, 1965; 47(4):669-77. [DOI:10.1302/0301-620X.47B4.669]
- Riemann BL. Is there a link between chronic ankle instability and postural instability? J Athl Train. 2002; 37(4):386-93. [PMCID] [PMID]
- Shumway-Cook A, Woollacott M. Attentional demands and postural control: the effect of sensory context. J Gerontol A Biol Sci Med Sci. 2000; 55(1):M10. [DOI:10.1093/gerona/55.1.M10] [PMID]
- Yardley L, Gardner M, Leadbetter A, Lavie N. Effect of articulatory and mental tasks on postural control. Neuroreport. 1999; 10(2):215-9. [DOI:10.1097/00001756-199902050-00003] [PMID]
- Vuillerme N, Nougier V. Attentional demand for regulating postural sway: the effect of expertise in gymnastics. Brain Res Bull. 2004; 63(2):161-5. [DOI:10.1016/j.brainresbull.2004.02.006] [PMID]
- Woollacott M, Shumway-Cook A. Attention and the control of posture and gait: A review of an emerging area of research. Gait posture. 2002; 16(1):1-14. [DOI:10.1016/S0966-6362(01)00156-4]
- Pellecchia GL. Postural sway increases with attentional demands of concurrent cognitive task. Gait Posture, 2003; 18(1):29-34. [DOI:10.1016/S0966-6362(02)00138-8]
- Teasdale N, Bard C, LaRue J, Fleury M. On the cognitive penetrability of posture control. Exp Aging Res. 1993; 19(1):1-13. [DOI:10.1080/03610739308253919] [PMID]
- Andersson G, Hagman J, Talianzadeh R, Svedberg A, Larsen, HC. Effect of cognitive load on postural control. Brain Res Bull. 2002; 58(1):135-9. [DOI:10.1016/S0361-9230(02)00770-0]
- Cavanaugh JT, Mercer VS, Stergiou N.Approximate entropy detects the effect of a secondary cognitive task on postural control in healthy young adults: A methodological report. J Neuroeng Rehabil. 2007; 4(1):42. [DOI:10.1186/1743-0003-4-42] [PMID] [PMCID]
- Ladislao L, Rabini RA, Ghetti G, Fioretti S. Approximate entropy on posturographic data of diabetic subjects with peripheral neuropathy. Gait Posture. 2008; (28):S6-S7. [DOI:10.1016/j.gaitpost.2007.12.018]
- Santarcangelo EL, Scattina E, Carli G, Balocchi R, Macerata A, Manzoni D. Modulation of the postural effects of cognitive load by hypnotizability. Exp Brain Res. 2009; 194(2):323-8. [DOI:10.1007/s00221-009-1740-6] [PMID]
- Donker SF, Roerdink M, Greven AJ, Beek PJ. Regularity of center-of-pressure trajectories depends on the amount of attention invested in postural control. Exp Brain Res. 2007; 181(1):1-11. [DOI:10.1007/s00221-007-0905-4] [PMID] [PMCID]
- Roerdink M, De Haart M, Daffertshofer A, Donker SF, Geurts ACH, Beek PJ. Dynamical structure of center-of-pressure trajectories in patients recovering from stroke. Exp Brain Res. 2006; 174(2):256. [DOI:10.1007/s00221-006-0441-7] [PMID]
- Zhang W, Schwenk M, Mellone S, Paraschiv-Ionescu A, Vereijken B, Pijnappels M, et al. Complexity of daily physical activity is more sensitive than conventional metrics to assess functional change in younger older adults. Sensors. 2018; 18(7):2032. [DOI:10.3390/s18072032] [PMID] [PMCID]
Type of Study: Letter to the Editor |
Subject:
Physiotherapy
Received: 2020/10/27 | Accepted: 2020/12/3 | Published: 2020/12/30
Received: 2020/10/27 | Accepted: 2020/12/3 | Published: 2020/12/30
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.