

Volume 3, Issue 1 (Continuously Updated 2020)
Func Disabil J 2020, 3(1): 141-150 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghoreishi Z S, Azimian M, Alaghband Rad J, Khorrami Banaraki A, Rafiee S M, Salavati M, et al . Analysis of Connected Speech in Persian Aphasic Patients and its Relationship With Type and Severity of Aphasia. Func Disabil J 2020; 3 (1) :141-150
URL: http://fdj.iums.ac.ir/article-1-118-en.html
URL: http://fdj.iums.ac.ir/article-1-118-en.html
Zahra Sadat Ghoreishi1 

 , Mojtaba Azimian *2 , Javad Alaghband Rad3 , Anahita Khorrami Banaraki4 , Seyed Majid Rafiee1 , Mahyar Salavati5 , Amir Shiani6 , Narges Bayat1
, Mojtaba Azimian *2 , Javad Alaghband Rad3 , Anahita Khorrami Banaraki4 , Seyed Majid Rafiee1 , Mahyar Salavati5 , Amir Shiani6 , Narges Bayat1
, Mojtaba Azimian *2 , Javad Alaghband Rad3 , Anahita Khorrami Banaraki4 , Seyed Majid Rafiee1 , Mahyar Salavati5 , Amir Shiani6 , Narges Bayat1
1- Department of Speech Therapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Clinical Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,mazimian@yahoo.com
3- Department of Psychiatry, Psychology Research Center, Roozbeh Hospital, Tehran University of Medical Sciences, Tehran, Iran.
4- Brain and Cognition Clinic, Tehran, Iran.
5- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
6- Department of Speech Therapy, School of Rehabilitation Sciences, Kermanshah University of Medical Sciences, Kermanshah, Iran.
2- Department of Clinical Sciences, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. ,
3- Department of Psychiatry, Psychology Research Center, Roozbeh Hospital, Tehran University of Medical Sciences, Tehran, Iran.
4- Brain and Cognition Clinic, Tehran, Iran.
5- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
6- Department of Speech Therapy, School of Rehabilitation Sciences, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Full-Text [PDF 1190 kb]
(719 Downloads)
| Abstract (HTML) (1929 Views)
Full-Text: (797 Views)
1. Introduction
From the perspective of a therapist, it is important to analyze connected speech in order to have a comprehensive assessment and treatment planning [1]. There are lots of tests evaluating the type and severity of aphasia [2, 3], but none of them can provide a comprehensive assessment in a short time. Connected speech can provide a comprehensive profile of strengths and weaknesses of a patient’s linguistic ability within the shortest time possible, and is affected in all types of aphasia [4, 5]. Daily communication is reportedly an appropriate representative of the strengths and weaknesses of speech production in its context [6]. Since Expressive language is an important part of daily communication, analysis of connected speech could be a functional measure for expressive language [7].
Rate of speech and Mean Length of Utterance (MLU) are the two main factors to classify aphasia as either fluent or non-fluent [8-11]. According to Wilson (2010), “fluency is a multidimensional construct that encompasses features, such as speech rate, phrase length, articulatory agility, and syntactic structure, which are not always impacted in parallel” [1]. As such, by definition, a non-fluent aphasic patient’s speech is slow, dysprosodic, telegraphic, and effortful. Fluent aphasic patients have normal or near the normal speech rate with relatively normal syntax and melody; however, their speech is empty and full of jargon [12].
On the other hand, the social importance of connected speech and its role in functional communication is also mentioned in several other studies [13]. Since the 1970s, a new approach to aphasiology emerged with a focus on communication problems in daily living instead of concentration on linguistic problems of aphasic patients [14]. Meanwhile, the international classification of impairment, disabilities, and handicaps (ICIDH) published by the World Health Organization [15], supported the functional communication approach to aphasia. This approach has an enormous impact on the assessment of neurogenic communication disorders. Thus, the social aspects of the impairments gained attention more than linguistic deficit [16]. Connected speech is one of the main factors to define verbal functional communication [17]. Although many previous tests have been designed according to this approach (e.g. Western Aphasia Battery (WAB) and Boston diagnostic Aphasia Exam (BDAE) for aphasia diagnosis they did not instruct clearly how to analyze or measure spontaneous speech [18]. Thus. many articles have been written on the methods and parameters of speech analysis [19-21].
Spontaneous, descriptive, and free speech in aphasia literature are all related concepts. Prins (2004) [18] in his review article about the analysis of spontaneous speech, divided connected speech into real spontaneous speech and semi-real spontaneous speech. According to his definition, real spontaneous speech is elicited through the interview with the patient using open questions or a dialogue between the patient and his/her familiar partner or therapist, and semi-spontaneous speech is extracted by describing pictures or retelling a familiar story or role-playing [18].
Language parameters have been concerned; however, assessing connected speech varies in different studies. Sajjadi et al. (2012) analyzed some parameters, such as the mean length of utterances, frequency of relative sentences, and verb agreement errors in connected speech of patients with aphasia [22]. Speech rate, lexical content, and syntactic structure were assessed by Wilson et al. (2010) in his study on connected speech in aphasia [1].
