

Volume 3, Issue 1 (Continuously Updated 2020)
Func Disabil J 2020, 3(1): 83-90 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tavana H, Rouzbahani M, Sameni S J, Maarefvand M. Examination of Speech Signals’ Intensity Reconstruction Through Evaluation of the Frequency Responses of Behind-the-ear Hearing Aids Fitted With NAL-NL2 and DSLi/o v5 Prescription Formulas. Func Disabil J 2020; 3 (1) :83-90
URL: http://fdj.iums.ac.ir/article-1-129-en.html
URL: http://fdj.iums.ac.ir/article-1-129-en.html


1- Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Science, Tehran, Iran.
2- Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Science, Tehran, Iran. ,rouzbahani.m@iums.ac.ir
2- Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Science, Tehran, Iran. ,
Full-Text [PDF 1319 kb]
(689 Downloads)
| Abstract (HTML) (1580 Views)
Full-Text: (672 Views)
1. Introduction
Congenital hearing loss (hearing loss that is present at birth) is one of the most prevalent chronic conditions in newborns [1]. Normal hearing abilities are essential for the acquisition and development of language and speech skills [2]. Hence, suffering from hearing loss in such a critical period while being deprived of early rehabilitation interventions leave extremely destructive impacts on the language and speech skills of children with hearing impairments [3]. Since hearing aids are the most commonly used devices to help with auditory rehabilitation, they must incorporate suitable electro-acoustic properties to reconstruct the spoken sounds [4]. The initial purpose of a proper amplification is to create a signal perceptible in all speech frequency ranges, which is specifically essential for hearing impaired children and infants due to their special amplification needs [5] .
The wide bandwidth of frequency response in hearing aids can result in perceptual benefits, but the entire bandwidth has no similar effect in sound perception [6], and the hearing aid’s gain usually declines at the extremity of the frequency response range [4]. However, hearing aids are still inadequate in providing sufficient amplification at the favorable frequency bandwidth despite the recent advancements [7]. Therefore, it appears that the question of whether or not these hearing aids are capable of providing adequate hearing gain for all speech sounds, specifically those with high-frequency speech stimuli, requires further examination.
The majority of the previously conducted studies have examined the intensity parameters needed for providing maximum speech clarity and have tried to find which properties are required to reach this end, but few pieces of research have addressed hearing aids as the primary tools in the reconstruction and provision of these required intensity parameters.
On the other hand, the selection of a hearing aid capable of reconstructing the essential and required electroacoustic parameters without effective limitations gains a high gravity following acoustic dynamics loss in the cochlea [8]. A 2010 study conducted by Holube et al. aiming to compare various stimuli used to assess and validate hearing aids revealed that because speech is the most significant stimulus in the everyday life of hearing aid users and it is different from other stimuli in terms of spectrum, intensity, and other acoustic properties [9], it would be better to use speech stimuli to validate the proper performance of hearing aids and examine different aspects of their capabilities. For this purpose, a stimulus able to eliminate linguistic differences would be efficient. A 2001 study by Stelmachowicz et al. suggested the hypothesis that hearing aid’s incapability of complete reconstruction of speech sounds might be responsible for the low speech clarity of children with hearing impairments [5]. Subsequently, many studies were conducted addressing suitable acoustic parameters for reconstructing speech sounds, but the question of whether or not the prescribed hearing aids incorporate these parameters still requires further investigations. The purpose of this study was to examine how capable hearing aids gain the required intensity properties given the existing limitations.
2. Materials and methods
The present applied research is an observational, descriptive-analytical study and a subset of cross-sectional-comparative studies. In order to test the consistency of outcomes, two Phonak Bolero B50 BTE hearing aids were selected. These two hearing aids were fitted with NAL-NL2 and DSLi/o v5 prescription formulas for both mild to moderately severe and moderately severe to severe hearing losses. Then, the amount of gain was measured across frequencies from 200 to 8000 HZ for input levels of 50, 65, and 80 dB SPL. There were three repetitions for the measurement at each level. The total number of trials was 72 (2 hearing aids×2 types of hearing losses×2 types of fitting formulas×3 input levels×3 repetitions).