Nicholas et al. (1993) in their study focused on some parameters of connected speech, like words per minute, percentage of correct information units, and correct information unites per minute in aphasic patients [23]. Content units, syllables per minute, and content units per minute were analyzed in a study by Yorkstone and Beukelman on speech samples of patients with aphasia [24]. The last two studies indicated that the speech rate has a long history as one of the speech measure indices for the analysis of connected speech.
There are various methods for the evaluation of speech, including the Spontaneous Speech Language Analysis (SSLA) system [25] or the system described by Mayer [21]. We used some parts of SSLA variables in the current study. Eight measures of speech, including speech rate, MLU, number of utterances, total words, content words, function words, nouns, and verbs were selected.
Objectives
The main purpose of this study was to assess the parameters of connected speech of aphasic patients in comparison with a normal matched group. Moreover, measuring the relationship between connected speech parameters and severity of aphasia was another purpose of the present study.
2. Materials and Methods
In this descriptive cross-sectional study, we compared the performances of 27 right-handed patients with aphasia with the control group. The inclusion criteria for aphasic patients were the presence of aphasia secondary to left hemisphere brain damage without any history of psychiatric or other neurological disorders. The neurologic assessment was done by a neurologist and the diagnosis of aphasia was done by a speech therapist using the Persian WAB (P-WAB). Controlled matched right-handed group, were adults over 27 years old living in Tehran. They were native Persian speakers with no history of psychiatric or neurological disorders.
Nest Bird’s story pictures were used to extract speech samples for both aphasic patients and the control group. Parameters of connected speech, including speech rate, MLU, number of utterances, total words, content words, function words, nouns, and verbs were measured. Both groups were matched based on age, gender, and education. Finally, the correlation between connected speech parameters and severity of aphasia was measured. The severity of aphasia was obtained through an Aphasia Quotient (AQ) score extracted from P-WAB.
The utterance is the smallest unit of speech, which is bounded by silence. In order to calculate MLU, the total number of words should be divided into the total number of utterances [26].
Content words are the words with meaning and give us the most important information, such as “bird”, “tree”, and “cry”. Nouns, verbs, adjectives, and adverbs are considered as content words. A noun refers to a person, place, or thing, etc. A verb tells us about the action happening, or the state. Adjectives give us details about objects and people and adverbs tell us how, when, or where something is done [27].
Function words explain or create grammatical or structural relationships, which the content words may fit into them. These words mostly do not have meaning on their own; like “the”, “in” “to”, “as”. Pronouns, prepositions, conjunctions, determiners, qualifiers, and interrogatives are some examples of function words [27].
All participants were instructed: “please see these serial pictures and describe it completely”. Language samples were recorded and analyzed afterward.
3. Results
Table 1 showed that the Mean±SD age of aphasic patients and the control groups was 53.27±9.07 and 54.83±14.62, respectively. The normality of data was checked using the Kolmogorov-Smirnov test and the normal distribution of data was confirmed.

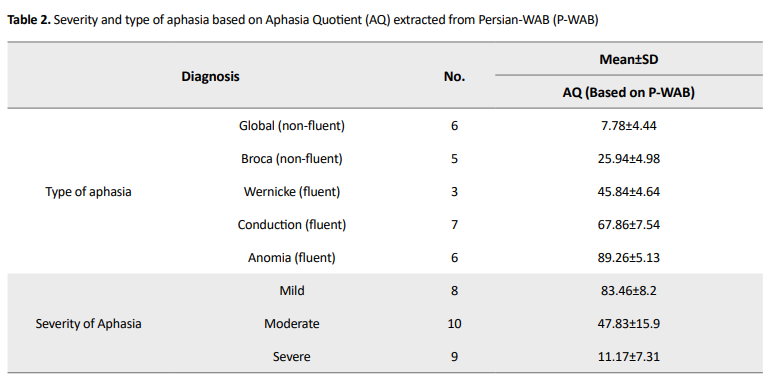
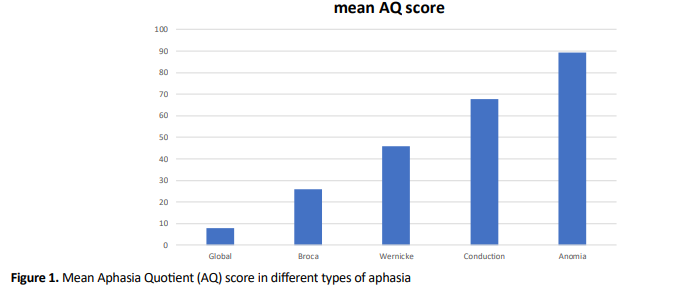
Table 2 presents the type and severity of aphasia based on the P-WAB test [28, 29]. Figure 1 shows the difference between the mean AQ score (based on P-WAB) in different types of aphasia groups.