The International Speech Test Signal (ISTS) stimulus used in the study was a 60-seconds recorded speech stimulus of a female speaker speaking with a combination of 6 living languages of the world (American English, Chinese, French, German, Arabic, and Spanish), with no meaning and therefore, capable of eliminating linguistic effects and simulating the acoustic characteristics of speech.
The ISTS speech stimulus was intensity-filtered using Adobe Audition v. 12.1.3.10 –a 2019 Adobe product- to cover two degrees of hearing loss (mild to moderately severe and moderately severe to severe). The extent of stimulus intensity reduction was in proportion to the audiogram required to reduce various frequency contents.
In the next step, the selected hearing aid was fitted in conformity with the aforementioned two degrees of hearing loss using the respective fitting software. The NAL-NL2 or DSLi/o v5 prescription formulas were used to fit the hearing aid. The hearing aid was then exposed to the filtered stimuli in three input intensities, and the output generated by the hearing aid was analyzed using the FRYE FP35 analyzer device. Eventually, the frequency response, the output gain of the filtered stimulus, and the amounts reduced by intensity filtration were compared.
The NAL-NL2 formula does not attempt to restore normal loudness at each frequency. The underlying rationale is to maximize speech intelligibility, subject to the overall loudness of speech at any level being no more than that perceived by a normal-hearing person [10].
One of the most popular loudness normalization procedures is DSLi/o v5 (desired sensation level input/output). The rationale of DSLi/o v5 is to adjust the hearing instrument parameters so that the acoustic dynamic range of a normally hearing person is compressed into the residual dynamic range of the hearing-impaired person to be fitted. The objective is to make all sounds audible to the hearing impaired user at the same loudness as they would be to the normally hearing person [6, 11].
Data analysis was conducted using IBM SPSS softwa v. 25 at a significance level of 0.05. Indices of central tendency (mean) and indices of dispersion (minimum, maximum, and standard deviation) were used in the descriptive statistics section. In the analytical statistics section, Kolmogorov-Smirnov and Generalized Linear Model (GLM) tests were conducted to examine the distribution of data and to analyze the differences between the groups, respectively. Tuckey’s test for post hoc analysis was also conducted to follow up the significant differences.
3. Results
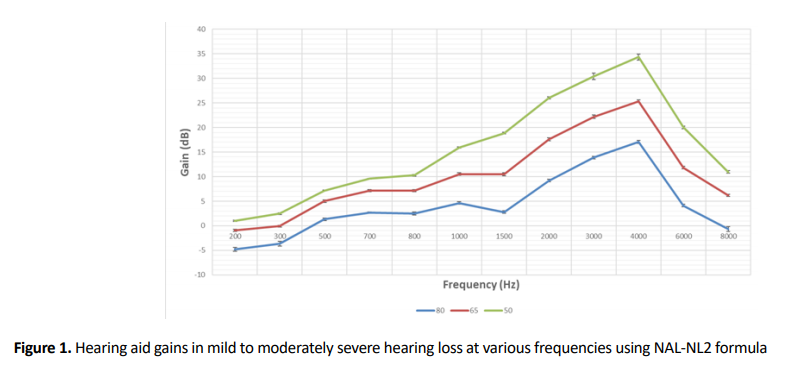
As indicated in Figure 1, for hearing aids fitted with the NAL-NL2 formula for mild to moderately severe hearing loss degrees in three input intensities of 50, 65, and 80 dB SPL, the highest gain was at the frequency of 4000 Hz (P=0.001) and the lowest gain was at the frequency of 200 Hz (P=0.004).
As indicated in Figure 2, for hearing aids fitted with the NAL-NL2 formula for moderately severe to severe hearing loss at 50 dB SPL input intensity level, the highest gain was at the frequency of 3000 Hz (P=0.002) and the lowest gain was at the frequency of 200 Hz (P=0.003), while the highest gain was at 4,000 Hz frequency (P=0.002) and the lowest gain was in 200 Hz frequency (P=0.003) at 65 and 80 dB SPL intensity input levels.