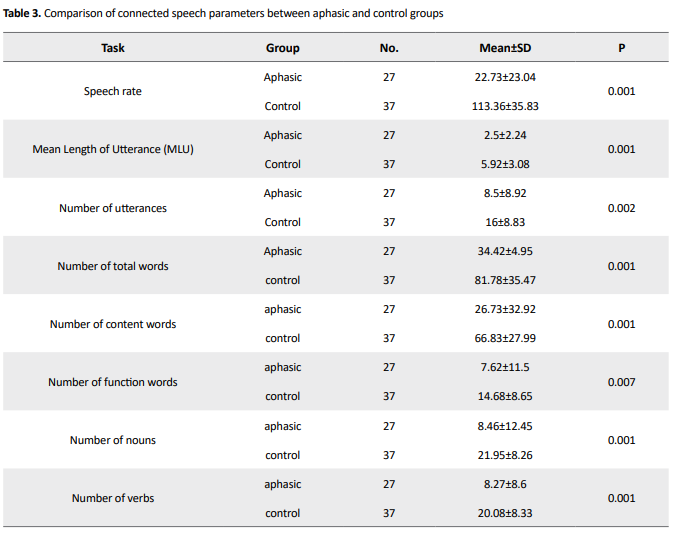
A significant difference was found between the groups in all parameters of connected speech (P<0.01) (Table 3).
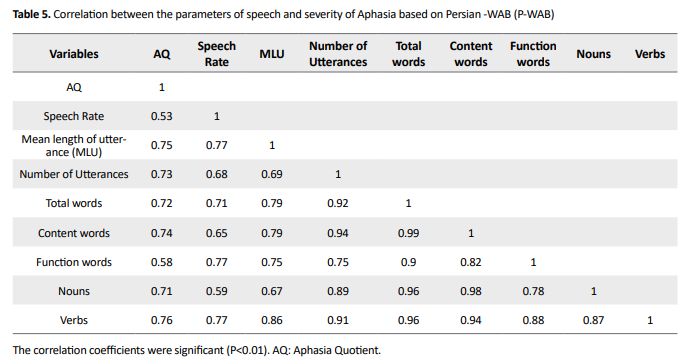
The correlation coefficient between speech parameters and severity of aphasia ranged from 0.71 to 0.76 and were strongly correlated (P<0.01) apart from the speech rate and the number of function words (Table 4).
According to Figure 2, the number of function words, nouns, and verbs had significant differences between the aphasic and control groups. The number of function words in the aphasic group was nearly half of this number in normal people. There were considerable differences in the number of nouns and verbs between the two aphasic and normal groups. However, this difference was less notable in the number of function words between the two groups.
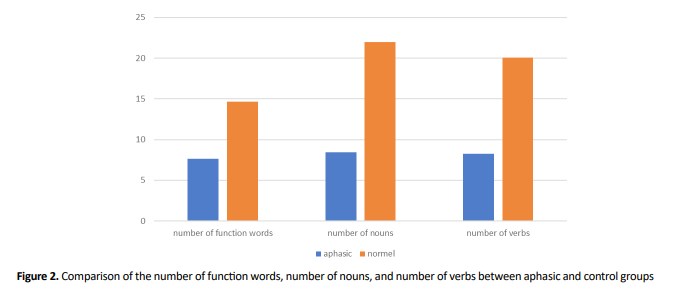
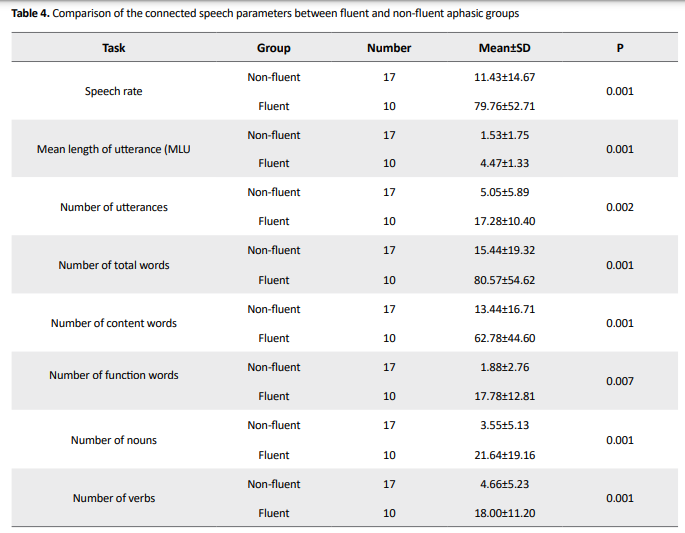
Table 4 presents the comparison of connected speech parameters between fluent and non-fluent aphasic groups. All the parameters showed a higher mean in fluent aphasia patients.
4. Discussions
The present study initially assessed the parameters of connected speech of aphasic patients in comparison with the normal matched group. Then, the correlation between connected speech measures and severity of aphasia was analyzed. In this article, we documented the language profile of aphasic patients and the normal matched group (Table 5).
To the best of our knowledge, this study was the first Persian report of analysis of connected speech in aphasic patients. Analysis of connected speech is important from both theoretical and practical dimensions. Many articles have been published by linguistics on connected speech [30, 31]. However, it is mandatory for clinicians to use the results of connected speech analysis in the assessment and treatment planning. In this article, the experts with clinical experiences presented indices of speech measures in the analysis of connected speech. This report considered connected speech analysis based on the type and severity of aphasia. We implemented a picture description task to control the content of spontaneous speech. A similar approach has been taken by Yorkston and Beukelman (1977), who used the picture description task as a more replicable and predictable measure [26].
The ability to retrieve precise words for objects, events, relationships, and ideas during unstructured and spontaneous language production it is important to conveying concepts. In addition, the ability of a person with aphasia to produce content during highly structured tasks may differ from his or her abilities during less structured communication activities that require greater amounts of verbal or written output and more thinking to prepare the response. Therefore, clinicians analyze samples of their patients’ spoken or written connected language to determine the accuracy, responsiveness, completeness, promptness, and efficiency of the content (Chapey 2014).
Shewan published a study about connected speech analysis in patients with aphasia. He assessed the number of utterances, the total speaking time, rate of speech, length of utterances, melody, articulation, number of complex sentences, syntactic and morphological errors, content units, paraphasias, repetitions, and communication efficiency [25]. In this report, some of these parameters are measured.
As seen in Table 3, all parameters were significantly different between the two groups. These findings are consistent with the results of Shewan on speech rate, MLU, and the number of utterances [25].
As indicated in Table 4, MLU, number of utterances, total words, content words, nouns, and verbs were significantly correlated with the severity of aphasia. These results were expected because AQ is representative of the language performance of aphasia [32]. Furthermore connected speech is one of the language components impaired in all types of aphasia. Hence, AQ was correlated with connected speech measures apart from speech rate and function words.
In our study, speech rate was not correlated with aphasia severity. This does not seem to be surprising as fluency is not a real measure for the severity of aphasia and a representative of whole language performance. In addition, the speech rate did not change in parallel with AQ. It is noteworthy that all of the four types of fluent aphasia (Wernicke, Sensory Transcortical, Conduction, and Anomia) did not have lower severity than the four types of non – fluent aphasia (Broca, Motor Transcortical, Global and Mixed Transcortical). For instance, according to the taxonomy of aphasia based on WAB, Motor Transcortical aphasia had better AQ in WAB in comparison with Wernicke aphasia. The result of this study explains why the speech rate could not anticipate the severity of aphasia.
As indicated in Figure 2, there were significant differences between the two aphasic and control groups in the number of function words, nouns, and verbs. This result also was reported by Gleason (1980) who studied the narrative strategies of aphasic and normal people [33].
According to our results, a strong correlation was found between MLU and the number of action words (verb), probably because both of them are indices of the complexity of the language [34]. However, according to some studies, MLU is not a proper index to determine the language level [35].
In our study, the score of connected speech in the normal group might demonstrate a horizon for expected performance for aphasic patients. The results of this study are in the same direction as the findings of Shewan [25] and can be used as the first step of a preliminary scale for Persian patients.
According to Hussmann et al. (2012), fluent aphasic patients have higher MLU than non-fluent aphasia patients, which is reported in our study. Also, in our study, the average number of words, content words, and function words were higher in fluent aphasic patients than non-fluent aphasic patients as reported by Heim et al. (2013) [36]. A higher average of speech rate in fluent aphasic patients was reported by Benson (1967), who compared some measures of verbal output in fluent and non-fluent types of aphasia. Other measures, like the number of nouns and verbs, were reported in the Benson study (1967), which is consistent with our findings [37]. Non-fluent aphasic patients have a lower average of nouns and verbs than fluent aphasic patients based on our findings.
Due to the limited number of studies on the analysis of spontaneous speech for Iranian aphasic patients, the present study could be intriguing clinically and paves the way for future studies.
5. Conclusions
This first report of connected speech parameters of Persian aphasic patients exhibited a useful scale for clinical use. The connected speech is informative enough to give us a view about the patient’s ability in expressive language on one hand, and on the other hand, there is a high correlation between speech parameters and the severity of aphasia. It is suggested to use “connected speech analysis” for the assessment and treatment of aphasia.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1395.401).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision: Zahra Sadat Ghoreishi, Mojtaba Azimian, Javad Alaghband Rad; Methodology: Zahra Sadat Ghoreishi, Amir Shiani, Mahyar Salavati; Writing-original draft: Zahra Sadat Ghoreishi, Narges Bayat; Investigations, writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
From the perspective of a therapist, it is important to analyze connected speech in order to have a comprehensive assessment and treatment planning [1]. There are lots of tests evaluating the type and severity of aphasia [2, 3], but none of them can provide a comprehensive assessment in a short time. Connected speech can provide a comprehensive profile of strengths and weaknesses of a patient’s linguistic ability within the shortest time possible, and is affected in all types of aphasia [4, 5]. Daily communication is reportedly an appropriate representative of the strengths and weaknesses of speech production in its context [6]. Since Expressive language is an important part of daily communication, analysis of connected speech could be a functional measure for expressive language [7].