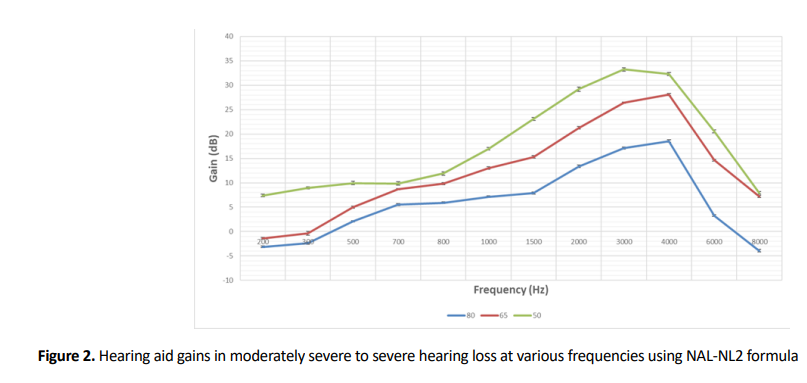
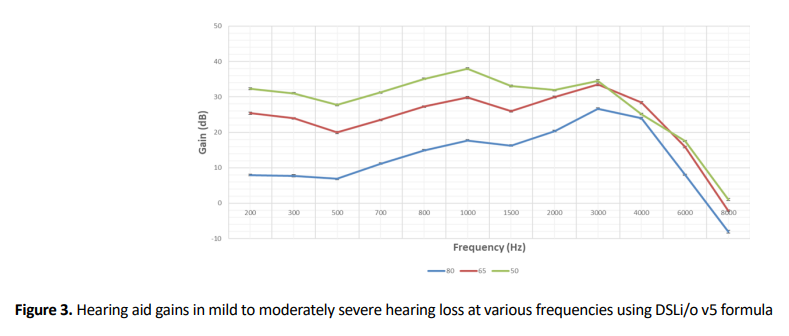
Figure 3 indicates that the highest gain was at the frequency of 1000 Hz (P=0.007) and the lowest gain was at the frequency of 8000 Hz (P=0.005) for hearing aids fitted with DSLi/o v5 formula for mild to moderately severe hearing loss at 50 dB SPL input intensity level, while the highest gain was at 3000 Hz frequency (P=0.006) and the lowest gain was at 8000 Hz frequency (P=0.002) at 65 and 80 dB SPL intensity input levels.
As Figure 4 illustrates, the highest gain was at the frequency of 1000 Hz (P=0.003) and the lowest gain was at the frequency of 8000 Hz (P=0.001) for hearing aids fitted with DSLi/o v5 formula for moderately severe to severe hearing loss at 50, 65, and 80 dB SPL input intensity levels.

Using hearing aids fitted with NAL-NL2 formula at 50 dB SPL input intensity level, the highest gain was at the frequency of 4000 Hz (P=0.005) and the lowest gain was at the frequency of 200 Hz (P=0.002) for mild to moderately severe hearing loss, while the highest gain was at 3000 Hz frequency (P=0.007) and the lowest gain was at 200 Hz frequency (P=0.003) for moderately severe to severe hearing loss. Using DSLi/o v5 obtained the highest gain at 1000 Hz frequency (P=0.001) and the lowest gain at 8000 Hz frequency (P=0.004) for both mild to moderately severe and moderately severe to severe hearing loss degrees. In general, the DSLi/o v5 formula exerts higher average gains at both hearing loss degrees.
The highest gain was at the frequency of 4000 Hz (P=0.008) and the lowest gain was at the frequency of 200 Hz (P=0.006) for hearing aids fitted with the NAL-NL2 formula for both mild to moderately severe and moderately severe to severe hearing loss degrees at 65 dB SPL input intensity. Using the DSLi/o v5 formula for mild to moderately severe hearing loss, the highest gain was observed at 3000 Hz frequency (P=0.001) and the lowest gain was observed at 8000 Hz frequency (P=0.012). In general, the DSLi/o v5 formula exerts a higher average gain at both hearing loss degrees.
In both mild to moderately severe and moderately severe to severe hearing loss degrees, fitting the hearing aid with the NAL-NL2 formula at 80 dB SPL input intensity level yields the highest gain at 4000 Hz frequency (P=0.003) and the lowest gains at 200 and 8000 Hz frequency, respectively (P=0.002 and P=0.009, respectively). Using DSLi/o v5 formula exerts the highest gain at 3000 Hz frequency (P=0.002) and the lowest gain at 8000 Hz frequency (P=0.001) in mild to moderately severe hearing loss, while it exerts the highest gain at 1000 Hz frequency (P=0.001) and the lowest gain at 8000 Hz frequency (P=0.009) in moderately severe to severe hearing loss. Generally, DSLi/o v5 yields higher average gain at both hearing loss degrees.
4. Discussion
Hearing aid response modification and examination of its efficiency and usefulness are among audiological rehabilitation objectives that are practiced immediately after the hearing aid is fine-tuned and its function is validated. The validation of a hearing aid’s appropriate gain does not necessarily mean that the hearing aid is effective. The main factor contributing to the effectiveness is the hearing aid’s gain and electroacoustic parameters having an effective function in hearing. The validation of the hearing aid’s usefulness is dependent on mental, real, and verbal tests in various situations.
As indicated in other studies, non-linear hearing aids fitted with NAL-NL2 and DSLi/o v5 formulas exert different gains at 50, 65, and 80 dB SPL intensity levels. The exerted gains for the aforementioned input intensities were constantly observed to be significantly higher at 50 dB SPL compared with the other two input intensities (P=0.001). Using NAL-NL2 and DSLi/o v5 formulas for both mild to moderately severe and moderately severe to severe hearing loss degrees, the highest exerted gain was observed at the input intensity level of 50 dB SPL (P=0.002 and P=0.009, respectively) while the lowest gain was observed at 80 dB SPL (P=0.003 and P=0.007, respectively) input intensity level. This difference between the prescribed gains was significant and consistent with the findings of similar studies [12, 13, 14].
In terms of hearing loss degrees, it can be said that both NAL-NL2 and DSLi/o v5 exerted a significantly higher average gain for moderately severe to severe hearing loss compared with that of mild to moderately severe hearing loss. This difference between the prescribed gains was significant and consistent with the findings of similar studies [12, 15].
In terms of the reconstruction of filtered intensity content at 50 dB SPL input level, it can be said that DSLi/o v5 exerted a higher average gain and intensity reconstruction at both hearing loss degrees at an input intensity level of 50 dB in low and medium frequencies (P=0.001 and P=0.002, respectively). However, the two formulas indicated the same performance in high frequencies (P=0.004) and the NAL-NL2 formula might even exert higher gains for those with mild to moderately severe hearing loss at higher frequencies (P=0.014). Also, in terms of the reconstruction of filtered intensity content at 65 and 80 dB SPL input levels, it can be said that DSLi/o v5 formula revealed to exert higher gains at both hearing loss degrees (P=0.006 and P=0.002 respectively) that is consistent with the findings of other studies [13, F].
5.Conclusion
By comparing the two formulas, it can be inferred that DSLi/o v5 exerted higher average gains compared with NAL-NL2 for both hearing loss degrees and at all three input levels. Therefore, depending on the purpose of gain prescription, whether the loudness is important, or speech intelligibility, the choice of appropriate fitting formula and other specific prescription qualities can be affected.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
The paper was extracted from the MSc. thesis of the first author at Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Science, Tehran.
Authors' contributions
All authors equally contributed to preparing this article
Conflict of interest
The authors declared no conflict of interest.