Rate of speech and Mean Length of Utterance (MLU) are the two main factors to classify aphasia as either fluent or non-fluent [8-11]. According to Wilson (2010), “fluency is a multidimensional construct that encompasses features, such as speech rate, phrase length, articulatory agility, and syntactic structure, which are not always impacted in parallel” [1]. As such, by definition, a non-fluent aphasic patient’s speech is slow, dysprosodic, telegraphic, and effortful. Fluent aphasic patients have normal or near the normal speech rate with relatively normal syntax and melody; however, their speech is empty and full of jargon [12].
On the other hand, the social importance of connected speech and its role in functional communication is also mentioned in several other studies [13]. Since the 1970s, a new approach to aphasiology emerged with a focus on communication problems in daily living instead of concentration on linguistic problems of aphasic patients [14]. Meanwhile, the international classification of impairment, disabilities, and handicaps (ICIDH) published by the World Health Organization [15], supported the functional communication approach to aphasia. This approach has an enormous impact on the assessment of neurogenic communication disorders. Thus, the social aspects of the impairments gained attention more than linguistic deficit [16]. Connected speech is one of the main factors to define verbal functional communication [17]. Although many previous tests have been designed according to this approach (e.g. Western Aphasia Battery (WAB) and Boston diagnostic Aphasia Exam (BDAE) for aphasia diagnosis they did not instruct clearly how to analyze or measure spontaneous speech [18]. Thus. many articles have been written on the methods and parameters of speech analysis [19-21].
Spontaneous, descriptive, and free speech in aphasia literature are all related concepts. Prins (2004) [18] in his review article about the analysis of spontaneous speech, divided connected speech into real spontaneous speech and semi-real spontaneous speech. According to his definition, real spontaneous speech is elicited through the interview with the patient using open questions or a dialogue between the patient and his/her familiar partner or therapist, and semi-spontaneous speech is extracted by describing pictures or retelling a familiar story or role-playing [18].
Language parameters have been concerned; however, assessing connected speech varies in different studies. Sajjadi et al. (2012) analyzed some parameters, such as the mean length of utterances, frequency of relative sentences, and verb agreement errors in connected speech of patients with aphasia [22]. Speech rate, lexical content, and syntactic structure were assessed by Wilson et al. (2010) in his study on connected speech in aphasia [1].
Nicholas et al. (1993) in their study focused on some parameters of connected speech, like words per minute, percentage of correct information units, and correct information unites per minute in aphasic patients [23]. Content units, syllables per minute, and content units per minute were analyzed in a study by Yorkstone and Beukelman on speech samples of patients with aphasia [24]. The last two studies indicated that the speech rate has a long history as one of the speech measure indices for the analysis of connected speech.
There are various methods for the evaluation of speech, including the Spontaneous Speech Language Analysis (SSLA) system [25] or the system described by Mayer [21]. We used some parts of SSLA variables in the current study. Eight measures of speech, including speech rate, MLU, number of utterances, total words, content words, function words, nouns, and verbs were selected.
Objectives
The main purpose of this study was to assess the parameters of connected speech of aphasic patients in comparison with a normal matched group. Moreover, measuring the relationship between connected speech parameters and severity of aphasia was another purpose of the present study.
2. Materials and Methods
In this descriptive cross-sectional study, we compared the performances of 27 right-handed patients with aphasia with the control group. The inclusion criteria for aphasic patients were the presence of aphasia secondary to left hemisphere brain damage without any history of psychiatric or other neurological disorders. The neurologic assessment was done by a neurologist and the diagnosis of aphasia was done by a speech therapist using the Persian WAB (P-WAB). Controlled matched right-handed group, were adults over 27 years old living in Tehran. They were native Persian speakers with no history of psychiatric or neurological disorders.
Nest Bird’s story pictures were used to extract speech samples for both aphasic patients and the control group. Parameters of connected speech, including speech rate, MLU, number of utterances, total words, content words, function words, nouns, and verbs were measured. Both groups were matched based on age, gender, and education. Finally, the correlation between connected speech parameters and severity of aphasia was measured. The severity of aphasia was obtained through an Aphasia Quotient (AQ) score extracted from P-WAB.
The utterance is the smallest unit of speech, which is bounded by silence. In order to calculate MLU, the total number of words should be divided into the total number of utterances [26].
Content words are the words with meaning and give us the most important information, such as “bird”, “tree”, and “cry”. Nouns, verbs, adjectives, and adverbs are considered as content words. A noun refers to a person, place, or thing, etc. A verb tells us about the action happening, or the state. Adjectives give us details about objects and people and adverbs tell us how, when, or where something is done [27].
Function words explain or create grammatical or structural relationships, which the content words may fit into them. These words mostly do not have meaning on their own; like “the”, “in” “to”, “as”. Pronouns, prepositions, conjunctions, determiners, qualifiers, and interrogatives are some examples of function words [27].
All participants were instructed: “please see these serial pictures and describe it completely”. Language samples were recorded and analyzed afterward.