Refrences:
Congenital hearing loss (hearing loss that is present at birth) is one of the most prevalent chronic conditions in newborns [1]. Normal hearing abilities are essential for the acquisition and development of language and speech skills [2]. Hence, suffering from hearing loss in such a critical period while being deprived of early rehabilitation interventions leave extremely destructive impacts on the language and speech skills of children with hearing impairments [3]. Since hearing aids are the most commonly used devices to help with auditory rehabilitation, they must incorporate suitable electro-acoustic properties to reconstruct the spoken sounds [4]. The initial purpose of a proper amplification is to create a signal perceptible in all speech frequency ranges, which is specifically essential for hearing impaired children and infants due to their special amplification needs [5] .
The wide bandwidth of frequency response in hearing aids can result in perceptual benefits, but the entire bandwidth has no similar effect in sound perception [6], and the hearing aid’s gain usually declines at the extremity of the frequency response range [4]. However, hearing aids are still inadequate in providing sufficient amplification at the favorable frequency bandwidth despite the recent advancements [7]. Therefore, it appears that the question of whether or not these hearing aids are capable of providing adequate hearing gain for all speech sounds, specifically those with high-frequency speech stimuli, requires further examination.
The majority of the previously conducted studies have examined the intensity parameters needed for providing maximum speech clarity and have tried to find which properties are required to reach this end, but few pieces of research have addressed hearing aids as the primary tools in the reconstruction and provision of these required intensity parameters.
On the other hand, the selection of a hearing aid capable of reconstructing the essential and required electroacoustic parameters without effective limitations gains a high gravity following acoustic dynamics loss in the cochlea [8]. A 2010 study conducted by Holube et al. aiming to compare various stimuli used to assess and validate hearing aids revealed that because speech is the most significant stimulus in the everyday life of hearing aid users and it is different from other stimuli in terms of spectrum, intensity, and other acoustic properties [9], it would be better to use speech stimuli to validate the proper performance of hearing aids and examine different aspects of their capabilities. For this purpose, a stimulus able to eliminate linguistic differences would be efficient. A 2001 study by Stelmachowicz et al. suggested the hypothesis that hearing aid’s incapability of complete reconstruction of speech sounds might be responsible for the low speech clarity of children with hearing impairments [5]. Subsequently, many studies were conducted addressing suitable acoustic parameters for reconstructing speech sounds, but the question of whether or not the prescribed hearing aids incorporate these parameters still requires further investigations. The purpose of this study was to examine how capable hearing aids gain the required intensity properties given the existing limitations.
2. Materials and methods
The present applied research is an observational, descriptive-analytical study and a subset of cross-sectional-comparative studies. In order to test the consistency of outcomes, two Phonak Bolero B50 BTE hearing aids were selected. These two hearing aids were fitted with NAL-NL2 and DSLi/o v5 prescription formulas for both mild to moderately severe and moderately severe to severe hearing losses. Then, the amount of gain was measured across frequencies from 200 to 8000 HZ for input levels of 50, 65, and 80 dB SPL. There were three repetitions for the measurement at each level. The total number of trials was 72 (2 hearing aids×2 types of hearing losses×2 types of fitting formulas×3 input levels×3 repetitions).
The International Speech Test Signal (ISTS) stimulus used in the study was a 60-seconds recorded speech stimulus of a female speaker speaking with a combination of 6 living languages of the world (American English, Chinese, French, German, Arabic, and Spanish), with no meaning and therefore, capable of eliminating linguistic effects and simulating the acoustic characteristics of speech.
The ISTS speech stimulus was intensity-filtered using Adobe Audition v. 12.1.3.10 –a 2019 Adobe product- to cover two degrees of hearing loss (mild to moderately severe and moderately severe to severe). The extent of stimulus intensity reduction was in proportion to the audiogram required to reduce various frequency contents.
In the next step, the selected hearing aid was fitted in conformity with the aforementioned two degrees of hearing loss using the respective fitting software. The NAL-NL2 or DSLi/o v5 prescription formulas were used to fit the hearing aid. The hearing aid was then exposed to the filtered stimuli in three input intensities, and the output generated by the hearing aid was analyzed using the FRYE FP35 analyzer device. Eventually, the frequency response, the output gain of the filtered stimulus, and the amounts reduced by intensity filtration were compared.
The NAL-NL2 formula does not attempt to restore normal loudness at each frequency. The underlying rationale is to maximize speech intelligibility, subject to the overall loudness of speech at any level being no more than that perceived by a normal-hearing person [10].
One of the most popular loudness normalization procedures is DSLi/o v5 (desired sensation level input/output). The rationale of DSLi/o v5 is to adjust the hearing instrument parameters so that the acoustic dynamic range of a normally hearing person is compressed into the residual dynamic range of the hearing-impaired person to be fitted. The objective is to make all sounds audible to the hearing impaired user at the same loudness as they would be to the normally hearing person [6, 11].
Data analysis was conducted using IBM SPSS softwa v. 25 at a significance level of 0.05. Indices of central tendency (mean) and indices of dispersion (minimum, maximum, and standard deviation) were used in the descriptive statistics section. In the analytical statistics section, Kolmogorov-Smirnov and Generalized Linear Model (GLM) tests were conducted to examine the distribution of data and to analyze the differences between the groups, respectively. Tuckey’s test for post hoc analysis was also conducted to follow up the significant differences.
3. Results
As indicated in Figure 1, for hearing aids fitted with the NAL-NL2 formula for mild to moderately severe hearing loss degrees in three input intensities of 50, 65, and 80 dB SPL, the highest gain was at the frequency of 4000 Hz (P=0.001) and the lowest gain was at the frequency of 200 Hz (P=0.004).
As indicated in Figure 2, for hearing aids fitted with the NAL-NL2 formula for moderately severe to severe hearing loss at 50 dB SPL input intensity level, the highest gain was at the frequency of 3000 Hz (P=0.002) and the lowest gain was at the frequency of 200 Hz (P=0.003), while the highest gain was at 4,000 Hz frequency (P=0.002) and the lowest gain was in 200 Hz frequency (P=0.003) at 65 and 80 dB SPL intensity input levels.
Figure 3 indicates that the highest gain was at the frequency of 1000 Hz (P=0.007) and the lowest gain was at the frequency of 8000 Hz (P=0.005) for hearing aids fitted with DSLi/o v5 formula for mild to moderately severe hearing loss at 50 dB SPL input intensity level, while the highest gain was at 3000 Hz frequency (P=0.006) and the lowest gain was at 8000 Hz frequency (P=0.002) at 65 and 80 dB SPL intensity input levels.
As Figure 4 illustrates, the highest gain was at the frequency of 1000 Hz (P=0.003) and the lowest gain was at the frequency of 8000 Hz (P=0.001) for hearing aids fitted with DSLi/o v5 formula for moderately severe to severe hearing loss at 50, 65, and 80 dB SPL input intensity levels.
Using hearing aids fitted with NAL-NL2 formula at 50 dB SPL input intensity level, the highest gain was at the frequency of 4000 Hz (P=0.005) and the lowest gain was at the frequency of 200 Hz (P=0.002) for mild to moderately severe hearing loss, while the highest gain was at 3000 Hz frequency (P=0.007) and the lowest gain was at 200 Hz frequency (P=0.003) for moderately severe to severe hearing loss. Using DSLi/o v5 obtained the highest gain at 1000 Hz frequency (P=0.001) and the lowest gain at 8000 Hz frequency (P=0.004) for both mild to moderately severe and moderately severe to severe hearing loss degrees. In general, the DSLi/o v5 formula exerts higher average gains at both hearing loss degrees.
The highest gain was at the frequency of 4000 Hz (P=0.008) and the lowest gain was at the frequency of 200 Hz (P=0.006) for hearing aids fitted with the NAL-NL2 formula for both mild to moderately severe and moderately severe to severe hearing loss degrees at 65 dB SPL input intensity. Using the DSLi/o v5 formula for mild to moderately severe hearing loss, the highest gain was observed at 3000 Hz frequency (P=0.001) and the lowest gain was observed at 8000 Hz frequency (P=0.012). In general, the DSLi/o v5 formula exerts a higher average gain at both hearing loss degrees.