3. Results
Table 1 showed that the Mean±SD age of aphasic patients and the control groups was 53.27±9.07 and 54.83±14.62, respectively. The normality of data was checked using the Kolmogorov-Smirnov test and the normal distribution of data was confirmed.
Table 2 presents the type and severity of aphasia based on the P-WAB test [28, 29]. Figure 1 shows the difference between the mean AQ score (based on P-WAB) in different types of aphasia groups.
A significant difference was found between the groups in all parameters of connected speech (P<0.01) (Table 3).
The correlation coefficient between speech parameters and severity of aphasia ranged from 0.71 to 0.76 and were strongly correlated (P<0.01) apart from the speech rate and the number of function words (Table 4).
According to Figure 2, the number of function words, nouns, and verbs had significant differences between the aphasic and control groups. The number of function words in the aphasic group was nearly half of this number in normal people. There were considerable differences in the number of nouns and verbs between the two aphasic and normal groups. However, this difference was less notable in the number of function words between the two groups.
Table 4 presents the comparison of connected speech parameters between fluent and non-fluent aphasic groups. All the parameters showed a higher mean in fluent aphasia patients.
4. Discussions
The present study initially assessed the parameters of connected speech of aphasic patients in comparison with the normal matched group. Then, the correlation between connected speech measures and severity of aphasia was analyzed. In this article, we documented the language profile of aphasic patients and the normal matched group (Table 5).
To the best of our knowledge, this study was the first Persian report of analysis of connected speech in aphasic patients. Analysis of connected speech is important from both theoretical and practical dimensions. Many articles have been published by linguistics on connected speech [30, 31]. However, it is mandatory for clinicians to use the results of connected speech analysis in the assessment and treatment planning. In this article, the experts with clinical experiences presented indices of speech measures in the analysis of connected speech. This report considered connected speech analysis based on the type and severity of aphasia. We implemented a picture description task to control the content of spontaneous speech. A similar approach has been taken by Yorkston and Beukelman (1977), who used the picture description task as a more replicable and predictable measure [26].
The ability to retrieve precise words for objects, events, relationships, and ideas during unstructured and spontaneous language production it is important to conveying concepts. In addition, the ability of a person with aphasia to produce content during highly structured tasks may differ from his or her abilities during less structured communication activities that require greater amounts of verbal or written output and more thinking to prepare the response. Therefore, clinicians analyze samples of their patients’ spoken or written connected language to determine the accuracy, responsiveness, completeness, promptness, and efficiency of the content (Chapey 2014).
Shewan published a study about connected speech analysis in patients with aphasia. He assessed the number of utterances, the total speaking time, rate of speech, length of utterances, melody, articulation, number of complex sentences, syntactic and morphological errors, content units, paraphasias, repetitions, and communication efficiency [25]. In this report, some of these parameters are measured.
As seen in Table 3, all parameters were significantly different between the two groups. These findings are consistent with the results of Shewan on speech rate, MLU, and the number of utterances [25].
As indicated in Table 4, MLU, number of utterances, total words, content words, nouns, and verbs were significantly correlated with the severity of aphasia. These results were expected because AQ is representative of the language performance of aphasia [32]. Furthermore connected speech is one of the language components impaired in all types of aphasia. Hence, AQ was correlated with connected speech measures apart from speech rate and function words.
In our study, speech rate was not correlated with aphasia severity. This does not seem to be surprising as fluency is not a real measure for the severity of aphasia and a representative of whole language performance. In addition, the speech rate did not change in parallel with AQ. It is noteworthy that all of the four types of fluent aphasia (Wernicke, Sensory Transcortical, Conduction, and Anomia) did not have lower severity than the four types of non – fluent aphasia (Broca, Motor Transcortical, Global and Mixed Transcortical). For instance, according to the taxonomy of aphasia based on WAB, Motor Transcortical aphasia had better AQ in WAB in comparison with Wernicke aphasia. The result of this study explains why the speech rate could not anticipate the severity of aphasia.
As indicated in Figure 2, there were significant differences between the two aphasic and control groups in the number of function words, nouns, and verbs. This result also was reported by Gleason (1980) who studied the narrative strategies of aphasic and normal people [33].
According to our results, a strong correlation was found between MLU and the number of action words (verb), probably because both of them are indices of the complexity of the language [34]. However, according to some studies, MLU is not a proper index to determine the language level [35].
In our study, the score of connected speech in the normal group might demonstrate a horizon for expected performance for aphasic patients. The results of this study are in the same direction as the findings of Shewan [25] and can be used as the first step of a preliminary scale for Persian patients.
According to Hussmann et al. (2012), fluent aphasic patients have higher MLU than non-fluent aphasia patients, which is reported in our study. Also, in our study, the average number of words, content words, and function words were higher in fluent aphasic patients than non-fluent aphasic patients as reported by Heim et al. (2013) [36]. A higher average of speech rate in fluent aphasic patients was reported by Benson (1967), who compared some measures of verbal output in fluent and non-fluent types of aphasia. Other measures, like the number of nouns and verbs, were reported in the Benson study (1967), which is consistent with our findings [37]. Non-fluent aphasic patients have a lower average of nouns and verbs than fluent aphasic patients based on our findings.