In both mild to moderately severe and moderately severe to severe hearing loss degrees, fitting the hearing aid with the NAL-NL2 formula at 80 dB SPL input intensity level yields the highest gain at 4000 Hz frequency (P=0.003) and the lowest gains at 200 and 8000 Hz frequency, respectively (P=0.002 and P=0.009, respectively). Using DSLi/o v5 formula exerts the highest gain at 3000 Hz frequency (P=0.002) and the lowest gain at 8000 Hz frequency (P=0.001) in mild to moderately severe hearing loss, while it exerts the highest gain at 1000 Hz frequency (P=0.001) and the lowest gain at 8000 Hz frequency (P=0.009) in moderately severe to severe hearing loss. Generally, DSLi/o v5 yields higher average gain at both hearing loss degrees.
4. Discussion
Hearing aid response modification and examination of its efficiency and usefulness are among audiological rehabilitation objectives that are practiced immediately after the hearing aid is fine-tuned and its function is validated. The validation of a hearing aid’s appropriate gain does not necessarily mean that the hearing aid is effective. The main factor contributing to the effectiveness is the hearing aid’s gain and electroacoustic parameters having an effective function in hearing. The validation of the hearing aid’s usefulness is dependent on mental, real, and verbal tests in various situations.
As indicated in other studies, non-linear hearing aids fitted with NAL-NL2 and DSLi/o v5 formulas exert different gains at 50, 65, and 80 dB SPL intensity levels. The exerted gains for the aforementioned input intensities were constantly observed to be significantly higher at 50 dB SPL compared with the other two input intensities (P=0.001). Using NAL-NL2 and DSLi/o v5 formulas for both mild to moderately severe and moderately severe to severe hearing loss degrees, the highest exerted gain was observed at the input intensity level of 50 dB SPL (P=0.002 and P=0.009, respectively) while the lowest gain was observed at 80 dB SPL (P=0.003 and P=0.007, respectively) input intensity level. This difference between the prescribed gains was significant and consistent with the findings of similar studies [12, 13, 14].
In terms of hearing loss degrees, it can be said that both NAL-NL2 and DSLi/o v5 exerted a significantly higher average gain for moderately severe to severe hearing loss compared with that of mild to moderately severe hearing loss. This difference between the prescribed gains was significant and consistent with the findings of similar studies [12, 15].
In terms of the reconstruction of filtered intensity content at 50 dB SPL input level, it can be said that DSLi/o v5 exerted a higher average gain and intensity reconstruction at both hearing loss degrees at an input intensity level of 50 dB in low and medium frequencies (P=0.001 and P=0.002, respectively). However, the two formulas indicated the same performance in high frequencies (P=0.004) and the NAL-NL2 formula might even exert higher gains for those with mild to moderately severe hearing loss at higher frequencies (P=0.014). Also, in terms of the reconstruction of filtered intensity content at 65 and 80 dB SPL input levels, it can be said that DSLi/o v5 formula revealed to exert higher gains at both hearing loss degrees (P=0.006 and P=0.002 respectively) that is consistent with the findings of other studies [13, F].
5.Conclusion
By comparing the two formulas, it can be inferred that DSLi/o v5 exerted higher average gains compared with NAL-NL2 for both hearing loss degrees and at all three input levels. Therefore, depending on the purpose of gain prescription, whether the loudness is important, or speech intelligibility, the choice of appropriate fitting formula and other specific prescription qualities can be affected.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
The paper was extracted from the MSc. thesis of the first author at Department of Audiology, School of Rehabilitation Sciences, Iran University of Medical Science, Tehran.
Authors' contributions
All authors equally contributed to preparing this article
Conflict of interest
The authors declared no conflict of interest.
Refrences:
- Korver AM, Smith RJ, Van Camp G, Schleiss MR, Bitner-Glindzicz MA, Lustig LR, et al. Congenital hearing loss. Nat Rev Dis Primers. 2017; 3(1):1-17. [DOI:10.1038/nrdp.2016.94] [PMID] [PMCID]
- Robinshaw HMJBjoa. The pattern of development from non-communicative behaviour to language by hearing impaired and hearing infants. Int J Audiol. 1996; 30(3):177-98. [DOI:10.3109/03005369609079039] [PMID]
- Dillon H. Hearing aids. London: Hodder Arnold; 2008. https://www.amazon.com/Hearing-Aids-Harvey-Dillon/dp/1604068108
- Stelmachowicz PG, Pittman AL, Hoover BM, Lewis DE. Aided perception of /s/ and /z/ by hearing-impaired children. Ear Hear. 2002; 23(4):316-24. [DOI:10.1097/00003446-200208000-00007] [PMID]
- Stelmachowicz PG, Pittman AL, Hoover BM, Lewis DE. Effect of stimulus bandwidth on the perception of /s/ in normal- and hearing-impaired children and adults. J Acoust Soc Am. 2001; 110(4):2183-90. [DOI:10.1121/1.1400757] [PMID]
- Eddins DA. Sandlin’s textbook of hearing aid amplification, 3rd Edition. Oxfordshire: Taylor & Francis; 2014. [DOI:10.3109/14992027.2014.965797]
- Yadav N, Kumar S, Annapurna S, Vinila VJJT, Studies PiL. The effect of stimulus bandwidth on perception of fricative/s/among individuals with different degrees of sensorineural hearing loss. Theory Practice Lang Stud. 2011; 1(12):1679-87. [DOI:10.4304/tpls.1.12.1679-1687]
- Fabry DA. Nonlinear hearing AIDS and verification of fitting targets. Trends Amplif. 2003; 7(3):99-115. [DOI:10.1177/108471380300700303] [PMID] [PMCID]
- Holube I, Fredelake S, Vlaming M, Kollmeier B. Development and analysis of an International Speech Test Signal (ISTS). Int J Audiol. 2010; 49(12):891-903. [DOI:10.3109/14992027.2010.506889] [PMID]
- Dillon H. Hearing aids/Harvey Dillon. Boomerang Press; Thieme Sydney: New York; 2012. https://catalogue.nla.gov.au/Record/5815051
- Tate Maltby M. Principles of Hearing Aid Audiology. Journal of Audiological Medicine. New Jersey: Wiley; 2002. https://www.wiley.com/en-us/
- Keidser G, Dillon H, Flax M, Ching T, Brewer S. The NAL-NL2 prescription procedure. Audiol Res. 2011; 1(1):e24. [DOI:10.4081/audiores.2011.e24] [PMID] [PMCID]
- Ching TY, Zhang VW, Johnson EE, Van Buynder P, Hou S, Burns L, et al. Hearing aid fitting and developmental outcomes of children fit according to either the NAL or DSL prescription: Fit-to-target, audibility, speech and language abilities. Int J Audiol. 2018; 57(suple 2):S41-S54. [DOI:10.1080/14992027.2017.1380851] [PMID] [PMCID]
- Keidser G, Dillon H, Carter L, O’Brien A. NAL-NL2 empirical adjustments. Trends Amplif. 2012; 16(4):211-23. [DOI:10.1177/1084713812468511] [PMID] [PMCID]
- Marriage JE, Vickers DA, Baer T, Glasberg BR, Moore BC. Comparison of different hearing aid prescriptions for children. Ear Hear. 2018; 39(1):20-31. [DOI:10.1097/AUD.0000000000000460] [PMID]
Type of Study: Research |
Subject:
Audiology
Received: 2020/10/30 | Accepted: 2020/12/1 | Published: 2020/12/3
Received: 2020/10/30 | Accepted: 2020/12/1 | Published: 2020/12/3
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.