Due to the limited number of studies on the analysis of spontaneous speech for Iranian aphasic patients, the present study could be intriguing clinically and paves the way for future studies.
5. Conclusions
This first report of connected speech parameters of Persian aphasic patients exhibited a useful scale for clinical use. The connected speech is informative enough to give us a view about the patient’s ability in expressive language on one hand, and on the other hand, there is a high correlation between speech parameters and the severity of aphasia. It is suggested to use “connected speech analysis” for the assessment and treatment of aphasia.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1395.401).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, supervision: Zahra Sadat Ghoreishi, Mojtaba Azimian, Javad Alaghband Rad; Methodology: Zahra Sadat Ghoreishi, Amir Shiani, Mahyar Salavati; Writing-original draft: Zahra Sadat Ghoreishi, Narges Bayat; Investigations, writing-review & editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Wilson SM, Henry ML, Besbris M, Ogar JM, Dronkers NF, Jarrold W, et al. Connected speech production in three variants of primary progressive aphasia. Brain. 2010; 133(7):2069-88. [DOI:10.1093/brain/awq129] [PMID] [PMCID]
- Nilipour R, Pourshahbaz A, Ghoreyshi ZS. Reliability and validity of bedside version of Persian WAB (P-WAB-1). Basic Clin Neurosci. 2014; 5(4):253-8. [PMID] [PMCID]
- Nilipour R, Pour Shahbaz A, Ghoreishi ZS, Yousefi A. [Reliability and Validity of Persian Aphasia Battery Test (Persian)]. Salmand: Iran J Ageing. 2016; 10(4):182-91. http://salmandj.uswr.ac.ir/article-1-835-en.html
- Shewan CM. Expressive language recovery in aphasia using the Shewan Spontaneous Language Analysis (SSLA) system. J communic disord. 1988; 21(2):155-69. [DOI:10.1016/0021-9924(88)90003-2]
- Vermeulen J, Bastiaanse R, Van Wageningen B. Spontaneous speech in aphasia: A correlational study. Brain Lang. 1989; 36(2):252-74. [DOI:10.1016/0093-934X(89)90064-3]
- Armstrong E, Ferguson A. Language, meaning, context, and functional communication. Aphasiology. 2010; 24(4):16. [DOI:10.1080/02687030902775157]
- Olness GS, Gyger J, Thomas K. Analysis of narrative functionality: Toward evidence-based approaches in managed care settings. Semin Speech Lang. 2012; 33(1):55-67. [DOI:10.1055/s-0031-1301163] [PMID]
- Goodglass H, Hyde MR, Blumstein S. Frequency, picturability and availability of nouns in aphasia. Cortex. 1969; 5(2):104-19. [DOI:10.1016/S0010-9452(69)80022-5]
- Kerschensteiner M, Poeck K, Brunner E. The fluency-non fluency dimension in the classification of aphasic speech. Cortex. 1972; 8(2):233-47. [DOI:10.1016/S0010-9452(72)80021-2]
- Gordon JK. The fluency dimension of aphasia. Aphasiology. 1998; 12(7-8):15. [DOI:10.1080/02687039808249565]
- Goodglass HQ, F.A. Timberlake, W.H. Phrase Length and the Type and Severity of Aphasia. Cortex. 1964; 1(2):133-53. [DOI:10.1016/S0010-9452(64)80018-6]
- Kolb B, Whishaw IQ. Fundamentals of human neuropsychology. 5th edition. New York: Worth Publishers; 2003. https://www.worldcat.org/title/fundamentals-of-human-neuropsychology/oclc/55617319
- Wright HH, Capilouto GJ. Considering a multi-level approach to understanding maintenance of global coherence in adults with aphasia. Aphasiology. 2012;26(5):656-72. [DOI:10.1080/02687038.2012.676855] [PMID] [PMCID]
- Holland A. Some practical considerations in aphasia rehabilitation. In: Sullivan MK, M., editor. Rationale for adult aphasia therapy. Omaha: University of Nebraska Medical Center; 1979. pp. 167-180.
- WHO. International classification of impairments, disabilities, and handicaps. Geneva: World Health Organization; 1980.
- Worral L, Frattali CM. Neurogenic communication disorders: A functional approach. New York: Thieme; 2000.
- Doesborgh SJ, van de Sandt-Koenderman WM, Dippel DW, van Harskamp F, Koudstaal PJ, Visch-Brink EG. The impact of linguistic deficits on verbal communication. Aphasiology. 2002; 16(4-6):10. [DOI:10.1080/02687030244000077]
- Prins R, Bastiaanse R. Review. Aphasiology. 2004; 18(12):1075-91. [DOI:10.1080/02687030444000534]
- Grande M, Hussmann K, Bay E, Christoph S, Piefke M, Willmes K, et al. Basic parameters of spontaneous speech as a sensitive method for measuring change during the course of aphasia. Int J Lang Commun Disord. 2008; 43(4):408-26. [DOI:10.1080/13682820701685991] [PMID]
- Hussmann K, Grande M, Meffert E, Christoph S, Piefke M, Willmes K, et al. Computer-assisted analysis of spontaneous speech: Quantification of basic parameters in aphasic and unimpaired language. Clin Linguist Phon. 2012; 26(8):661-80. [DOI:10.3109/02699206.2012.683672] [PMID]
- Mayer J, Murray L. Functional measures of naming in aphasia: Word retrieval in confrontation naming versus connected speech. Aphasiology. 2003; 17(5):481-97. [DOI:10.1080/02687030344000148]
- Sajjadi SA, Patterson K, Tomek M, Nestor PJ. Abnormalities of connected speech in the non-semantic variants of primary progressive aphasia. Aphasiology. 2012; 26(10):1219-37. [DOI:10.1080/02687038.2012.710318]
- Nicholas LE, Brookshire RH. A system for quantifying the informativeness and efficiency of the connected speech of adults with aphasia. J Speech Hear Res. 1993; 36(2):338-50. [DOI:10.1044/jshr.3602.338] [PMID]
- Yorkston KM, Beukelman DR. An analysis of connected speech samples of aphasic and normal speakers. J Speech Hear Disord. 1980; 45(1):27-36. [DOI:10.1044/jshd.4501.27] [PMID]
- Shewan CMJJocd. The Shewan Spontaneous Language Analysis (SSLA) system for aphasic adults: Description, reliability, and validity. J Commun Disord. 1988; 21(2):103-38. [DOI:10.1016/0021-9924(88)90001-9] [PMID]
- Nilipour R. Linguistics and language pathology. Tehran: Hermes; 2001.
- Church KW, Hanks P. Word association norms, mutual information, and lexicography. Comput Ling. 1990; 16(1):22-9. https://dl.acm.org/doi/10.5555/89086.89095
- Ramezani A, Alvani SR, Lashai M, Rad H, Houshiarnejad A, Razani J, et al. Case study of an Iranian-American neuropsychological assessment in the surgical setting: Role of language and tests. Appl Neuropsychol Adult. 1-6. [DOI:10.1080/23279095.2019.1706517]
- Kertesz A, Poole E. The aphasia quotient: The taxonomic approach to measurement of aphasic disability. Can J Neurol Sci. 1974;1(1):7-16. [DOI:10.1017/S031716710001951X] [PMID]
- Nilipour R, Rezai H, Meysami N, Abasiyan Bidgoli S. Neuropsychological double dissociation between linguistic levels: Clinical linguistic evidence from Iranian aphasic patients. Basic Clin Neurosci. 2012; 3(3):5-15. https://applications.emro.who.int/imemrf/Basic_Clin_Neurosci/Basic_Clin_Neurosci_2012_3_3_5_15.pdf
- Nilipour R. Agrammatic language: Two cases from Persian. Aphasiology. 2000;14:1205-42. [DOI:10.1080/02687030050205723]
- Shewan CM, Kertesz A. Reliability and validity characteristics of the Western Aphasia Battery (WAB). J Speech Hear Disord. 1980; 45(3):308-24. [DOI:10.1044/jshd.4503.308] [PMID]
- Gleason JB, Goodglass H, Obler L, Green E, Hyde MR, Weintraub S. Narrative strategies of aphasic and normal-speaking subjects. J Speech Hear Res. 1980; 23(2):370-82. [DOI:10.1044/jshr.2302.370] [PMID]
- Klee T, Stokes S, Wong AM, Fletcher P, Gavin WJ. Utterance length and lexical diversity in Cantonese-speaking children with and without specific language impairment. J Speech Lang Hear Res. 2004; 47(6):14. [DOI:10.1044/1092-4388(2004/104)]
- Eisenberg SL, Fersko TM, Lundgren C. The use of MLU for identifying language impairment in preschool children: A review. Ame J Speech-Language Pathol. 2001; 10(nov):19. [DOI:10.1044/1058-0360(2001/028)]
- Heim S. Advances in experimental psychopatholinguistics: What can we learn from simulation of disorder-like symptoms in human volunteers? Adv Cogn Psycholv. 2013; 9(2):102–11. [DOI:10.2478/v10053-008-0137-6]
- Benson DFJC. Fluency in aphasia: Correlation with radioactive scan localization. Cortex. 1967; 3(4):373-94. [DOI:10.1016/S0010-9452(67)80025-X]
Type of Study: Research |
Subject:
Speech Therapy
Received: 2020/10/20 | Accepted: 2020/11/28 | Published: 2020/12/30
Received: 2020/10/20 | Accepted: 2020/11/28 | Published: 2020/12/30
Contact Information

All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.
Tehran Province, Tehran, District 3, Mirdamad Ave, Nezam Ave, School of Rehabilitation Science
Tel: +98 21 22228051-2 Ext: 180
Fax98 21 22220946
All the work in this journal are licensed under a Creative Commons
ATTRIBUTION-NONCOMMERCIAL-SHAREALIKE 4.0
INTERNATIONAL International License.